Leaving the health workforce during the COVID-19 pandemic: A cross-sectional study among Filipino healthcare workers
Christl Jan S. Tiu, Nicole Rose I. Alberto, Maria Beatriz C. Baron, Michael Vincent V. Mercado, Ronnie E. Baticulon, Padmasayee Papineni, Padmasayee Papineni

TL;DR
This study explores why Filipino healthcare workers left their jobs during the pandemic, highlighting burnout, stress, and low pay as key factors.
Contribution
The study provides insights into the specific reasons for healthcare worker attrition in the Philippines during the early stages of the pandemic.
Findings
Most healthcare workers cited work overload, burnout, and stress as reasons for quitting.
Low salary and insufficient compensation were frequently mentioned as contributing factors.
Participants proposed solutions like better pay, reduced workload, and improved workplace safety to retain workers.
Abstract
The COVID-19 pandemic exacerbated the shortage of healthcare workers (HCWs), particularly in low- and middle-income countries. This cross-sectional descriptive study aimed to examine why hospital-based HCWs in the Philippines quit from their workplace at a time when HCWs were urgently needed to provide health services. Using an online, self-administered questionnaire distributed through personal and professional networks, we surveyed hospital-based Filipino HCWs who resigned between March 11, 2020, and September 15, 2021. We obtained demographics, workplace information, reasons for quitting, and proposed interventions. Among 70 valid responses, most of the HCWs were single (74%), female (59%), and without children (81%). More than half were nurses (31%) and physicians (29%). Most participants had one to five years of work experience (71%), worked in level 3 hospitals (70%), and had a…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
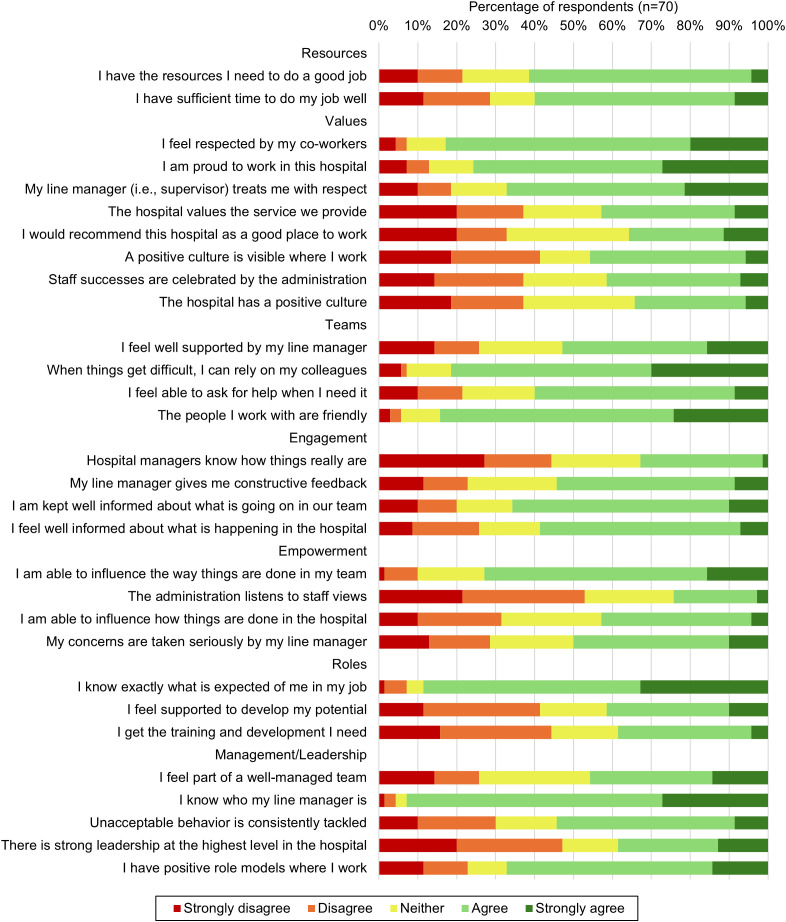 Fig 1
Fig 1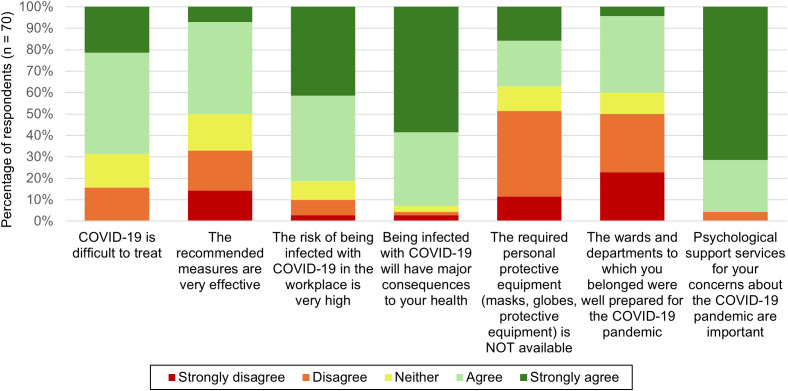 Fig 2
Fig 2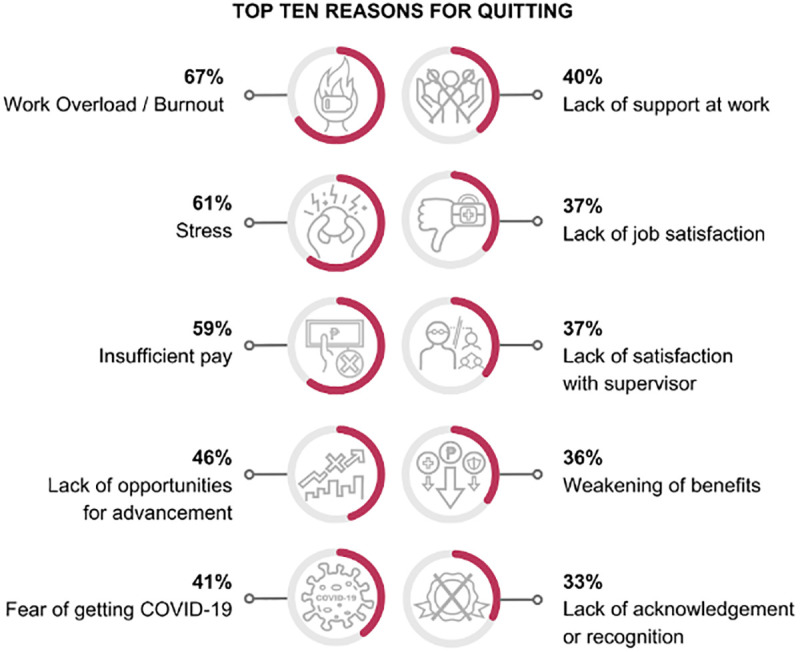 Fig 3
Fig 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHealthcare professionals’ stress and burnout · COVID-19 and Mental Health · COVID-19 and healthcare impacts
Introduction
The World Health Organization (WHO) reported that the COVID-19 pandemic worsened the preexisting shortage of healthcare workers (HCWs) globally, especially in low- and middle-income countries [1–3]. The Philippines is a lower-middle income country in Southeast Asia (Total population: 117 million in 2023 [4]) widely known for training HCWs, many of whom migrate to other countries [5–8]. This has resulted in chronic shortage of HCWs locally [8–10] despite many efforts to augment the health workforce, such as return service agreements where aspiring health professionals can avail of educational incentives and scholarships in exchange of working locally for at least 3 years [11–13]. In 2021, there were an estimated 7.9 doctors and 47.5 nurses and midwifery personnel for every 10,000 people in the Philippines [14]. Although the recent figures have surpassed the WHO-recommended threshold of 45 skilled health workers for every 10,000 people [15], most of the country’s health workforce remains concentrated in cities and urban areas [9].
Many studies that had previously described the attrition of the health workforce during the COVID-19 pandemic focused on turnover intention [16,17]. Turnover intention, often used interchangeably with intention to leave, is defined as the individual’s willingness to leave their current employment for a different position in the same or different profession [18–20]. During the pandemic, commonly cited reasons why HCWs considered leaving their workplace were related to moral distress. Examples of these include increased workload despite being short-staffed, insufficient personal protective equipment, allocation of scarce resources, fear of spreading COVID-19 to loved ones, and lack of organizational or government support [17]. Fear of COVID-19 was noted to be prevalent in both international and local studies [16,17,21,22]. To our knowledge, there is no published study that has documented the profiles and circumstances of HCWs who ultimately resigned.
In this paper, we aimed to describe the sociodemographic characteristics and work circumstances of Filipino HCWs who resigned from their hospital-based employment during the acute phase of the COVID-19 pandemic. Understanding the underlying reasons of HCWs who resigned can provide valuable insights for ministries of health, policymakers, public and private health administrators, third-party payers, and health worker unions, who must work together to encourage workforce retention and ensure continuity of health services during national and global health crises.
Methods
Ethics statement
The University of the Philippines Manila Research Ethics Board granted ethical approval (UPMREB Code 2021-523-01). Informed consent was obtained in the initial section of the online, self-administered, survey questionnaire.
This is a cross-sectional descriptive study using an online, self-administered survey in GoogleForms (Google LLC, Mountain View, California). We adhered to the Checklist for Reporting Results of Internet E-Surveys (S1 Checklist).
We defined HCWs as individuals who provide professional, health-related services to patients. These include physicians, nurses, occupational therapists, physical therapists, respiratory therapists, speech pathologists, pharmacists, medical technologists, and radiologic technologists, among others. For this study, we recruited those who had worked for at least one year and resigned from their hospital-based employment between March 11, 2020 and September 15, 2021, which covered the Alpha and Delta waves of the COVID-19 pandemic in the Philippines. The study excluded HCWs who were on leave of absence or those who had been relieved from their positions. We collected responses from October 15 to December 30, 2021. We discontinued data collection due to a lack of new responses.
The survey questionnaire (S1 Text) collected data on the respondents’ sociodemographic characteristics, workplace information and culture, worries of HCWs during the COVID-19 pandemic, reasons for leaving their positions, and proposed interventions for retention.
To assess the workplace culture, we used the Culture of Care Barometer [23]. Although originally designed to facilitate team exploration of workplace strengths and weaknesses, we used the Culture of Care Barometer in this study to investigate the culture of the respondents’ previous workplace settings. Respondents rated items in this section using a Likert scale ranging from Strongly disagree to Strongly agree. Items were categorized into the following themes: Resources, Values, Team, Engagement, Empowerment, Role, and Management/Leadership.
To assess the degree and content of the worries of HCWs on COVID-19, including the perceived importance of psychological support, we adapted questions from a study by Sahashi et al. [24]. To explore reasons for quitting, we asked the respondents to choose reasons from a list, irrespective of priority, with an option for a free-form response. Finally, we asked the participants to describe, in a free-form response, any specific intervention that would convince them to return to work or remain as a hospital HCW during a pandemic.
We pilot-tested the survey among eight HCWs. We revised the survey questions based on feedback to improve the clarity of questions and to address potential issues in question construction. We distributed the revised survey questionnaire through social media platforms including Twitter, Facebook, and Instagram. We reached out to both personal networks and professional organizations to distribute the survey link among their connections (S1 List). Participation in the survey was open to all healthcare professionals with a registered email address. Using the first section of the online form, informed consent was obtained prior to answering the survey questionnaire. Upon completion, the participants could review their responses before submitting. Further, a copy of their responses was sent via their registered emails. All data collected were stored in the University of the Philippines Network and were only accessible to the authors.
After data collection, we exported de-identified survey responses to RStudio 2024.04.2 + 764 (Posit Software, PBC, Boston Massachusetts) for data analysis. We calculated the median and interquartile range for continuous variables and frequencies and percentages for categorical variables. Likert-scale responses were also reported as frequencies and percentages. Reasons for quitting were tabulated, creating categories as necessary for free-text responses. Finally, we conducted a thematic analysis of the proposed interventions to encourage workforce retention. Three authors independently analyzed and performed axial coding of the submitted free-text responses. Afterward, the authors convened to discuss the codes and to identify common themes, with the senior author resolving any disagreements.
Results
Survey respondents
We received a total of 78 responses, of which 70 (90%) were considered valid. Reasons for exclusion included the following: did not work in a hospital; occupation did not involve patient care; less than one year of experience as an HCW; and last day of work before March 11, 2020. Table 1 shows the sociodemographic characteristics of the survey respondents. The median age was 28 (IQR 7). Most of the participants were females (59%), single (74%), without children (81%), not the primary breadwinners of their families (71%), and had another household member contributing to the family income (80%). The most common jobs were nurses (31%) and physicians (29%). The majority had one to five years of experience in healthcare (71%). Nearly half of the respondents were from the National Capital Region (NCR, 46%).
Table 1: Sociodemographic Characteristics of Survey Respondents.
Workplace information, culture, and worries
The number of respondents who used to work in the private sector were slightly higher than those in the public sector (54% vs. 46%, respectively). There was a lack of responses from pharmacists, physical therapists, radiologic technologists, and respiratory therapists in the public sector. The majority (70%) were employed at level 3 hospitals, defined as teaching hospitals with intensive care units, a rehabilitation unit, an ambulatory surgical clinic, a dialysis unit, a blood bank, a tertiary clinical laboratory, and an imaging facility with interventional radiology [25]. The top three areas where they worked were the emergency department (23%), ward (21%), and outpatient clinic (16%). Most of the participants (75%) worked on shifts that lasted more than eight hours per day. Half (50%) had > 10 patients served per shift (S1 Table). Physical therapists had the lowest median net salary at Php 14,000 (USD 1 = Php 49.62, 2020; IQR: Php 3,088) while doctors had the highest median net salary at Php 46,000 (IQR: Php 38,500) (S2 Table). Physicians and nurses from the public sector have median salaries that are higher than their counterparts from the private sector (Php 50,000 vs. Php 18,000 for physicians and Php 26,000 vs. Php 17,000 for nurses) (S3 Table). However, the small sample size does not allow for formal statistical testing.
The Culture of Care Barometer suggested that the study respondents had a neutral to positive workplace culture, as illustrated in Fig 1. More than eighty percent of participants agreed with the statements “When things get difficult, I can rely on my colleagues”, “I feel respected by my co-workers”, and “The people I work with are friendly”.
Summary of Likert Responses on the Culture of Care Barometer.
On the other hand, almost half of the participants disagreed with the following statements: “The administration listens to staff views”, “Hospital managers know how things really are”, “There is strong leadership at the highest level in the hospital”, “I feel supported to develop my potential” and “I get the training and development I need”.
Fig 2 illustrates the Likert scale responses regarding worries about COVID-19. Most of the respondents agreed that they worried about the pandemic (90%), with the statement “risk of infection of family members and other relatives” being their primary concern (95%) (S4 Table). Less than half of the HCWs had either contracted COVID-19 themselves or had a family member that got infected. Nearly all (90%) reported having coworkers who had been infected.
Summary of Likert scale responses on worries about the COVID-19 pandemic.
Reasons for quitting
The top three reasons for quitting were work overload and burnout (67%), stress (61%), and insufficient pay (59%) (Fig 3). Most participants made the decision to quit independently, without influence from their families (59%). Nearly half of the participants had already been contemplating leaving their jobs before the pandemic, but none planned to retire from the healthcare profession before 2025. Notably, many were planning to migrate and work abroad (49%). After resigning from their original employment, only a third remained working in healthcare settings locally (36%). The other respondents transitioned to nonclinical roles (29%), remained unemployed (17%), pursued employment abroad (9%), or pursued further studies (7%).
Top Ten Reasons for Quitting.Created in BioRender. Tiu, C. (2025) https://BioRender.com/ivwgepr.
Potential interventions to promote retention
The suggested interventions to promote HCW retention could be categorized under the following themes: increased monetary compensation, enhanced non-salary incentives, positive workplace culture, reasonable workload, clear opportunities for career advancement, and improved workplace safety. Representative responses from the HCWs are shown in Table 2.
Table 2: Summary of interventions suggested to promote retention in local healthcare work.
Discussion
To our knowledge, this is the first and only study to examine the characteristics and reasons of HCWs who quit from hospital-based employment during the COVID-19 pandemic in the Philippines. Our study found that fear of COVID-19 only ranked fifth among their cited reasons for quitting. The primary reasons for leaving the health workforce were preexisting issues, particularly work overload/burnout, stress, and insufficient pay.
Fear of COVID-19 is the most prevalent theme for turnover intention among HCWs [17]. Yet, our findings suggest that while possibly contributory, being infected with COVID-19 is unlikely to be the primary reason for quitting. Notably, most of our respondents and their family members have not contracted the virus. Additionally, over 70% of HCWs in a study at the Philippine General Hospital – many of whom have previously contracted the virus – stated willingness to work throughout the COVID-19 pandemic [26].
Affirming the findings of Poon, et al., our study found that the worsening of adverse working conditions contributed to the attrition of HCWs [17]. Many of our participants quit work due to the overwhelming workload brought on by the pandemic. They mostly worked from level 3 hospitals and in patient-intensive areas such as the emergency department, wards, and outpatient services. Further, majority also reported working beyond the prescribed 8-hour working shift by the Labor Code of the Philippines [27]. The increase in workload and long work hours likely intensified burnout and stress among those who quit. A qualitative study of nursing home staff in the United States reported similar findings, where, according to the respondents, the COVID-19 pandemic significantly increased staff workload, work hazards, and financial strains while decreasing job satisfaction and influencing staff turnover [28].
Despite working long hours and heavy workloads in high-risk environments, the participants reported a low net salary. During the pandemic, the government introduced additional compensation benefits such as COVID-19 hazard pay, special risk allowance, and comprehensive health insurance coverage for COVID-19-positive HCWs admitted to hospitals [29–32]. However, HCWs from the private sector were not uniformly covered and there were delays in providing these benefits [33,34]. Further, these benefits did not apply to family members who were also at risk of getting infected. Thus, being infected or having a family member infected and hospitalized could lead to impoverishing or catastrophic health expenditure.
To illustrate, in the Philippines, the estimated average out-of-pocket costs for being admitted for COVID-19 ranged from Php 4,005.60 to 44,428.63 [35]. The nurses who participated in the current study earned a median salary of Php 22,000 monthly. This meant that if a nurse or a family member were to get sick and admitted for COVID-19, the cost would potentially be equivalent to 2 months of work. That being said, the range provided for out-of-pocket hospitalization cost was likely an underestimation because this range was sourced from a public, tertiary-level hospital in the Philippines. This did not reflect hospitalization costs at private institutions and did not account for indirect costs such as lost wages.
The findings in this study contribute to literature explaining why there is an exacerbation of HCW shortage despite having a surplus of professionals in the Philippines [8,10]. The first reason is the persistence of brain drain, in which HCWs train locally but seek better opportunities in other countries [36]. Most of our participants were young professionals at the early stages of their healthcare careers. Among those who disclosed their intention to leave before the pandemic, nearly half desired to migrate and work abroad. The second reason is the transition of HCWs to other professions. Consistent with previously published findings by the Professional Regulatory Commission of the Philippines, only a portion of registered health professionals would eventually practice as HCWs [37]. In the current study, many participants transitioned to non-clinical roles, continued their education, or remained unemployed.
Recommendations to promote health workforce retention have remained consistent with pre-pandemic demands. This highlights longstanding issues in human resources for health. Even before the pandemic, a systematic review published in 2008 by Willis-Shattuck et al. [38] documented that significant motivators for HCW retention in low- and middle-income countries included financial rewards, career development, continuing education, hospital infrastructure, resource availability, hospital management, and recognition/appreciation – most of which were also proposed by our study participants. Additional suggestions such as the availability of personal protective equipment to ensure work safety have also been documented to increase willingness to work during health emergencies [39].
In light of our findings, it is important to take proactive steps to address the longstanding issues in the health workforce. The World Health Organization has provided a global strategy to address challenges in the health workforce. This includes creation and implementation of policies to address migration, bringing back workers into the health sector, and attracting unemployed health workers [2]. Rather than being reactive to HCW turnover, stakeholders must work together and invest in sustainable solutions to address existing problems such as work overload, burnout, and insufficient pay to encourage the retention of HCWs locally, not only in response to health emergencies, but more important, as a long-term public health investment.
Limitations
The online dissemination of the survey via convenience sampling on social media platforms and personal/professional networks limited the participant pool to those with social media accounts, internet access, and familiarity with using digital devices. Participant recruitment was conducted on a voluntary basis, introducing the potential for selection bias. To mitigate this, the survey was promoted through the social media accounts of professional organizations to achieve a broader reach. Geographic locations with limited internet access were not adequately represented and should be further explored in future research. The present study includes a disproportionately large number of participants from the NCR. As a result, our findings may have limited generalizability to other regions, which may have distinct experiences and challenges. Future research could seek a more proportionate representation across regions to capture the perspectives of HCWs beyond the NCR and enhance the generalizability of findings. Furthermore, the present study does not have a proportionate sample across HCW occupations from the private and public sectors. Considering that there may be differences between the two sectors (e.g., salary), obtaining a proportionate sample of HCWs from each occupation within private and public hospitals may offer a more generalizable and comprehensive understanding of the factors influencing each sector.
Ideally, a validated tool would have been used to investigate this issue. However, due to the acuity and time-dependent nature of data collection, we chose to adapt questionnaires from other studies covering the concepts of interest. Larger sample size and in-depth interviews to capture qualitative data would have contributed further to the current research. However, recruitment may be challenging as HCWs who resigned do not have organized groups. Future research may explore whether the HCWs who quit during the COVID-19 pandemic returned to work or retired from healthcare completely.
Conclusion
In this study among Filipino HCWs who resigned from their hospital-based employment during the early phase of the COVID-19 pandemic, we found that preexisting issues remained the most important reasons for quitting: work overload, burnout, stress, and insufficient pay. To strengthen the health workforce and encourage workforce retention, it is essential that ministries of health, hospital administrators, professional organizations, and health worker unions work together, to ensure continuity of health services even during national and global health crises.
Supporting information
S1 ChecklistChecklist for Reporting Results of Internet E-Surveys (CHERRIES).(DOCX)
S1 TextSurvey Questionnaire.(DOCX)
S1 ListList of Organizations.(DOCX)
S1 TableWorkplace information of survey respondents.(XLSX)
S2 TableSalary by Occupation.(XLSX)
S3 TableSalary by occupation, public vs. private.(XLSX)
S4 TableCauses of concern among healthcare workers.(XLSX)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1World Health Organization. Pulse survey on continuity of essential health services during the COVID-19 pandemic: interim report, 27 August 2020 [Internet]. 2020 Aug [cited 2024 Nov 9]. Available from: https://www.who.int/publications/i/item/WHO-2019-n Co V-EHS_continuity-survey-2020.1
- 2World Health Organization. Global strategy on human resources for health: Workforce 2030 [Internet]. Geneva, Switzerland; 2016 [cited 2024 Nov 9]. Available from: https://iris.who.int/bitstream/handle/10665/250368/9789241511131-eng.pdf
- 3World Health Organization. Facts on health and care workers [Internet]. 2021 [cited 2024 Nov 9]. Available from: https://www.who.int/campaigns/annual-theme/year-of-health-and-care-workers-2021/facts
- 4World Bank Group. Philippines [Internet]. 2023 [cited 2024 Nov 5]. Available from: https://data.worldbank.org/country/philippines
- 5Institute of Health Policy and Development Studies. Migration of health workers: Country case study Philippines [Internet]. Geneva, Switzerland; 2006 [cited 2024 Nov 8]. Available from: https://www.ilo.org/wcmsp 5/groups/public/---ed_dialogue/---sector/documents/publication/wcms_161163.pdf
- 6Brush BL, Sochalski J. International nurse migration: lessons from the Philippines. Policy Polit Nurs Pract. 2007;8(1):37–46. doi: 10.1177/1527154407301393 17470770 · doi ↗ · pubmed ↗
- 7Lorenzo FME, Galvez-Tan J, Icamina K, Javier L. Nurse migration from a source country perspective: Philippine country case study. Health Serv Res. 2007;42(3 Pt 2):1406–18. doi: 10.1111/j.1475-6773.2007.00716.x 17489922 PMC 1955369 · doi ↗ · pubmed ↗
- 8Mendoza DR. Shortage Amid Surplus: Emigration and Human Capital Development in the Philippines [Internet]. Bangkok and Washington; 2015 Dec [cited 2024 Nov 8]. (A Joint Series of the IOM Regional Office for Asia and the Pacific and the Migration Policy Institute). Report No.: 15. Available from: https://www.migrationpolicy.org/sites/default/files/publications/MPI%20Issue%20No%2015_2Dec 2015_web%20version_FINAL.pdf