Demographics, Clinical Profiles, and Outcomes of Patients With Adrenal Disorders in a Tertiary Care Center: A Retrospective Study
Tufeel Ahmad Khan, Firdous Ahmad Beigh, Abdul Rouf Khawaja, Sajad A Malik, Sajjad A Para, Saqib Mehdi, Arif Hamid, Saundarya Kumar Verma, Mudasir Ahmad Tantray

TL;DR
This study examines adrenal mass patients in India, finding pheochromocytoma is common and larger tumors are more likely to be malignant.
Contribution
The paper provides demographic and clinical insights into adrenal disorders in a South Asian population, emphasizing management strategies and diagnostic challenges.
Findings
Pheochromocytoma was the most common functional tumor (39.58% of cases).
Laparoscopic adrenalectomy resulted in shorter hospital stays compared to open surgery.
Tumor size greater than 4 cm was significantly associated with malignancy.
Abstract
Background: Adrenal masses encompass a spectrum from benign incidentalomas to malignant tumors, posing diagnostic and therapeutic challenges due to their varied clinical presentations and histopathological characteristics. The increased use of imaging has led to detection rates, necessitating detailed studies to guide management strategies in diverse populations. Objective: This study evaluates the demographic, clinical, pathological, and outcome profiles of patients with adrenal masses managed at a tertiary care center in Srinagar, India, highlighting complex cases to illustrate diagnostic and treatment intricacies. Methods: We analyzed 48 patients with adrenal masses at Sher-i-Kashmir Institute of Medical Sciences (SKIMS), Srinagar, from January 2021 to December 2024. Data, retrospectively collected from electronic records of patients referred to Urology, included demographics,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
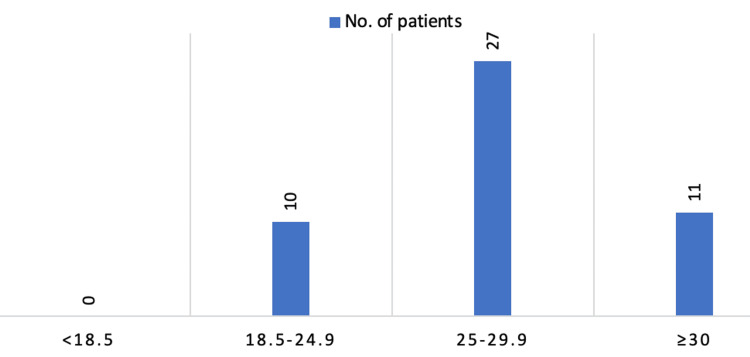 Figure 1
Figure 1 Figure 2
Figure 2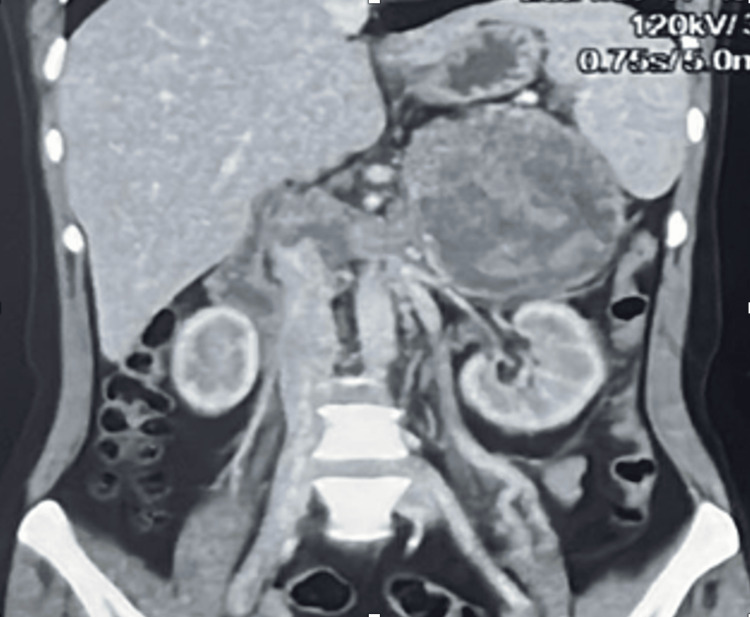 Figure 3
Figure 3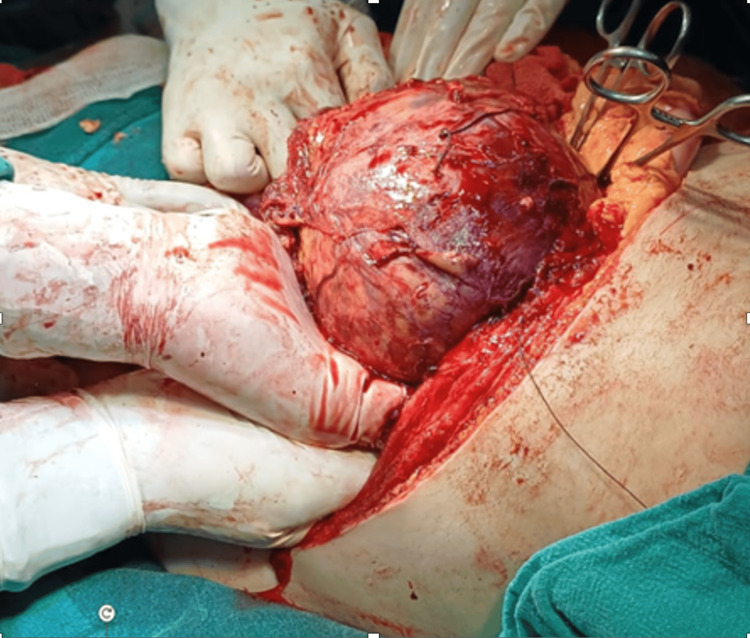 Figure 4
Figure 4 Figure 5
Figure 5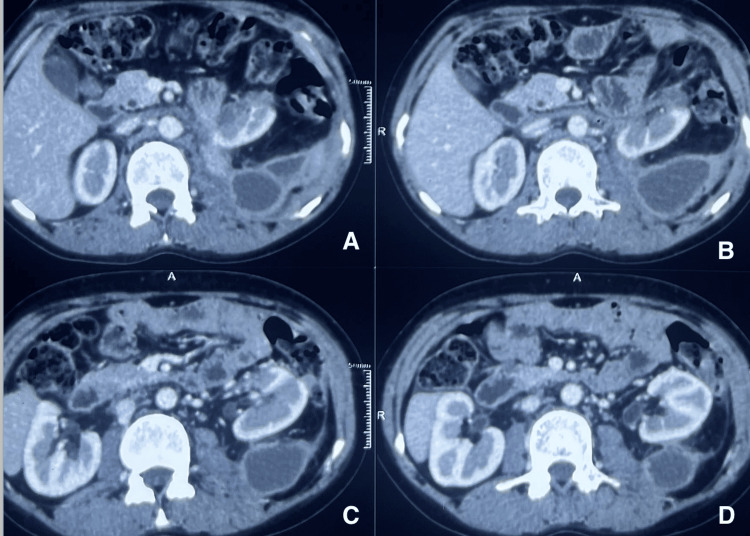 Figure 6
Figure 6 Figure 7
Figure 7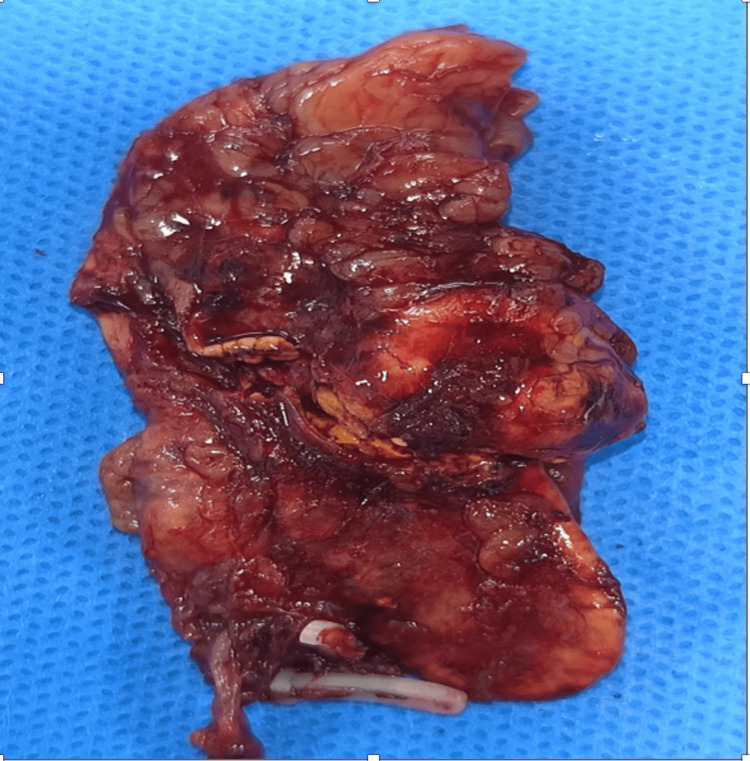 Figure 8
Figure 8| Age (Years) | Total Number of Patients n (%). |
| A (10-20) | 2 (4.17) |
| B (21-30) | 7 (14.58) |
| C (31-40) | 12 (25.00) |
| D (41-50) | 12 (25.00) |
| E (51-60) | 9 (18.75) |
| F (61-70) | 6 (12.50) |
| Total | 48 (100%) |
| Presentations/Symptoms | Total Number of Patients n (%). |
| Incidental mass | 23 (47.92) |
| Localized symptoms | 13(27.08) |
| Symptoms of hormonal excess | 9 (18.75) |
| Resistant hypertension | 2 (4.17) |
| Cancer screening | 1 (2.08) |
| Total | 48 |
| Parameter | Value |
| Demography | |
| Male n (%) | 18 (37.5) |
| Female n (%) | 30 (62.5) |
| Median age of presentation (years) | 45 (13-65) |
| Modality of presentation n (%) | |
| Incidental discovery | 21 (43.75) |
| Local symptoms (pain/mass) | 13 (27.08) |
| Symptoms of hormonal access | 9 (18.75) |
| Drug resistant/severe HTN | 2 (4.17) |
| Cancer surveillance or staging | 1 (2.08) |
| Functional status n (%) | |
| Functional | 26 (54.16) |
| Non-functional | 22 (45.83) |
| Past or current medical history of extra-adrenal malignancy | |
| Yes | 4 (8.33) |
| unknown | 24(91.67) |
| Mass Location | Value |
| Left | 26 (54.17) |
| Right | 21 (43.75) |
| bilateral | 1 (2.08) |
| Number of lesions | |
| Single | 46 (95.83) |
| Multiple | 2 (4.17) |
| Size of lesion (cm) | |
| Maximum diameter | 14 |
| Mean diameter | 5.6 |
| Size <= 4 | 22 (42.85) |
| Size > 4 | 26 (54.16) |
| 4-6 | 17 (35.42) |
| >6 | 9 (18.75) |
| Unenhanced CT mass attenuation | |
| Median CT attenuation (HU) | 10 |
| <= 10HU n (%) | 12 (25) |
| 11-20 HU n (%) n (%) | 8 (16.67) |
| >20 HU n (%) | 7 (14.58) |
| Heterogeneous n (%) | 8 (16.67) |
| Unknown n (%) | 13 (27.08) |
| Tumor Size (cm) | Number of Patients n(%) |
| < 4 | 22 (45.83) |
| 4-6 | 17 (35.42) |
| >6 | 9 (18.75) |
| Mean tumor size (cm) | 5.6 |
| Surgical Technique | Value |
| Lap. adrenalectomy n (%) | 22 (45.83) |
| Open adrenalectomy n (%) | 20 (41.67) |
| HPE (42 operated cases) | |
| Adenoma (non-functional) n (%) | 9(18.75) |
| Myelolipoma n (%) | 4(8.33) |
| Pheochromocytoma n (%) | 19(39.58) |
| Cushing's adenoma n (%) | 5(10.42) |
| Adrenocortical cancer (ACC) n (%) | 1(2.08) |
| Cons adenoma | 1(2.08) |
| Ganglioneuroma | 1 (2.08) |
| Schwannoma | 1 (2.08) |
| Paraganglioma | 1(2.08) |
| Association Tested | Statistical Test | Test Statistic | p-Value | Result | Interpretation |
| Tumor Size and Malignancy | Chi-square test | χ² = 2.62 | 0.03 | Significant association; 3/26 (11.54%) tumors >4 cm malignant vs. 0/22 (0%) ≤4 cm | Tumors >4 cm are more likely to be malignant, supporting surgical intervention for larger lesions. Limited generalizability due to a small malignant case number (n=1). |
| Functional Status and Gender | Chi-square test | χ² = 0.57 | 0.45 | No significant association; 16/30 (53.33%) female patients and 10/18 (55.56%) male patients with functional tumors | Hormonal activity of tumors is not influenced by gender in this cohort. |
| Functional Status and Tumor Side | Chi-square test | χ² = 0.24 | 0.62 | No significant association; functional tumors in 14/26 (53.85%) left-sided, 11/21 (52.38%) right-sided, 1/1 (100%) bilateral | Tumor laterality does not influence functional status in this cohort. |
| Age Distribution and Functional Status | Mann-Whitney U test | U = 238 | 0.32 | No significant difference; median age 38 years (functional) vs. 42 years (non-functional) | Age does not significantly affect tumor functional status in this cohort. |
| BMI and Tumor Size | Spearman correlation | r = 0.12 | 0.41 | No significant correlation between BMI and tumor size categories | Overweight status (median BMI 27.5 kg/m²) does not directly influence tumor size in this sample. |
| Presentation Modality and Functional Status | Chi-square test | χ² = 10.45 | 0.03 | Significant association; hormonal symptoms in 7/9 (77.78%) functional tumors vs. 10/23 (43.48%) incidental findings | Hormonal symptoms are more common in functional tumors, highlighting symptomatology’s role in identifying active lesions. |
| Blood Loss by Surgical Technique | Mann-Whitney U test | U = 230 | 0.9197 | Median blood loss: 150 mL (range 100–300 mL) for both laparoscopic (n=22) and open (n=20) adrenalectomies | No significant difference in blood loss between laparoscopic and open procedures. |
| Hospital Stay by Surgical Technique | Chi-square test | χ² = 6.10 | 0.014 | Mean hospital stay: 2.5 days (laparoscopic) vs. 3.8 days (open) | Laparoscopic adrenalectomy is associated with a shorter hospital stay (by 1.3 days) compared to open adrenalectomy, is significant. |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAdrenal and Paraganglionic Tumors · Hormonal Regulation and Hypertension · Adrenal Hormones and Disorders
Introduction
Adrenal glands are present above the kidneys and orchestrate critical physiological functions through their cortical (producing mineralocorticoids, glucocorticoids, and sex hormones) and medullary (secreting catecholamines) regions. Enhanced imaging technologies have escalated the detection of adrenal masses, with prevalence rates of 3-7% in adults, increasing to 6% beyond age 60 [1,2]. Although most adrenocortical tumors (75-90%) are benign, 2-10% are malignant, and 30-60% exhibit hormonal activity, manifesting as hypertension, Cushing’s syndrome, or hyperaldosteronism [1,3]. This study explores the clinical characteristics, treatment strategies, and outcomes of 48 adrenal tumor patients managed at SKIMS, including two exemplary cases that underscore diagnostic and therapeutic complexities.
Materials and methods
This retrospective analysis included 48 patients with adrenal masses managed at SKIMS from January 2021 to December 2024. We retrospectively collected data from electronic records of all consecutive patients with adrenal masses referred to the department of Urology from January 2021 to December 2024. Data included both the referral patients to the department for surgical intervention and the first contact patients presented to OPD with incidentally detected masses. Collected data encompassed patient demographics, clinical symptoms, imaging findings (via ultrasound and contrast-enhanced CT (CECT)), hormonal assessments (including plasma cortisol, serum aldosterone, 24-hour urinary metanephrines, and dexamethasone suppression tests), surgical details, histopathological results, and follow-up outcomes.
A multidisciplinary team (urologists, endocrinologists, anesthesiologists, radiologists, pathologists) guided patient care. Preoperative assessments included electrolytes, ultrasound, and CECT. Hormonal evaluation guided management: functional tumors and non-functional >6 cm underwent adrenalectomy; non-functional <4 cm monitored (imaging every six months) if low-risk, surgical if high-risk; 4-6 cm based on malignancy-suggestive CT features (e.g., >20 HU, heterogeneity). Pheochromocytomas received alpha-blockers (prazosin 5-10 mg) and beta-blockers (propranolol) preoperatively. Surgical techniques used were laparoscopic or open adrenalectomy; intraoperative BP control was done with sodium nitroprusside/nitroglycerin for pheochromocytomas.
Two cases were selected to highlight challenges. Analysis used descriptive statistics (means, medians, percentages), Fisher's exact/chi-square tests, Mann-Whitney U, Spearman correlation for associations (e.g., size vs. malignancy) using IBM SPSS Statistics for Windows, Version 25 (Released 2017; IBM Corp., Armonk, New York, United States). SKIMS Ethics Committee approved the study; written consent was obtained.
Patient selection
The inclusion criteria for this retrospective study encompassed all patients who presented with adrenal masses and were managed at the Sher-i-Kashmir Institute of Medical Sciences in Srinagar, Jammu and Kashmir, India, during the period from January 2021 to December 2024.
Patients with incomplete or unavailable medical records, including essential diagnostic, treatment, or follow-up data and patients who did not provide written informed consent were excluded from the study
Results
Gender and age
The study cohort comprised 48 patients, with 30 female patients (62.5%) and 18 male patients (37.5%), and a median age of 45 years (range 13-65 years) (Table 1).
Presentation
Clinical presentations are shown in Table 2.
BMI
Median BMI was 27.5 kg/m² (range 22-32 kg/m²), indicating a slight overweight tendency and none of the patients had a BMI < 18.5 (Figure 1).
BMI distribution in the study
Functional status
Hormonal evaluations identified 26 (54.16%) functional and 22 (45.83%) non-functional tumors. Functional tumors included pheochromocytoma (19, 39.58%), Cushing's adenoma (5, 10.42%), Conn's adenoma (1, 2.08%), and paraganglioma (1, 2.08%).
Preoperative parameters
All preoperative parameters are presented in Table 3.
Radiological characteristics
Imaging revealed 26 (54.17%) left-sided and 21 (43.75%) right-sided adrenal masses and one (2.08%) bilateral adrenal mass. Ninety-four percent of patients had a single lesion and 6% patients had more than one lesion on one side.
Tumor sizes included 26 patients (54.17%) with >4 cm (median 7.2 cm, range 4.5-14 cm) and 22 (45.83%) with ≤4 cm (median 2.8 cm, range 2.1-4 cm) (Tables 4, 5).
CT attenuation values were available for 35 patients (72.92% patients) with median CT attenuation of 10 HU.
Histopathology of the 42 surgical cases is shown in Table 6. Six non-operative patients were labelled as adenoma based on CT findings and were managed conservatively by serial imaging. All had a size of < 4 cm (Table 6).
Operative and post-operative parameters
Surgical intervention occurred in 42 patients (87.50%), with 22 (52.38%) laparoscopic and 20 (47.62%) open adrenalectomies. Laparoscopic procedures averaged 120 minutes (range 90-180), while open procedures averaged 110 minutes (range 95-170) (Table 6).
Median blood loss was 150 mL (range 100-300 mL). Postoperative hospital stays averaged 2.5 days (100% of laparoscopic cases within 2-7 days) for laparoscopic adrenalectomy and 3.8 days (100% of open cases within 3-8 days) for open adrenalectomy. Complications included one splenectomy (2.08%) due to splenic vein injury and one patient with IVC thrombus in whom IVC thrombectomy was done (2.08%) (Case 1). Fourteen patients (29.17%) with non-functional tumors <4 cm were monitored with serial imaging and hormonal tests. No perioperative deaths occurred. Four patients (8.33%) had concurrent extra-adrenal malignancies: three renal cell carcinomas (6.25%) and one lung cancer (2.08%).
Statistical analysis
Data analysis was conducted using IBM SPSS Statistics for Windows, Version 25 (Released 2017; IBM Corp., Armonk, New York, United States), employing descriptive statistics to summarize demographic, clinical, radiological, and histopathological characteristics. Continuous variables, such as age, BMI, tumor size, CT attenuation values, intraoperative time, and hospital stay, were expressed as medians with ranges or means with standard deviations where appropriate. Categorical variables, including gender, presentation modality, functional status, lesion location, number of lesions, tumor size categories, and histopathological diagnoses, were presented as frequencies and percentages.
To assess associations, chi-square tests were utilized for larger sample subgroups, while Fisher's exact test was applied for smaller expected frequencies (<5) to ensure accuracy. The following key associations were examined:
Tumor Size and Malignancy
A chi-square test indicated a significant association between tumor size >4 cm and malignancy (χ² = 2.62, p=0.03), with 3/26 (11.54%) tumors >4 cm classified as malignant compared to 0/22 (0%) tumors ≤4 cm. This finding supports the clinical threshold for surgical intervention in larger lesions, though the small number of malignant cases (n=1 adrenocortical carcinoma (ACC) in the cohort) limits generalizability.
Functional Status and Gender
No significant association was found between functional status and gender (χ² = 0.57, p=0.45), with functional tumors distributed as 16/30 (53.33%) in female patients and 10/18 (55.56%) in male patients. This suggests that hormonal activity is not influenced by gender in this cohort.
Functional Status and Tumor Side
Similarly, no significant association was observed between functional status and tumor laterality (χ² = 0.24, p=0.62), with functional tumors occurring in 14/26 (53.85%) left-sided, 11/21 (52.38%) right-sided, and 1/1 (100%) bilateral cases.
Age Distribution and Functional Status
The median age did not differ significantly between functional (median 38 years) and non-functional (median 42 years) groups (Mann-Whitney U test, p=0.32), indicating no age-related bias in tumor activity.
BMI and Tumor Size
BMI showed no significant correlation with tumor size categories (Spearman r = 0.12, p=0.41), suggesting that overweight status (median BMI 27.5 kg/m²) does not directly influence lesion dimensions in this sample.
Presentation Modality and Functional Status
Chi-square analysis revealed a significant association between presentation modality and functional status (χ² = 10.45, p=0.03), with hormonal symptoms more common in functional tumors (7/9, 77.78%) compared to incidental findings (10/23, 43.48%), highlighting the role of symptomatology in identifying active lesions.
Complications and Surgical Technique
Fisher's exact test showed no significant difference in complication rates between laparoscopic and open approaches (p=0.89), with each group experiencing one complication (splenectomy in laparoscopic, IVC thrombectomy in open).
Mean Tumor Size
The mean tumor size is 5.6 cm (SD 2.4 cm, range 2.1-14 cm).
Median Intraoperative Time
The median intraoperative time is 120 minutes (laparoscopic 130 minutes, open 110 minutes).
Median Hospital Stay
The median hospital stay is 3.15 days (laparoscopic 2.5 days, open 3.8 days).
Median CT Attenuation
The median CT attenuation is 10 HU (range 5-35 HU among assessed cases)
Mean Hospital Stay
The mean hospital stay is 2.5 days (laparoscopic) vs. 3.8 days (open). Laparoscopic adrenalectomy is associated with a shorter hospital stay (by 1.3 days) compared to open adrenalectomy, is significant.
Statistical associations tested in the adrenal tumor cohort: tests, results, and interpretations are presented in Table 7.
Illustrative cases
Case 1 (Adrenocortical Carcinoma with IVC Thrombus)
This case report delineates the clinical journey of a 31-year-old female patient who presented with a triad of symptoms: bilateral lower limb swelling persisting for 20 days, chronic left flank pain enduring for one and a half months, and the emergence of facial hair over a three-month period. Comprehensive diagnostic workup, encompassing contrast-enhanced computed tomography (CT) and hormonal profiling, identified a 14109cm left adrenal mass with an associated thrombus extending through the renal vein into the inferior vena cava (IVC) (Figures 2, 3). Laboratory analysis revealed elevated morning serum cortisol (680 nmol/L, normal <450 nmol/L) and testosterone (3.2 nmol/L, normal <2.5 nmol/L) levels, indicative of a hormonally active adrenal neoplasm, likely ACC. The patient underwent a meticulously orchestrated surgical intervention involving a left adrenalectomy and IVC thrombectomy, with a deliberate effort to preserve the left kidney to sustain renal function (estimated glomerular filtration rate (eGFR) 90 mL/min/1.73m²). The procedure, executed via an open surgical technique at the Sher-i-Kashmir Institute of Medical Sciences (SKIMS), Srinagar, under the guidance of a multidisciplinary team comprising endocrinologists, urologists, anesthetists and cardiovascular surgeons, successfully excised the adrenal mass and thrombus. Intraoperative findings corroborated the presence of a solid mass (Figures 4, 5) and postoperative histopathological examination confirmed ACC with vascular invasion (Weiss score 5). Postoperative management incorporated anticoagulation with rivaroxaban and hydrocortisone supplementation to address adrenal insufficiency. The patient’s recovery was unremarkable, discharged on 5th POD and there were no complications at two-week postoperative follow-up. A post-op CT scan at 12 weeks showed no residual or recurrent lesion seen in the kidney, bland thrombus seen in left Renal vein and IVC with no e/o malignant thrombus seen (Figure 6). Her symptoms as well as hirsutism settled (Figure 7), and the patient was put on medical oncology follow-up as well. At one-year follow-up, she is doing well and not on any medications, her serum creatinine is 1.22 mg/dL and has normal contrast uptake and enhancement in both kidneys with no evidence of metastasis on computed tomography (CECT) images.
Case 1: left ACC with IVC thrombus (axial view)ACC: Adrenocortical cancer
Case 1: left ACC with IVC thrombus (coronal view)ACC: Adrenocortical cancer
Case 1: intraoperative image revealing a large tumor delivered from the wound
Case 1: resected left adrenalectomy (replaced by tumor) specimen
Case 1: post-op CT (12wks) showing a well-perfused left kidney (axial view)Panels A, B, C & D showing a well-perfused left kidney, with a loculated collection in the renal bed (A, B, C & D). The collection was managed conservatively (pigtail drainage).
Case 1: pre-op (A) and 12-week post-op (A) images of the patient, with disappearance of facial hair post surgery
This case underscores the pivotal role of a collaborative multidisciplinary approach in managing rare adrenal pathologies complicated by vascular thrombosis. It also accentuates the viability of kidney preservation in complex surgical settings. The report enriches the existing literature by emphasizing the importance of thorough preoperative planning, advanced surgical methodologies, and the necessity for extended follow-up to monitor potential recurrence, given the aggressive propensity of ACC. Future investigations are imperative to enhance therapeutic modalities and prognostic frameworks for patients with analogous clinical presentations.
Case 2 (Aldosterone-Secreting Adenoma)
A 35-year-old man with chronic hypertension (160/100 mmHg) presented with acute quadriparesis. Tests revealed severe hypokalemia (1.09 meq/L), acute kidney injury (creatinine 3.56 mg/dL), and an aldosterone/renin ratio of 11.8. CT confirmed a 20x17 mm left adrenal adenoma. Laparoscopic adrenalectomy was performed, specimen removed (Figure 8), with histopathology verifying an aldosterone-producing adenoma. Potassium levels normalized (4.16 meq/L) by day 2 post-surgery. The patient had a smooth postoperative course and had no symptoms up to 24 months of follow up.
Case 2: resected adrenalectomy specimen
Discussion
The retrospective analysis of 48 adrenal tumor patients at the Sher-i-Kashmir Institute of Medical Sciences (SKIMS) provides a detailed perspective on the clinical management of adrenal masses within a tertiary care environment, reflecting both global trends and unique regional characteristics. The cohort demonstrated a marked female predominance (62.5%), consistent with prior research suggesting that increased imaging utilization among women or hormonal influences may contribute to higher detection rates [1].
The median age of 45 years is significantly lower than the 50-60 years typically observed in Western populations [2], potentially indicating earlier disease onset, regional genetic predispositions, or differences in healthcare access and referral patterns in this resource-limited setting. This age discrepancy merits further exploration into environmental or genetic factors, such as potential mutations in VHL or RET genes, which are known to affect younger individuals [3].
The high prevalence of incidentalomas (47.92%) aligns with international estimates of 5-7% in adults, a trend driven by the widespread adoption of cross-sectional imaging [4]. This highlights the contemporary challenge of managing clinically silent adrenal lesions, necessitating meticulous differentiation between benign and malignant entities. The cohort also included 27.08% of patients with localized symptoms, such as flank pain or palpable masses, and 18.75% with hormonal symptoms, including hypertension or Cushingoid features, which are within the expected 30-60% range of functional tumors reported in the literature [5]. The median BMI of 27.5 kg/m², reflecting a slight overweight tendency, may suggest a metabolic link to adrenal pathology, as obesity has been associated with an elevated incidence of adrenal incidentalomas in some studies [6]. Functional status assessment revealed a predominance of non-functional tumors (66.67%), consistent with the 70-85% reported in larger cohorts [7]. However, the notable presence of pheochromocytoma (39.58% of the cohort, 62.5% of functional cases) diverges from European data, where cortisol-secreting adenomas are more prevalent [5]. This regional variation could indicate a higher incidence of catecholamine-secreting tumors in South Asian populations, potentially linked to genetic predispositions such as SDHB or SDHD mutations, which are associated with pheochromocytoma and paraganglioma [8]. The absence of genetic testing in this study restricts etiological understanding, a limitation also observed in other resource-constrained environments [9]. Radiological findings showed a left-sided predominance (54.17%), a pattern occasionally noted due to anatomical or imaging biases [10]. The vast majority of lesions were single (95.83%), aligning with typical adrenal tumor presentations [11].
Tumor size distribution, with 54.17% exceeding 4 cm, supports clinical guidelines recommending surgical intervention for larger masses due to heightened malignancy risk [7]. The median CT attenuation of 10 Hounsfield Units (HU), with 25% ≤10 HU suggestive of adenomas, corresponds with established diagnostic criteria for benign lesions [12]; however, 27.08% of cases with unknown attenuation values pose a significant barrier to non-invasive characterization. Surgical intervention was performed in 87.50% of patients, with a preference for laparoscopic adrenalectomy (52.38%), reflecting a global shift toward minimally invasive approaches. This technique resulted in a reduced postoperative hospital stay (2.5 days for laparoscopic versus 3.8 days for open procedures), a benefit supported by literature indicating shorter recovery times and decreased morbidity [13]. Intraoperative durations averaged 130 minutes for laparoscopic and 110 minutes for open procedures, with a median blood loss of 150 mL, both within acceptable ranges for adrenal surgery [14]. Complications, including one splenectomy and one IVC thrombectomy (2.08% each), highlight the complexity of certain cases, with conversion rates of 5-10% reported in challenging laparoscopic scenarios [15].
Histopathological analysis identified pheochromocytoma as the predominant diagnosis (52.08%), reinforcing the regional trend, followed by adenoma (29.17%), with rarer entities such as myelolipoma (8.33%), ganglioneuroma (2.08%), schwannoma (2.08%), and paraganglioma (2.08%) contributing to the diversity. ACC (2.08%) and Conn's disease (2.08%) occurred at lower frequencies, consistent with their reported incidences of 2-10% and 5-10%, respectively [16,17]. The significant association between tumor size >4 cm and malignancy (p=0.03), with 11.54% of larger tumors being ACCs, supports evidence linking size to cancer risk [7]. The absence of significant associations between functional status and gender (p=0.45) or tumor side (p=0.62) suggests that these factors do not reliably predict tumor behavior, a finding echoed in varied studies [18].
ACC with IVC thrombus exemplifies a rare and aggressive presentation. The successful kidney-preserving surgery, despite tumor adherence to adjacent structures, underscores the value of multidisciplinary expertise, achieving survival rates exceeding 60% for localized disease with adjuvant therapies like radiation [19]. The 12-week follow-up without recurrence is promising, and as the patient is still on follow-up, it should be continued as per the recommended five-year surveillance period, given the 20-40% recurrence risk for ACC [7]. Aldosterone-producing adenoma causing quadriparesis due to severe hypokalemia also represents a rare manifestation (<10% of primary aldosteronism cases), emphasizing the importance of timely hormonal diagnosis. The rapid postoperative normalization of potassium levels and 90-95% success rate following laparoscopic adrenalectomy validate surgery as the definitive treatment [20]. The low complication rate (2.08% for splenectomy and IVC thrombectomy) is consistent with reported conversion rates of 5-10% in complex laparoscopic cases, highlighting the need for skilled surgical teams [14].
The 8.33% incidence of concurrent extra-adrenal malignancies (6.25% renal cell carcinomas, 2.08% lung cancer) underscores the necessity for comprehensive staging, as adrenal metastases are a frequent secondary finding in oncology patients [21]. The absence of advanced imaging modalities like PET-CT limited metastatic evaluation, a common constraint in resource-limited settings. Similarly, incomplete biochemical profiling, such as limited dexamethasone suppression tests for subclinical Cushing’s syndrome, impedes accurate functional assessment, a critical aspect of adrenal tumor management [9]. The lack of genetic screening is particularly significant, given that 10-20% of pheochromocytomas and ACCs are associated with hereditary syndromes like multiple endocrine neoplasia type 2 or Li-Fraumeni syndrome [3]. The follow-up period, ranging from 2 to 4 years with an average of 3.5 years, offers a more substantial observation window than the initial 12-24 months, yet it remains insufficient for detecting long-term recurrence risks, particularly for malignancies requiring five-year monitoring [7]. Future research should prioritize standardized diagnostic protocols, incorporating comprehensive hormonal assays (e.g., 1 mg overnight dexamethasone suppression test, plasma metanephrines) and genetic testing to identify hereditary syndromes. Multicenter studies could validate these findings across diverse populations, while national registries would support long-term outcome tracking. The integration of advanced imaging techniques, such as MRI or PET-CT, could improve diagnostic accuracy for indeterminate lesions [22].
Limitations of the study
This retrospective study, while providing valuable insights into adrenal tumor management at a single tertiary care center in a resource-limited setting like the Sher-i-Kashmir Institute of Medical Sciences in Srinagar, is subject to several limitations that warrant caution in interpreting its findings. The retrospective design inherently introduces risks of selection bias, recall bias, and incomplete data collection, which undermine the ability to establish causality compared to prospective studies. The relatively small cohort of 48 patients further restricts statistical power, limiting the detection of rare events, subtle associations, and generalizability, particularly evident in the analysis of malignancy risks, where only one confirmed case of ACC was identified. Conducted exclusively at one institution, the results may not reflect broader populations, potentially influenced by regional referral patterns, genetic predispositions, or environmental factors, such as the unusually high prevalence of pheochromocytoma and a younger median age (40-45 years) compared to Western cohorts, which were not thoroughly investigated. Diagnostic assessments were hampered by incomplete hormonal evaluations in 13 (27.08%) cases, including limited dexamethasone suppression tests for subclinical Cushing's syndrome, as well as the absence of genetic screening for hereditary syndromes (e.g., VHL, RET, SDHB/SDHD mutations), restricting etiological understanding. Reliance on basic imaging modalities like ultrasound and contrast-enhanced CT, without advanced tools such as PET-CT or MRI, further impeded metastatic evaluation and non-invasive lesion characterization, compounded by unavailable CT attenuation values in 27.08% of patients. The follow-up period, ranging from 24-48 months with an average of 3.5 years, falls short of the recommended five-year surveillance for malignancies like ACC, potentially underestimating long-term recurrence risks. Finally, the lack of standardized protocols and advanced therapies in this resource-constrained environment may not mirror outcomes in better-equipped settings, highlighting the need for larger, multicenter prospective studies to validate and expand upon these observations.
Conclusions
In this retrospective study of 48 patients with adrenal masses at SKIMS (2021-2024), functional tumors were predominant, with pheochromocytoma being the most common. Laparoscopic adrenalectomy showed shorter hospital stays and lower complications. Larger tumors trended toward malignancy, though limited by small sample size. Functional tumors correlated with hormonal symptoms. The study highlights effective multidisciplinary management in a resource-limited setting, with cases like ACC and Conn’s adenoma showing good outcomes. Limitations include retrospective design, a small cohort, and short follow-up. Larger, prospective studies are needed to refine regional patterns and protocols.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Medical and surgical evaluation and treatment of adrenal incidentalomas J Clin Endocrinol Metab Zeiger MA Siegelman SS Hamrahian AH 20042015962011 https://doi.org/10.1210/jc.2011-00852163281310.1210/jc.2011-0085 · doi ↗ · pubmed ↗
- 2Clinical practice. The incidentally discovered adrenal mass N Engl J Med Young WF Jr 6016103562007 https://doi.org/10.1056/NEJ Mcp 0654701728748010.1056/NEJ Mcp 065470 · doi ↗ · pubmed ↗
- 3von Hippel-Lindau disease: a clinical and scientific review Eur J Hum Genet Maher ER Neumann HP Richard S 617623192011 https://doi.org/10.1038/ejhg.2010.1752138687210.1038/ejhg.2010.175PMC 3110036 · doi ↗ · pubmed ↗
- 4The clinically inapparent adrenal mass: update in diagnosis and management Endocr Rev Mansmann G Lau J Balk E Rothberg M Miyachi Y Bornstein SR 309340252004 https://doi.org/10.1210/er.2002-00311508252410.1210/er.2002-0031 · doi ↗ · pubmed ↗
- 5AME position statement on adrenal incidentaloma Eur J Endocrinol Terzolo M Stigliano A Chiodini I 8518701642011 https://doi.org/10.1530/EJE-10-11472147116910.1530/EJE-10-1147 · doi ↗ · pubmed ↗
- 6Clinical characteristics and metabolic features of patients with adrenal incidentalomas with or without subclinical Cushing's syndrome Endocrinol Metab (Seoul) Kim BY Chun AR Kim KJ Jung CH Kang SK Mok JO Kim CH 457463292014 https://doi.org/10.3803/En M.2014.29.4.4572532526410.3803/En M.2014.29.4.457PMC 4285048 · doi ↗ · pubmed ↗
- 7Management of adrenal incidentalomas: European Society of Endocrinology Clinical Practice Guideline in collaboration with the European Network for the Study of Adrenal Tumors Eur J Endocrinol Fassnacht M Arlt W Bancos I 01752016 https://doi.org/10.1530/EJE-16-046710.1530/EJE-16-046727390021 · doi ↗ · pubmed ↗
- 8Phaeochromocytoma Lancet Lenders JW Eisenhofer G Mannelli M Pacak K 6656753662005 https://doi.org/10.1016/S 0140-6736(05)67139-51611230410.1016/S 0140-6736(05)67139-5 · doi ↗ · pubmed ↗