Esophageal Cancer in a Mid-esophageal Diverticulum: A Case Report on Diagnostic Challenges and Treatment Outcomes
Garima Vats, Prajwal Chandrashekhara, Anuj, Kalale Radhakrishnan Bhagavan

TL;DR
A rare case of esophageal cancer developing in a mid-esophageal diverticulum highlights diagnostic challenges and treatment success.
Contribution
This case report highlights the diagnostic difficulties and treatment outcomes of esophageal cancer within a mid-esophageal diverticulum.
Findings
Initial biopsies were non-diagnostic, but a CT scan and bronchoscopy confirmed squamous cell carcinoma.
The patient responded positively to chemotherapy and radiotherapy.
Early detection and thorough evaluation are critical for improved outcomes in such rare cases.
Abstract
Esophageal diverticula are rare pouches that form in the esophageal lining. They occur infrequently in the general population and are more often seen in individuals with dysphagia. Among the types, mid-esophageal (parabronchial) diverticula are especially uncommon. These diverticula are usually asymptomatic and are often found incidentally during diagnostic procedures. Unlike distal esophageal diverticula, which may be linked to acid reflux, mid-esophageal types are thought to result from long-standing inflammation or mechanical forces acting on the esophagus. Although cancer arising in esophageal diverticula is uncommon, when it does occur, it may progress more rapidly due to structural weaknesses in the diverticular wall. We present the case of a middle-aged man with progressive difficulty swallowing and a persistent dry cough. Endoscopy identified a large mid-esophageal diverticulum…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
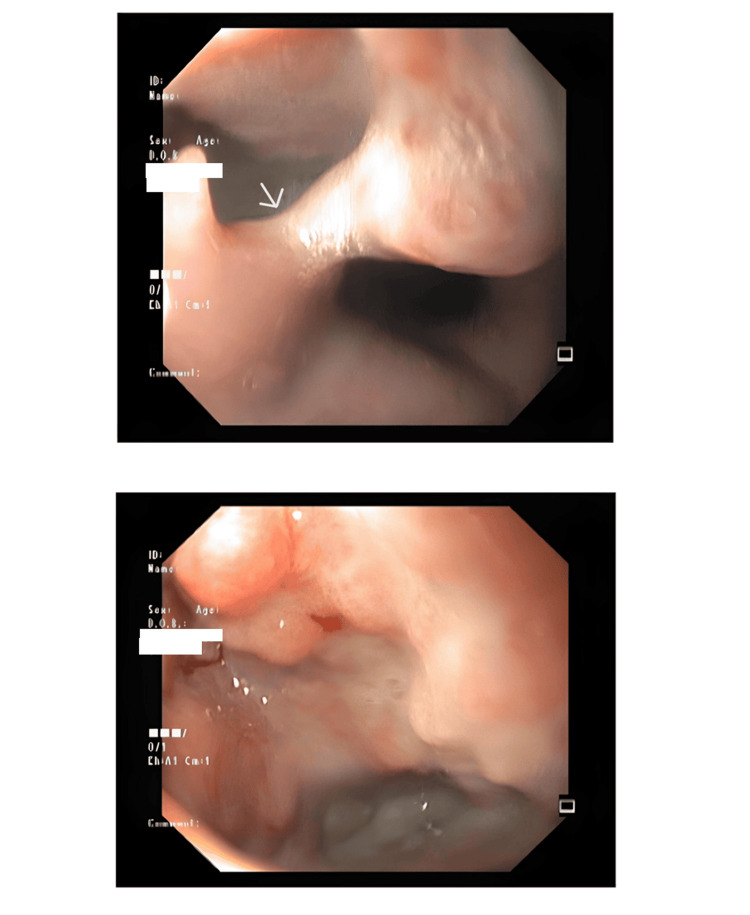 Figure 1
Figure 1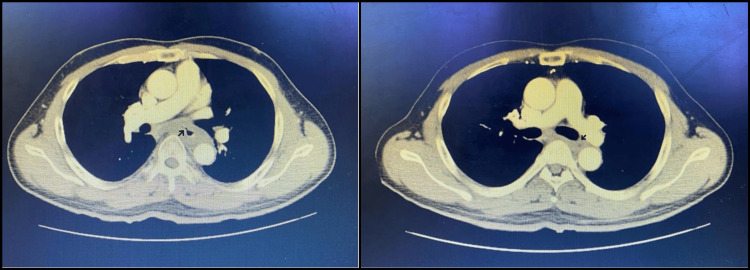 Figure 2
Figure 2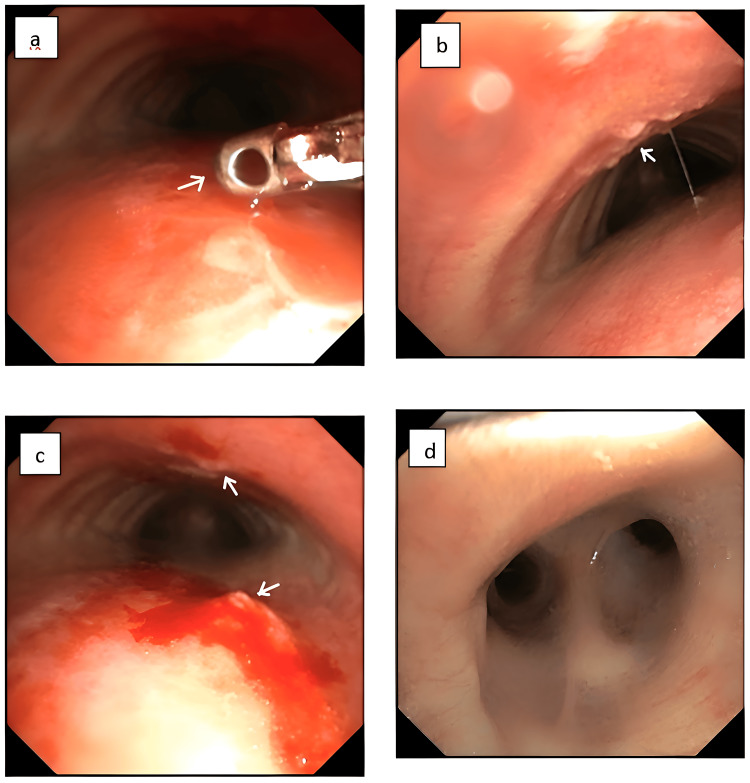 Figure 3
Figure 3| Treatment Phase | Details |
| Neoadjuvant Chemotherapy | Three cycles administered at 3-week intervals |
| Chemotherapy Regimen | Paclitaxel: 260 mg in 1 pint normal saline with ondansetron, infused over 3 hours - Carboplatin: 450 mg in 5% dextrose IV over 3 hours |
| Response to Initial Treatment | Significant tumor reduction and resolution of irregular mucosa in the diverticulum after neoadjuvant therapy followed by radical radiotherapy |
| Subsequent Chemoradiotherapy | Three additional cycles of chemotherapy using the same dosing schedule |
| Radiotherapy Details | 30 fractions of external beam radiotherapy, delivering a total of 54 Gy over six weeks |
| Article (Year) | Size of Diverticulum | Extent of Carcinoma at Diagnosis | Metastatic Lesions Present | Treatment Given | Outcome | Reference Number |
|---|---|---|---|---|---|---|
| Fukuda et al., 2023 | 10 cm | cT1a-EP/LPM N0 M0 (in situ, 20mm lesion), pTis-EP, ly0, v0, R0 | none | Surgical resection (diverticulectomy) | Discharged, no complications | [ |
| Zhang et al., 2023 | Shallow pulsion diverticulum | 28 mm superficial esophageal cancer in the middle thoracic esophagus | none | Endoscopic submucosal dissection (ESD) followed by a temporary covered esophageal stent | Discharged, no complications | [ |
| Polit et al., 2022 | 5.0 × 4.4 × 2.4 cm diverticulum | 3.2 × 2.5 × 1 cm, exophytic, ulcerated, involving the full esophageal wall, abutting serosa. Moderately differentiated squamous cell carcinoma on microscopy, margins negative | none | Open surgical diverticulectomy (Zenker resection) followed by hematology-oncology reference | Not stated (but authors note that after simple diverticulectomy with clear margins, patients are expected to remain disease-free) | [ |
| Fu et al., 2017 | Large epiphrenic diverticulum just above the esophagogastric junction | Intraepithelial squamous cell carcinoma confined to lamina propria, no lympho-vascular invasion, margins negative. | none | Endoscopic submucosal dissection (ESD) | Uneventful hospital course. No local recurrence or metastasis at 42-month follow-up. | [ |
| Tanaka et al., 2015 | Shallow pulsion diverticulum, ~3 × 2 cm | Macroscopic type 0-Ⅱc, half circumference of the middle thoracic esophagus. Squamous cell carcinoma lesion confined to epithelium or lamina propria mucosa (NBI/IPCL). | none | Endoscopic submucosal dissection (ESD). Perforation occurred- repaired with clips + detachable snare | Mediastinal and subcutaneous emphysema, fever, and leukocytosis all resolved by day 7. Discharged in good condition. | [ |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEsophageal and GI Pathology · Esophageal Cancer Research and Treatment · Gastrointestinal Tumor Research and Treatment
Introduction
An esophageal diverticulum is a rare condition characterized by an outpouching of the esophageal mucosa. It affects less than 1% of the general population and occurs in approximately 1% to 3% of individuals presenting with dysphagia [1-2]. A mid-esophageal diverticulum, also known as a parabronchial diverticulum, is typically located about 5-6 cm distal to the tracheal bifurcation [3]. The risk of malignancy in esophageal diverticula varies by location, with reported rates of 0.3-7.1% in pharyngeal, 1.8% in mid-esophageal, and 0.6% in epiphrenic diverticula [4]. A Japanese study identified the most common sites of esophageal diverticula as the pharyngeal esophageal region (Zenker’s diverticulum, 15.8%), the tracheal bifurcation (Rokitansky diverticulum, 73.0%), and the supradiaphragmatic region (11.2%) [5]. Mid-esophageal diverticula are relatively uncommon, often asymptomatic, and typically discovered incidentally. Unlike distal diverticula, which are frequently associated with gastroesophageal reflux disease, mid-esophageal diverticula are more commonly related to chronic mediastinal inflammation and traction forces exerted on the esophageal wall [1].
Pulsion diverticula are considered false diverticula because they lack a muscular layer and result from elevated intraluminal pressures, typically due to underlying esophageal motility disorders [6]. Due to the absence of the muscularis propria, malignancy in pulsion diverticula may infiltrate the adventitia and adjacent tissues more readily [7].
Case presentation
A male patient in his early fifties presented with a six-month history of progressively worsening dysphagia to solids, which had intensified over the past month but improved with liquids. He also reported a persistent change in voice over the same six-month period and a dry cough for the past 25 days. Additionally, the patient recalled experiencing mild dysphagia and postprandial cough intermittently over the past three years, though these symptoms were previously less severe. There was no history of dyspnea, hemoptysis, or other gastrointestinal symptoms such as vomiting, abdominal pain, distension, diarrhea, or constipation. His medical history was significant for type II diabetes mellitus for the past 10 years, with no history of tobacco or alcohol use. There was no personal or family history of malignancy. General and systemic examinations were unremarkable.
Given the progressive dysphagia, an upper gastrointestinal endoscopy (UGI scopy) was performed. This revealed a mid-esophageal diverticulum approximately 6-8 cm in length, located 25 cm from the incisors. The mucosal surface appeared irregular, prompting multiple biopsies. Histopathology revealed normal mucosa with granulation tissue (Figure 1).
EsophagogastroduodenoscopyEsophagogastroduodenoscopy images depicted ulceroproliferative growth noted in the mid esophageal diverticula (marked by an arrow).
In spite of the normal biopsy report, further evaluation was done based on clinical suspicion; a contrast-enhanced CT (CECT) scan of the thorax was performed. The scan revealed circumferential wall thickening in the infracarinal thoracic esophagus (10 mm thick and 7.6 cm long), causing luminal narrowing. Periesophageal fat stranding, loss of mural stratification, and indistinct fat planes with adjacent vital structures were noted. The esophageal thickening extended into the prevertebral space and encroached on surrounding vascular and bronchial structures. Additionally, metastatic deposits were identified in both lungs, strongly suggesting advanced malignancy (Figure 2).
Contrast-enhanced CT (CECT) of the thorax CECT Thorax images depicting circumferential enhancing wall thickening of infracarinal thoracic oesophagus measuring a maximum thickness of 10 mm for a length of 7.6 cm, causing luminal narrowing. Indistinct fat planes with the left main bronchus, left atrium, arch of aorta, left main pulmonary artery, and descending thoracic aorta (marked by arrows).
Despite repeated biopsies showing only granulation tissue, the patient’s persistent symptoms, the endoscopic appearance of the lesion, and CT findings heightened clinical suspicion for malignancy. A bronchoscopy was performed to assess for airway involvement. This revealed infiltrative growths on the anterior and posterior walls of the trachea, along with a mucosal bulge at the distal end of the left main bronchus. Brush cytology taken during bronchoscopy and evaluated with rapid on-site evaluation (ROSE) was suggestive of squamous cell carcinoma originating from the esophagus with tracheal infiltration (Figure 3).
BronchoscopyBronchoscopy images: a. and c. Infiltrative growth seen in both anterior and posterior walls of the trachea (marked by arrows); b. mucosal bulge seen at the distal end of the left main bronchus (marked by an arrow); d. the main carina appears normal.
Subsequent histopathology confirmed moderately differentiated squamous cell carcinoma. Based on imaging and histopathological findings, a final diagnosis of metastatic infracarinal esophageal squamous cell carcinoma (T4aN3M1) was made.
The patient was initiated on treatment with three cycles of neoadjuvant chemotherapy (paclitaxel and carboplatin) followed by radical radiotherapy. A repeat CECT thorax revealed significant tumor reduction and resolution of the mucosal irregularity within the diverticulum. The patient subsequently completed three more cycles of chemotherapy and received 30 fractions of external beam radiation (54 Gy) over six weeks, with a favorable clinical response.
Differential diagnostic reasoning
The patient presented with dysphagia, hoarseness of voice, and cough, raising clinical suspicion for esophageal malignancy and prompting an upper gastrointestinal (UGI) endoscopy. Endoscopic evaluation revealed a mid-esophageal diverticulum with irregular mucosa, raising concern for carcinoma arising within the diverticulum. To further assess the extent of disease, a CECT of the thorax was performed, which demonstrated esophageal wall thickening, loss of fat planes with adjacent mediastinal structures, and pulmonary metastases--findings suggestive of advanced malignancy. Endoscopic biopsies, however, were inconclusive, showing only granulation tissue. Despite this, the patient's age, symptoms, and radiologic findings maintained a high index of suspicion for malignancy. Subsequent bronchoscopy revealed tracheal infiltration, and cytological and histopathological analysis confirmed squamous cell carcinoma. This case highlights the diagnostic challenges of malignancy arising within an esophageal diverticulum, particularly when initial biopsies are non-diagnostic, and underscores the importance of a high degree of clinical suspicion and a multimodal approach to diagnosis and management.
Treatment
Treatment Rationale and Dose Calculations
The patient was planned for combined modality treatment with radiotherapy and chemotherapy (Table 1).
Radiotherapy: Three-dimensional conformal radiotherapy (3D-CRT) was delivered to a total dose of 54 Gy in 30 fractions over 6 weeks (1.8 Gy per fraction, 5 fractions per week).
Chemotherapy: Concurrent systemic therapy with paclitaxel and carboplatin was administered. Based on a body surface area (BSA) of 1.6 m², the recommended dose of paclitaxel (175 mg/m²) corresponded to 280 mg, and an adjusted dose of 260 mg was given [8]. The carboplatin dose was calculated using the Calvert formula, with a glomerular filtration rate (GFR) of 67.2 mL/min. For a target area under the curve (AUC) of 5, as recommended in standard regimens [8], the calculated dose was approximately 461 mg, and the patient received 450 mg.
Outcome and follow-up
The patient received three cycles of neoadjuvant chemotherapy with paclitaxel and carboplatin, followed by reassessment showing a reduction in esophageal wall thickening and lung nodules. He subsequently underwent radical radiotherapy with significant tumor regression, then 3 additional chemotherapy cycles and 54 Gy radiation over 6 weeks.
Four months post-treatment, positron emission tomography (PET)-CT showed no residual esophageal lesion but revealed metastatic cervical lymphadenopathy and lung nodules. He was started on oral gefitinib 250 mg on alternate days, which he has continued for the past year. A repeat PET-CT four months ago showed mild regression of cervical nodes but no change in lung nodules. Hence, according to RECIST criteria (RECIST Working Group), despite complete resolution of the primary lesion, the lack of response in metastatic lung lesions classifies the case as stable disease (SD). Nonetheless, this still indicates a relatively favorable prognosis compared to typical outcomes in esophageal carcinoma [9].
Discussion
Esophageal diverticula, though rare, have become a focus of surgical interest over the past two decades. The risk of malignancy is higher in pulsion diverticula compared with true diverticula because of their anatomical differences [4]. Chronic irritation and inflammation, often caused by food stasis within the diverticulum, are key factors contributing to malignant transformation [10]. Esophageal diverticular carcinoma frequently presents at an advanced stage since its symptoms, such as dysphagia, regurgitation, or halitosis, are often attributed to the diverticulum itself rather than to malignancy [11]. This makes both the need for early diagnosis and the difficulty of achieving it particularly critical. Barium esophagography remains a useful tool for initial evaluation, but UGI scopy has gained prominence over time, as it allows for biopsy and definitive exclusion of malignancy [12]. However, esophagoscopy carries a risk of perforation, and manometry should be performed first to rule out motility disorders [13]. In selected cases, bronchoscopy can provide important additional information, particularly for detecting tracheal infiltration and confirming malignancy. Although long-term survival has been reported in some cases, such as Dionigi et al. [14], the overall prognosis remains poor for patients with esophageal diverticula complicated by malignancy. This highlights the importance of strict surveillance and follow-up, with any mucosal changes--ulceration, thickening, or discoloration--biopsied without delay. If cancer is confirmed, management should follow standard esophageal cancer protocols, including surgery, endoscopic therapy, or chemoradiation, depending on stage [15].
Table 2 summarizes recently reported cases of esophageal diverticula with squamous cell carcinoma, including mid-esophageal pulsion diverticula, together with their clinical details and management. Notably, across these reports, all patients were non-metastatic at presentation and underwent local resection, either endoscopic submucosal dissection (ESD) for superficial lesions or diverticulectomy for Zenker’s and larger diverticula. Outcomes were favorable in the short term, with disease-free follow-up where available. These findings suggest that when staging confirms mucosal disease without nodal or distant spread, simple resection (ESD or surgical diverticulectomy) is both appropriate and effective.
Conclusions
Although prognosis is generally poor for advanced esophageal diverticular carcinoma due to delayed diagnosis and the thin diverticular wall that allows rapid invasion, recent non-metastatic cases show that early detection and localized resection can lead to favorable outcomes. Symptoms may be mistaken for the diverticulum itself, leading to late detection. Regular endoscopic surveillance with prompt biopsy of suspicious changes is essential. When cancer is identified, treatment should follow standard esophageal cancer protocols. Vigilant monitoring and early intervention can markedly improve outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Esophageal diverticula Stat Pearls [Internet] 5 2025 Yam J Baldwin D Ahmad SA Treasure Island (FL)Stat Pearls Publishing 2023 https://www.ncbi.nlm.nih.gov/books/NBK 532858/30422453 · pubmed ↗
- 2Frequency and etiology of midesophageal diverticula at barium esophagography Clin Imaging Hoghooghi D Coakley FV Breiman RS Qayyum A Yeh BM 2452473020061681413910.1016/j.clinimag.2006.02.002 · doi ↗ · pubmed ↗
- 3Giant mid-esophageal pulsion diverticulum: a report of two operated cases Ann Thorac Surg Svane S 169216947120011138383110.1016/s 0003-4975(00)02297-9 · doi ↗ · pubmed ↗
- 4Esophageal diverticula and cancer Dis Esophagus Herbella FA Dubecz A Patti MG 1531582520122233520110.1111/j.1442-2050.2011.01226.x · doi ↗ · pubmed ↗
- 5A case of esophageal cancer in the esophageal diverticulum - a review of cases reported in Japan Jpn J Gastroenterol Surg Adachi J Tsutsui K Takano T 483487372004
- 6Pulsion diverticulum of the oesophagus: more than just an out pouch Indian J Surg Sonbare DJ 44487720152582971110.1007/s 12262-013-0955-8PMC 4376845 · doi ↗ · pubmed ↗
- 7Two cases of superficial esophageal cancer arising in esophageal diverticula Gastroenterol Endosc Chino O Makuuchi H Machimura T 303309381996 https://www.jstage.jst.go.jp/article/gee 1973 b/38/2/38_2_303/_article/-char/en
- 8A phase II study of carboplatin and paclitaxel in esophageal cancer Ann Oncol El-Rayes BF Shields A Zalupski M 9609651520041515195510.1093/annonc/mdh 230 · doi ↗ · pubmed ↗