Incidental rib hotspots on 99mTc-pyrophosphate scintigraphy in a patient with transthyretin cardiac amyloidosis: cough-induced fractures unveiled
Satoshi Kurisu, Hitoshi Fujiwara

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
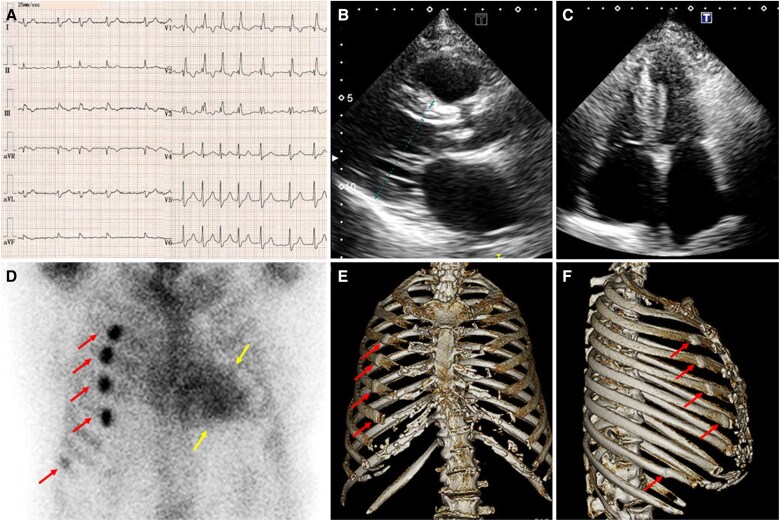 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMedical Imaging and Pathology Studies · Amyloidosis: Diagnosis, Treatment, Outcomes · Bone health and treatments
Case description
An 88-year-old woman was hospitalized for an asthma exacerbation. She had lumbar canal stenosis and bilateral carpal tunnel syndrome but no family history of heart disease. After a severe coughing episode, she was treated with intravenous corticosteroids. Two months later, she was readmitted for heart failure. Electrocardiography showed atrial fibrillation, low-voltage complexes, and right bundle branch block (Figure 1A). Transthoracic echocardiography revealed increased left ventricular wall thickness of 12 mm (Figure 1B), preserved ejection fraction of 58%, and increased left atrial volume index of 48 mL/m^2^ (Figure 1C), raising suspicion for cardiac amyloidosis. Technetium-99m pyrophosphate (99mTc-PYP) scintigraphy demonstrated Perugini Grade 3 myocardial uptake (Figure 1D, yellow arrows). Serum and urine immunofixation were negative for monoclonal proteins, and transthyretin genotyping was not performed. The diagnosis of transthyretin cardiac amyloidosis was made,^1^ and treatment with azosemide, dapagliflozin, and apixaban was initiated.
Electrocardiography showed atrial fibrillation, low-voltage complexes, and right bundle branch block (A). Transthoracic echocardiography revealed increased left ventricular wall thickness of 12 mm (B) and increased left atrial volume index of 48 mL/m2 (C). Technetium-99 m pyrophosphate scintigraphy demonstrated Perugini Grade 3 myocardial uptake (D, yellow arrows). Unexpectedly, five focal extracardiac hotspots were observed: four along the anterolateral right third to sixth ribs and one at the lateral right ninth rib (D, red arrows). Chest computed tomography demonstrated focal sclerotic changes at the third to sixth rib sites on frontal and lateral images (E and F, arrows), consistent with healed rib fractures. At the ninth rib site, a fracture line was clearly visualized on lateral imaging (F, arrow), confirming an additional rib fracture.
Unexpectedly, five focal extracardiac hotspots were observed: four along the anterolateral right third to sixth ribs and one at the lateral right ninth rib (Figure 1D, red arrows). Because of these hotspots, the heart-to-contralateral ratio could not be reliably measured. Chest computed tomography demonstrated focal sclerotic changes at the third to sixth rib sites on frontal and lateral images (Figure 1E and F, arrows), consistent with healed rib fractures. At the ninth rib site, a fracture line was clearly visualized on lateral imaging (Figure 1F, arrow), confirming an additional rib fracture. Although the exact timing of injury could not be confirmed, the fractures were suspected to be related to the recent coughing episode.
Cough-induced rib fractures are most commonly observed in postmenopausal women and are associated with risk factors such as asthma, osteoporosis, and corticosteroid use.^2,3^ This case underscores the importance of assessing extracardiac findings on 99mTc-PYP scintigraphy, as they may provide clinically meaningful insights beyond myocardial assessment.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Gillmore JD, Maurer MS, Falk RH, Merlini G, Damy T, Dispenzieri A, et al Nonbiopsy diagnosis of cardiac transthyretin amyloidosis. Circulation 2016;133:2404–2412.27143678 10.1161/CIRCULATIONAHA.116.021612 · doi ↗ · pubmed ↗
- 2Hanak V, Hartman TE, Ryu JH. Cough-induced rib fractures. Mayo Clin Proc 2005;80:879–882.16007893 10.4065/80.7.879 · doi ↗ · pubmed ↗
- 3Katrancioglu O, Akkas Y, Arslan S, Sahin E. Spontaneous rib fractures. Asian Cardiovasc Thorac Ann 2015;23:701–703.25957093 10.1177/0218492315586485 · doi ↗ · pubmed ↗