Physical Therapists’ Use of Behavior Change Strategies to Promote Physical Activity for Individuals with Neurological Conditions
Amber LaMarca, Gwendolyn Larsen, Kathleen D. Lyons, Julie Keysor

TL;DR
Physical therapists working with neurological patients focus on home exercises but rarely use strategies to promote aerobic activity or behavior change.
Contribution
This study characterizes how physical therapists use behavior change techniques to promote physical activity in neurorehabilitation.
Findings
Home exercise programs are emphasized over aerobic activity in PA promotion.
Common BCTs include instruction, behavioral practice, and social support.
Factors like knowledge, beliefs, and environment influence BCT use.
Abstract
Background/Objectives: People living with neurological conditions are inactive despite widespread literature showing physical activity (PA) is beneficial for this population. To impact long term changes in PA behavior, physical therapists treating individuals with neurological conditions need to provide effective PA promotion in combination with behavior change techniques (BCTs). The purpose of this study is to (1) characterize the use of BCTs during neurorehabilitation, and (2) to gain an understanding of considerations related to PA promotion. Methods: Observations of outpatient physical therapy encounters with subsequent semi-structured interviews were conducted. Observations were transcribed with detailed field notes and analyzed with descriptive analysis and deductive coding. Interviews were analyzed with thematic analysis. Results: Observations indicated that PA promotion in…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
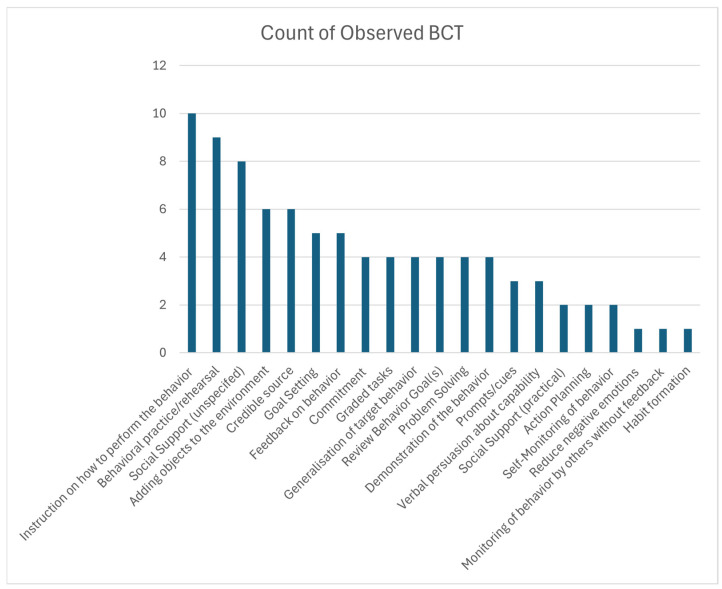 Figure 1
Figure 1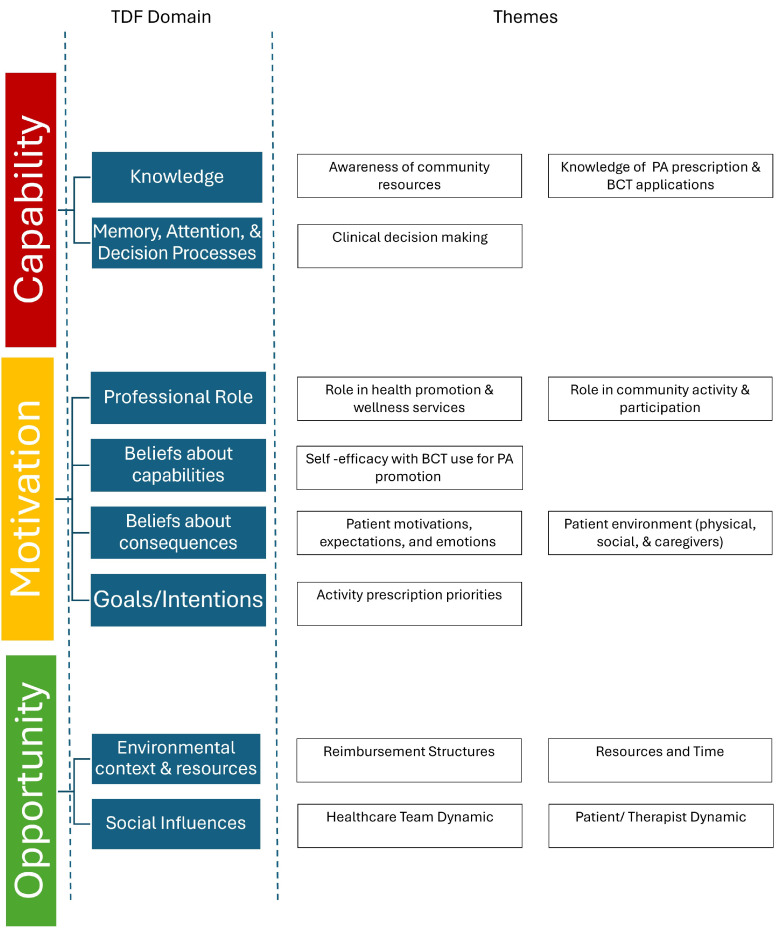 Figure 2
Figure 2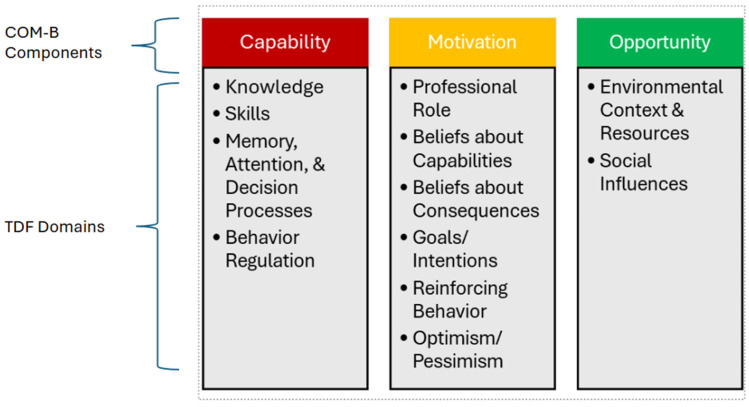 Figure 3
Figure 3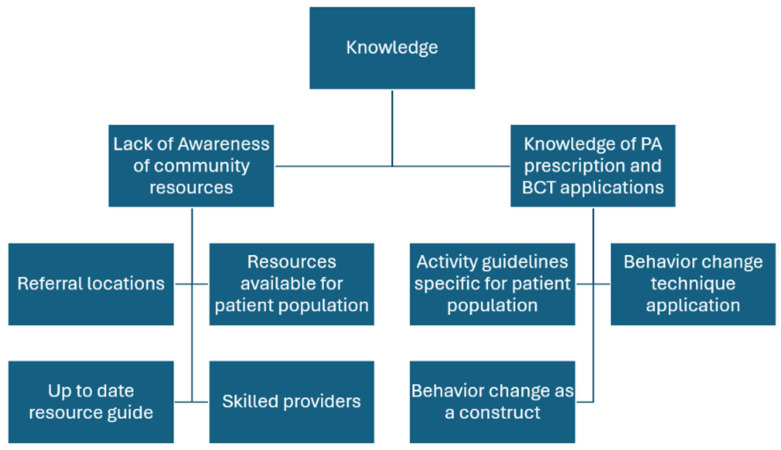 Figure 4
Figure 4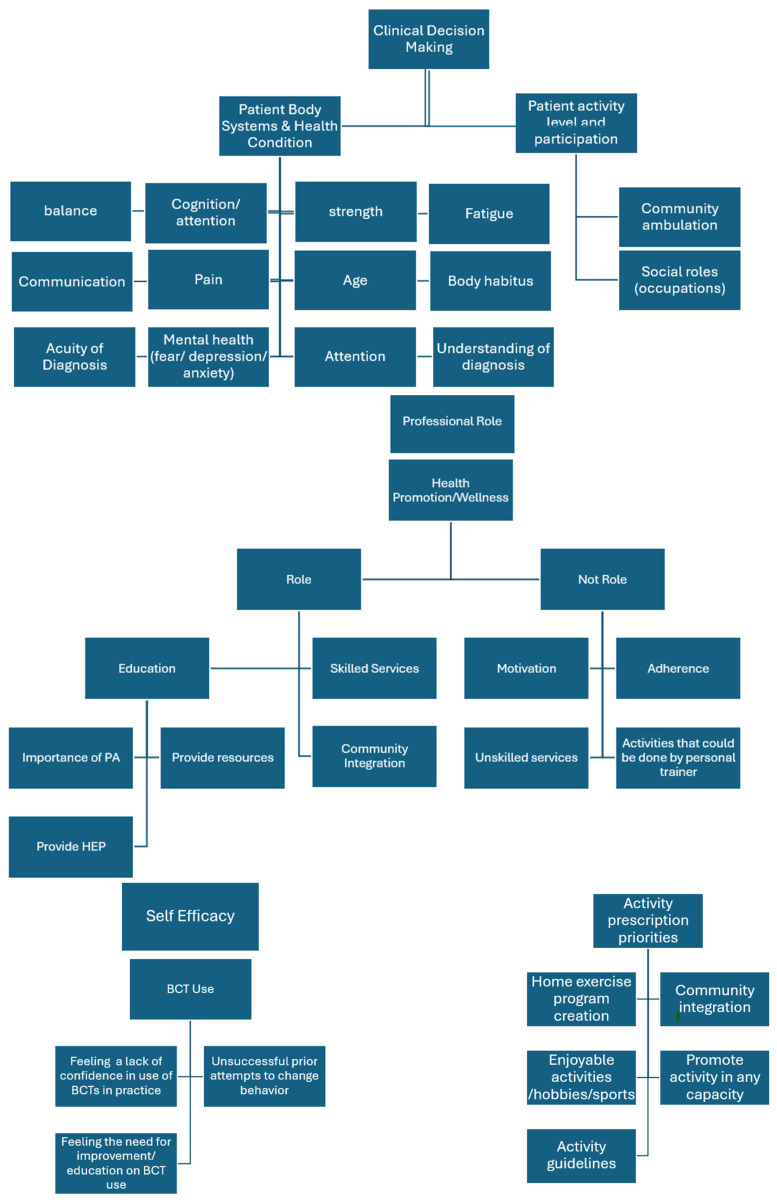 Figure 5
Figure 5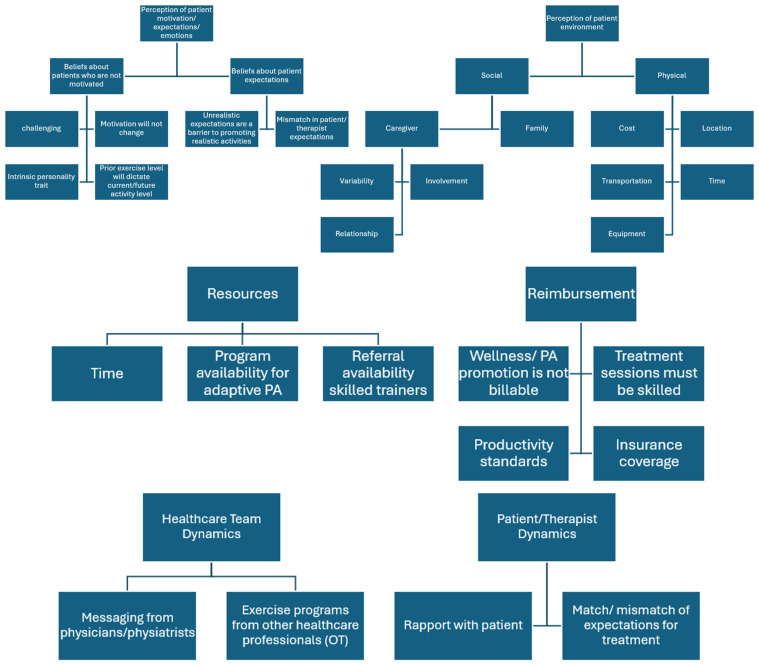 Figure 6
Figure 6Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPhysical Activity and Health · Behavioral Health and Interventions · Telemedicine and Telehealth Implementation
1. Introduction
Chronic neurological conditions, including stroke, Parkinson’s disease, traumatic brain injury, multiple sclerosis, and spinal cord injury are leading causes of disability globally and result in many lifelong multisystem impairments including mobility, cognition, and more [1]. Physical activity (PA) is recommended for individuals with neurological impairments for long-term management of health outcomes with an emphasis on moderate-intensity aerobic activity combined with strengthening, balance, and stretching [2,3,4,5]. PA can improve overall health factors (e.g., reducing blood pressure and arterial stiffness), improve neuroplasticity and functional outcomes (e.g., walking and balance), and reduce secondary complications and comorbidities [6,7,8,9]. However despite the well-known benefits of PA, people with neurological conditions are largely inactive [10,11,12,13]. To increase PA, it is recommended that healthcare professionals utilize behaviorally informed PA promotion, which is the use of behavior science to help guide the adoption of PA behaviors [14,15,16,17]. A critical component of behaviorally informed PA promotion is the use of individualized behavior change techniques (BCTs) such as goal setting, problem solving, and feedback [18]. Use of BCTs is linked to improvements in PA promotion in adults with musculoskeletal and chronic disease conditions [19,20,21,22,23,24,25].
However, despite recommendations and the widespread understanding of the importance of use of behavioral strategies to promote PA, it is rarely performed in practice by physicians and general practitioners [26,27]. Physical therapists with neurological clinical expertise may be well-poised to fill this gap as they are skilled in implementing effective treatments to address the functional needs of this population [28,29,30], and may be well-suited to promote PA when patients are being discharged from outpatient neurological physical therapy [27,31,32]. Behaviorally informed PA promotion approaches coupled with treatment of the complex physical elements of neurological conditions such as impaired motor control, muscle weakness, instability, gait impairments, and low endurance could be beneficial for patients as they transition to the home and community to promote long-term PA behavior [33,34,35,36]. Yet, little is known regarding how BCTs can be used to promote PA in adults with chronic neurological conditions. To our knowledge, there are no studies that explore how physical therapists in outpatient neurological clinics use behaviorally informed approaches to promote PA to help transition patients from outpatient clinical care to home-based PA programs.
The purpose of this study was to (1) characterize PA promotion and the use of behavior change strategies during physical therapists’ outpatient clinical encounters with people with chronic neurological conditions, and (2) gain an understanding of physical therapists’ perspectives regarding promoting home-based PA as patients are discharged from skilled outpatient therapy.
2. Materials and Methods
This qualitative study is reported following the Standards for Reporting Qualitative Research (SRQR) [37]. This study was approved by the local IRB (#2024P003290) and all participants provided consent.
2.1. Qualitative Approach and Research Paradigm
The study was a qualitative descriptive study designed with an interpretivism epistemological stance to gain an understanding of physical therapists’ actions, beliefs, motivations, and reasoning regarding promoting PA when transitioning patients from skilled care to independent home programs [38,39,40]. The overarching framework used to guide this work was the Capability, Opportunities, and Motivation System of Behavior (COM-B) [41]. The COM-B describes that there are three main components that influence behavior, capability, opportunity, and motivation, that can be further broken down into fourteen subdomains using the Theoretical Domains Framework (TDF) [42]. For a visual representation, please see Appendix A [43]. The domains of the TDF include ‘Knowledge’, ‘Skills’, ‘Social/Professional Role and Identity’, ‘Beliefs about Capabilities’, ‘Optimism’, ‘Beliefs about Consequences’, ‘Reinforcement’, ‘Intentions’, ‘Goals’, ‘Memory, Attention and Decision Processes’, ‘Environmental Context and Resources’, ‘Social Influences’, ‘Emotions’, and ‘Behavioral Regulation’. The COM-B and TDF integrated frameworks have been used to investigate healthcare professionals’ use of PA promotion in practice [44,45,46,47] and were used to guide study design, interview structure, and data analysis for this study.
2.2. Research Team Characteristics and Reflexivity
The research team comprised physical and occupational therapists and included individuals with backgrounds in clinical care and qualitative research. Three out of the four (AL, GL, and JK) had outpatient neurorehabilitation experience representing over 40 years of neurorehabilitation practice. AL and GL currently treat individuals with neurological conditions in the outpatient setting while engaging in academic research. Two members (JK and KDL) are experienced clinical researchers with expertise in qualitative research. Two members (AL and JK) completed the Behavior Change Taxonomy training and certification [48,49]. One team member (AL) conducted observations and semi-structured interviews. Two members analyzed the observational data (AL and JK); two members analyzed the semi-structured interview data (AL and GL). The team member that performed the observations and interviews (AL) had previous experience working in the hospital network and knew the physical therapist participants in the study. As a result, interview responses may be impacted by the familiarity from previous working relationships and a tendency to speak towards shared experiences. Her knowledge and past experiences assisted with her understanding of the work environment, patient population, and discharge process. To complement extensive clinical experience while minimizing potential bias related to known relationships with the study participants, a pre-determined interview guide and process informed by the COM-B [50], TDF [42], and scientific evidence was employed. Additionally, reflexivity was applied by the research team by discussing and challenging assumptions throughout the data analysis process.
2.3. Context
As little is known about this topic, we selected a setting known for its high standard of care in neurorehabilitation as this was most likely to reflect best practice. We targeted licensed physical therapists working in a neurological outpatient practice in an internationally recognized academic rehabilitation hospital, Spaulding Rehabilitation Hospital in Charlestown, MA, who were preparing patients for discharge from skilled physical therapy. Spaulding Hospital is recognized as a leader in neurological rehabilitation in the United States and is actively involved in academic research and teaching.
Prior to the observations and semi-structured interviews, therapists were informed that the purpose of the study was to understand the strategies physical therapists utilize to transition patients from clinic to home- and community-level PA during the discharge process. Observations were completed in the natural treatment environment of the outpatient physical therapy clinic to allow for the observation of the environmental context including resources and social interactions.
2.4. Sampling Strategy
Convenience sampling was utilized to recruit participants (i.e., physical therapists) who worked in the neurological outpatient department. Novice and experienced clinicians were sought for inclusion. Five physical therapists were enrolled, each with two patient encounters. Inclusion criteria included adults (18 years or older), individuals who were English-speaking, licensed physical therapists that performed at least 20 h of patient care per week, maintained a caseload comprising at least 50% patients with neurological conditions, and had at least two patients on caseload with anticipated discharge in the next month. Patients that were included in observations had to have adequate cognitive function and speak English to provide verbal consent for the observation of their clinical encounter.
2.5. Data Collection Methods
Data collection was performed from December 2024 through February 2025. Ten observations were completed, two observations for each participant (therapist). Each therapist completed a semi-structured interview at the completion of the second observation. Therapists’ demographics (age, gender, specialty certification, years of practice) were obtained by self-report and patient demographics were obtained (age, gender, primary diagnosis, ambulation status, caregiver presence during clinical encounter) from the medical chart.
2.5.1. Observations of Physical Therapist–Patient Clinical Encounters
Data were collected pertaining to physical therapist–patient communications and behaviors (AL). Discharge or discharge-planning encounters were chosen to capture conversations regarding therapist recommendations for home and community PA after discharge. Each clinical encounter was scheduled for 45 min. Efforts were made to avoid interruption of the traditional flow of clinical encounters or planned activities during observations.
Detailed field notes were taken to document the conversations, facial expressions, body language, actions, environmental characteristics, targeted PA behaviors, assessments of PA, and the context surrounding PA promotion. In addition to in-the-moment field notes, the researcher completed expanded detailed notes immediately after the observations. The researcher also completed a same-day debriefing session with physical therapists to allow the therapist to briefly share additional context of the patient’s situation, the clinical encounter that was observed, and their thoughts on the clinical encounter. The debrief was typically about 5 min in length or as time allowed based on the therapist’s schedule. Audio/video recordings were not plausible due to the open settings of the gym. Following observations, a reflective memo was completed that summarized the researcher’s evolving reflections and interpretations of the data.
2.5.2. Semi-Structured Interviews
Semi-structured interviews were conducted, recorded, and transcribed via a secure Zoom platform. All interviews were conducted using a pre-defined interview guide by one investigator (AL). The order of questions asked was variable based on conversation flow. Additional prodding questions were employed to expand on each participant’s experience. Whenever possible, open-ended questions were asked to study participants to elicit data in a non-biased manner.
The priorities of the interview were to (1) triangulate data from observations by asking therapists about what PA promotion strategies they use in practice and (2) understand capabilities, opportunities, and motivations that impact BCT use for PA promotion. First, therapists were asked about strategies they used for PA promotion. Second, they were asked questions based on the TDF model to address the subdomains of capabilities, opportunities, and motivations behind BCT use for PA promotion. See Appendix B for interview guide.
2.6. Data Processing and Analysis
2.6.1. Observations of Physical Therapist–Patient Clinical Encounters
After observations were completed, field notes were further revised, expanded, and cleaned for interpretation and descriptive statistics were computed. BCTs were coded according to the Behavior Change Technique Taxonomy [48,49].
First, the target PA behaviors were identified for each field note (AL). Target PA behaviors had to meet two criteria to be included: (1) it was classified as PA, defined using the older adult and adult wheelchair user physical activity compendiums [51,52], and (2) it was intended for carryover to the home or community setting. PA behaviors were then classified by the type of PA (e.g., walking activity, resistance exercise, recreational activity, household activity, aerobic exercise). While many physical activities could be considered aerobic, we used the code “aerobic exercise” only when the PA prescription was given with explicit instructions to focus on elevating one’s heart rate or reaching a higher level of perceived exertion.
Second, deductive coding of field notes [53] was performed using the predetermined Michie’s Behavior Change Technique Taxonomy [48] to code specific BCTs during the observed clinical encounters. Two independent researchers (A.L. and J.K.) extracted field note text that included promotion of target PA behaviors and then applied a corresponding taxonomy code.
Third, the coders extracted how BCTs were carried out (verbal instructions, use of materials and handouts, etc.), if PA parameters were prescribed (i.e., frequency, duration), and whether the strategy was initiated by the therapist, patient, or caregiver. To evaluate agreement, the average interrater agreement was calculated for BCT coding between observations and across item level for each BCT code.
2.6.2. Semi-Structured Interviews with the Physical Therapists
Interview recordings were transcribed via Zoom then cleaned, de-identified, and verified for accuracy alongside audio recordings. Filler words were also removed from transcripts (“like”, “um”, “kind of”, etc.) to enhance clarity for analysis. Two coders (AL and GL) reviewed the transcripts to identify relevant content for further analysis.
The portion of the interview used for triangulation of observations was deductively coded by two coders (AL and GL) for strategies that therapists reported they used for PA promotion. This was compared with BCTs that were observed during clinical encounters.
Additionally, the coders (AL and GL) explored therapist perspectives on BCT use for PA promotion. The coders inductively coded interviews and created operational definitions that were kept in a code book. After every transcript was analyzed, the coders met to discuss and iteratively create and modify the codes. If coders disagreed on a code, it was discussed until a consensus was formed. The coders then looked for patterns and created themes [54,55]. To guide interpretation and to ground the results in theory, the themes were located within TDF domains using TDF domain definitions [42,50]. Throughout, the researchers made conscious efforts to reflexively question their own preconceptions and assumptions.
2.7. Techniques to Enhance Trustworthiness
For observations, a debriefing session was performed for member checking after each clinical encounter to fill in gaps and clarify what was observed during the clinical encounter [56]. Triangulation of the data was performed by asking therapists about PA promotional strategies during the interviews as well. A clear audit trail was performed throughout the research study, including research memos after each observation to document reflections and interpretations of the data as it was collected. Coding decisions and rationale were also documented throughout the coding process. Two coders were used to discuss and challenge assumptions and interpretations of codes.
3. Results
3.1. Study Participant Characteristics
Five physical therapists were each observed in two separate clinical encounters with different patients (n = 10 observations). Interviews were conducted after completion of both observations (n = 5). The participants were primarily female (80%), 25–34 years of age, and had over 5 years of experience (See Table 1). The patients treated by the therapists were primarily male (60%), recovering from a stroke (50%), and used an assistive device (40%). The mean age was 60.5 years of age and half had a caregiver present during the session (See Table 2).
3.2. Agreement Data
Interrater agreement after coding the first four observations was moderate (60%). To improve agreement, the two coders met and modified guidelines for coding to predefine the target activity behaviors for each observation and limit codes to apply towards promotion of home activity only. Coding was redone after adjustments and the resulting average interrater agreement of BCT coding between observation was 97.8% (range 92.4–100). Percent agreement was also calculated for each behavior change code used with average agreement of 91% and range of (70–100).
3.3. Aim 1: Characterization of BCT Use During Observations of Clinical Encounters
3.3.1. Observations
In total, a target activity behavior was promoted 35 times. The most frequently targeted home PA behaviors were resistance training with a home exercise program (14/35 40%) and walking activity (7/35 20%). Only (4/35 11%) of targeted behaviors were promoting aerobic activity. Specific activity prescription (including reps, frequency, duration, etc.) was performed more frequently when providing home exercise program printouts that were targeting resistance exercises (3/35), but infrequently for walking activity and aerobic activities (1/35). BCTs for PA promotion were largely carried out via conversations between the therapist and patient/caregiver.
Out of the BCT taxonomy, 27/93 types of BCTs were observed across clinical encounters. There were 80 instances of BCTs observed. The average BCTs used per clinical encounter was 8.0 techniques (range 4–15). The most common BCTs used across all clinical encounters were “instruction on how to perform the behavior” (10/10 encounters, 100%), “behavioral practice and rehearsal” (9/10 encounters, 90%), “social support” (8/10 encounters, 80%), “credible source” (6/10 encounters, 60%), “adding objects to the environment” (6/10 encounters, 60%), and “goal setting” (5/10 encounters, 50%) (Figure 1, Table 3). There was another technique noted that did not fit the BCT Taxonomy; however, the coders felt it was applied as strategy to promote the behavior. This prompted an additional code “behavior check-in for accountability”. “Behavior check-in for accountability” (6/10 encounters, 60%) was a strategy employed by therapists when they asked a patient if they had performed an activity at home. This was a verbal check-in and did not include any feedback, support, instruction, or monitoring and thus did not fit the taxonomy.
3.3.2. Behavior Change Strategies Reported During Interviews
Therapists were asked to describe strategies they used to promote PA. The strategies reported by the therapists largely coincided with observations. A total of 21 strategies were noted by therapists. Education was the most prominent strategy noted in every interview (5/5) by physical therapists which was coded in observations as “instruction on how to perform behavior” and “credible source”. Other prominent strategies that therapists reported using were building social support/relationships (4/5) and goal setting (4/5). These were observed in clinical encounters and coded as “social support” and “goal setting”. Therapists discussed using activity monitoring informally in interviews. However, this type of monitoring did not meet the qualifications of a true behavior change strategy as it was not specific or logged by the patient and, therefore, did not occur frequently in coding. Also, all therapists brought up using an individualistic approach by promoting activities that are salient and enjoyable to the patient. This approach did not have a direct BCT code to link to. A less prominent but identified strategy was incorporating exercise into daily routines (2/5) which included behavior substitutions and using visual cues to exercise. These approaches were present but not consistently used in observations. Lastly, “behavioral practice and rehearsal” and “adding objects to the environment” were prominent in clinical encounters but were not brought up as explicit strategies in interviews. A table indicating how therapist reported strategies mapped onto observed strategies can be seen in Table 4.
3.4. Aim 2: Physical Therapists’ Perspectives Regarding Promoting Home-Based Physical Activity After Discharge from Outpatient Services
Thirteen themes were generated for therapists’ perspectives regarding promotion of PA in the home/community setting that mapped onto eight TDF domains: (i) knowledge, (ii) memory, attention, and decision processes, (iii) professional role, (iv) beliefs about capabilities, (v) beliefs about consequences, (vi) goals/intentions, (vii) environmental context and resources, and (viii) social influences. Table 5 represents a summary of themes and relevant quotations. The TDF domains mapped onto all three components of the COM-B model. For a visual representation of themes and the mapping onto the COM-B and TDF, refer to Figure 2. For further information and a visual of coding trees, please refer to Appendix C.
(i) Knowledge: Two themes aligned with knowledge: (i) awareness of community resources and (ii) knowledge of PA prescription and BCT applications.
- a.Lack of awareness of community resources: Participants noted a lack of awareness of up-to-date community resources and referrals, particularly for patients living in areas unfamiliar to the participants. While the hospital network did have options for referrals such as adaptive sports or community gyms, therapists expressed that options for referrals are often spread by word of mouth. Overall, therapists share the perspective that there is a lack of knowledge regarding up-to-date, accessible, and specialized services as referral sources to promote PA after discharge.
- b.Limited knowledge of PA prescription and BCT applications: Therapists noted their knowledge of population-specific PA prescription was limited. While therapists mentioned general guidelines (American Heart Association or CDC), these did not always seem suitable for the neurological population. Furthermore, while therapists reported using general strategies to promote PA during practice (e.g., education, social support, goal setting), their knowledge regarding behavior change and specific techniques was limited. (ii) Memory, Attention, and Decision Processes: One theme aligned with this domain, clinical decision-making.
- a.Clinical decision-making impacts how PA is promoted: Participants discussed using information regarding patients’ diagnosis, body systems (e.g., cognition, strength, balance), activity level (e.g., community ambulator), and participation (e.g., social roles) to guide recommendations of PA in the home/community setting. Impairments that impacted safety and fall risk such as balance and cognition were viewed as concerns when promoting PA that would impact the level of difficulty and type of PA promoted. Acuity of diagnosis impacted how PA promotion was approached. For example, three of the therapists mentioned they believed their patients experienced fear and anxiety regarding managing a new injury or diagnosis independently, which is heightened when discharging from outpatient physical therapy as the last structured rehabilitation after an acute injury or event. This makes it more important to promote an independent activity plan at home to help manage this anxiety. This differs from the approach to individuals with chronic conditions, where it is expected they are already managing more independently. (iii) Professional role: Two themes were linked to professional role, (i) views on the physical therapist role in health promotion and wellness services and (ii) views on the physical therapist role in community activity and participation.
- a.Physical therapy has a limited role in health promotion and wellness: Therapists all recognized the importance of activity in this population and the increased risk of inactivity and secondary consequences that individuals with neurological conditions have. However, the majority had the perspective that engaging in prolonged PA in the home and community was an unskilled service and/or fell under the role of personal trainers.
- b.PT role is for education not motivation for community activity and participation: All therapists felt that it was part of their role to help their patients with community integration, and it was connected to a sense of fulfillment that therapists had in their profession in two of the interviews. Community integration might include things such as returning to work, socializing, or getting involved with community groups. While this did occasionally have an overlap with increasing activity levels, it was not directly related. In terms of promoting community or home-based activity, all therapists felt it was part of their role to educate patients on activities and provide resources to be active. However, therapists put responsibility for the motivation and follow-through of these activities on the patient. (iv) Beliefs about capabilities: There was one theme regarding beliefs about capabilities, which was self-efficacy with BCT use for PA promotion.
- a.Limited self-efficacy: Physical therapists did not feel confident in their ability to successfully utilize BCTs to motivate patients to be more active. In general, they felt they were unsuccessful in their attempts to do this in practice. (v) Beliefs about consequences: Two themes mapped onto beliefs about consequences including (i) beliefs about how patient motivations, expectations, and emotions could impact the results of PA promotion and (ii) beliefs about how the patient environment (physical, social, and caregiver) could impact the results of PA promotion. There was a belief that barriers in these two domains would have negative consequences on efforts for PA promotion.
- a.Belief that patient motivations, expectations, and emotions impact the results of PA promotion: Most (n = 4) physical therapists felt that patients who were not motivated were “challenging”, and it was very difficult or not possible to change a patient’s exercise behaviors. Therapists also mentioned that when patients have unrealistic expectations for recovery, this can hinder the ability to promote activities that are achievable.
- b.Belief that the patient environment (physical, social, and caregiver) could impact the results of PA promotion: All therapists noted that logistical and environmental barriers make it challenging to encourage exercise. Cost, geographic location, transportation, and time impacts access to activity programming. Inconsistency and limited availability of PCAs is also a consideration as many community activity centers, such as gyms and adaptive programs, require a person to assist with transfers. These cumulative logistical barriers contribute to the challenge of promoting PA in this population. (vi) Goals/Intentions: One theme of goals and intentions was identified, which was therapist activity prescription priorities.
- a.Activity prescription priorities impact type of PA promoted: The goal of activity prescription was variable across participants. Some participants (n = 3) reported the goal for PA after discharge was to promote a home exercise program while others (n = 2) felt it was more important to emphasize community integration. One therapist felt it was important to provide clear activity guidelines, while the remainder encouraged patients just to be active in some capacity. (vii) Environmental context and resources: The themes of reimbursement structures and resources and time mapped onto this domain.
- a.Limitations due to reimbursement structures: Most of the therapists had the impression that using treatment time for PA and wellness-based treatments was non-billable or non-skilled (n = 4). Therapists felt that insurance coverage dictates why this is not performed in practice.
- b.Limitations due to resources and time: Most therapists (n = 4) reported that limited time was a barrier, both in finding time amongst many competing priorities for this complex patient population and the amount of time it takes to have difficult conversations surrounding motivation. Additionally, the availability of programs and skilled trainers to refer patients to also impacts the ability to promote PA to patients. Even in a large hospital-based clinic, the majority of therapists (n = 4) reported that finding resources that are accessible, affordable, and have the proper specialized equipment and care can be challenging to come by. Conversely, one therapist reported that within her hospital network, she felt lucky there were resources available to her patients. (viii) Social influences: Two themes mapped onto social influences, (i) healthcare team dynamics and (ii) patient/therapist dynamics.
- a.Healthcare team dynamics can facilitate PA promotion: Therapists felt that healthcare team dynamics including the referring physician or physiatrist support make a big difference in the effectiveness of PA promotion. Therapists report that consistent messaging across the healthcare team on the importance of PA, meeting PA guidelines, and support in promoting activity outside of PT was a facilitator to PA promotion.
- b.The patient/therapist dynamic impacts PA promotion: Therapists also reported that the dynamic between the patient and the therapist was important. When there was a good rapport and aligned expectations on activity, PA promotion was easier to perform, expressed by PT5. However, misaligned expectations can make it challenging.
4. Discussion
Our study is the first study of physical therapists that included direct observation of clinical encounters and in-depth qualitative interviews of physical therapists to characterize the use of BCTs for PA promotion during treatment encounters with people with chronic neurological conditions, and identify physical therapists’ perspectives regarding promoting home-based PA as patients are discharged from skilled outpatient therapy. Several important findings emerged. First, the majority of PA promotion behaviors during discharge-planning clinical encounters targeted home exercise (e.g., strength training) or walking programs (e.g., practice walking with a cane); promotion of aerobic activity was limited. Second, an average of 8 BCTs per session were used by physical therapists to promote PA, of which the most commonly used strategies were (i) “instruction on how to perform the behavior”, (ii) “behavioral practice and rehearsal”, (iii) “social support”, (iv) “credible source”, (v) “adding objects to the environment”, and (vi) “goal setting”. Lastly, physical therapists’ perspectives about promoting PA for patients with chronic neurological conditions were influenced by knowledge, clinical decision-making, views on professional role, beliefs about capabilities, beliefs about consequences, goals/intentions for PA, environmental context and resources, and social influences.
None of the therapeutic clinical encounters included recommendations of activity levels meeting Center for Disease Control and Prevention (CDC) guidelines or other evidence-based activity recommendations for people with neurological conditions. Rather, recommendations for PA typically included functional activities, strengthening, and home walking programs. This approach, while typical for neurological physical therapy treatment [57], does not meet recommended levels of PA for this patient population. Furthermore, it was noteworthy that therapists were generally not aware of recommended PA levels that were achievable for individuals with complex neurological conditions. Our findings concur with others who found physical therapists had limited knowledge regarding PA and exercise prescription for people with chronic pain; [58]; however, other settings such as cardiac rehabilitation utilize these guidelines more routinely in practice [59]. Previous work also suggests that there could be a relationship between therapist exercise behavior and their knowledge of and willingness to promote PA [60]. However, this was not found as a theme in our sample. While there is no one guideline for all neurological conditions due to the variability across conditions, the American Academy of Physical Therapy Neurology Chapter released a toolkit in 2020 detailing up-to-date evidence on exercise prescription recommendations for multiple sclerosis, Parkinson’s disease, traumatic brain injury, spinal cord injury, stroke, Huntington’s disease, and amyotrophic lateral sclerosis [61]. Toolkits such as these may help providers make PA recommendations to patients with complex conditions.
The most extensively used BCTs, “instruction on how to perform the behavior,” “behavioral practice and rehearsal,” and “social support”, are linked to behavior change [21,62]; however, other BCTs (e.g., “self-monitoring” “adding objects to the environment”, “information about consequences”, “goal setting”, “problem solving”, “action planning”, “feedback on behavior”, and “biofeedback”) that may have a greater impact for people with chronic conditions [23,63] were rarely used. Interestingly, while goal setting for impairment-based goals is a major aspect of physical therapy rehabilitation, goal setting for PA behaviors outside of the clinic occurred in only half of the observations. This difference was highlighted in the dissonance noted between therapist reported strategies versus observations. This suggests that while goal setting is used regularly to guide and justify clinical intervention, goal setting to promote behavior change was not prominently used when helping patients develop home-based PA programs. The inclusion of goal setting and other BCTs may help patients engage in activity in the home [23]. However, therapist knowledge regarding behavior change theory and BCT was limited, which may have impacted therapists’ use of specific techniques to promote behavior change in clinical encounters. Our findings concur with findings in orthopedic physical therapy practice that there is limited knowledge of how to apply BCTs [64].
Similarly to others [65,66], therapists viewed promotion of community engagement and activity as part of their role, but there was mixed opinions on what this entails. All therapists felt responsible for education on resources, but felt that it was hard to know and access the resources available for patients, especially those with increased needs, socioeconomic barriers, and rural geographical locations. After referring and education, therapists mostly felt that it was up to the patient to be accountable on follow through when resources were provided and that continued monitoring of PA was not a “skilled” billable service. However, education alone is insufficient to generate behavior change, and recommendations for PA promotion should incorporate behavior science to facilitate PA change [60]. Additionally, the American Physical Therapy Association has released guidelines that skilled maintenance care and remote monitoring are billable under Medicare guidelines and health promotion should be part of physical therapy practice [67]. Overall, the state of current practice patterns is not aligned with the American Physical Therapy Association [68] or the World Confederation for Physical Therapy [69] goals for increasing focus on PA screening and promotion as part of physical therapy practice. Work must be completed to shape physical therapist views on their role in health promotion and to improve knowledge on how this is performed effectively. A health-focused physical therapy model (HFPTM) has been suggested for implementing health promotion in physical therapy practice, which highlights the need for integration of behavior change interventions [18]. This suggests that to change health behaviors such as PA, physical therapists need to be able to identify target domains of behavior that can be changed, apply effective behavior change strategies to these domains, and evaluate the clinical impact of behavior change strategies. However, the findings in this study suggest physical therapists lack the knowledge, training, and tools to follow these steps. This body of work should contribute to development of physical therapy trainings, continuing education, and curriculum to emphasize PA prescription for specialized populations, use of behavior change strategies and theory in practice, and the role of physical therapists in health promotion. Future research will also need to develop valid and sensitive outcome measures to evaluate and test BCTs as well as investigate the best methods for training and implementation into practice. Additionally, new care delivery models that can be delivered in the home setting to provide long-term behavior change strategies should be considered. Embedding technologies such as remote monitoring combined with behavioral consultation into maintenance care models could be considered to bridge this care gap [70,71].
Limitations: Our study has several limitations that are worthy of consideration. First, the sample is a small, convenience sample comprising therapists from one setting. This limitation in sample size may have led to missed perspectives or incomplete saturation. However, the setting in the study was from a large, academic hospital with extensive resources and training for staff which would suggest that the targeted setting would be representative of best practice for this population. In addition, two observations of different patients were observed for each therapist (n = 10), which provided repeated opportunities to observe therapists across patients. Nonetheless, the small sample may not be representative of the broader neurological outpatient setting. Second, the communications of physical therapists with their patients were not audio-recorded and the field note data collection approach may have missed data. Third, only one researcher observed the clinical encounter and recorded the field notes. It is is possible that the field notes reflected the biases of the observer; however, the observer was a clinician with expertise in this patient domain, so the investigator also brought strength in understanding clinical practice patterns.
5. Conclusions
The findings from this study indicated that an average of 8.0 BCTs were used during each session and the application of BCTs in neurorehabilitation was mostly applied towards home exercise programs. Specific guidelines and activity prescription were rarely applied to aerobic exercise. “Instruction on how to perform the behavior”, “behavioral practice and rehearsal”, and “social support” were noted in almost all the clinical encounters. However, key behavioral approaches that are linked to successful long-term change in PA behavior such as “self-monitoring”, “goal setting”, “problem solving”, “action planning”, and “feedback” [23] were used less than 50% of the time. From the interviews, we identified factors pertaining to domains of knowledge, decision process, professional role, beliefs about capabilities, beliefs about consequences, goals/intentions, environmental context and resources, and social influences that impacted BCT use for PA promotion [64]. This study was the first to characterize BCT use by PTs working with individuals with neurological conditions and highlighted the need for increased education and implementation efforts to integrate behavior change, PA prescription, and health promotion into routine practice. Targeted education, training, resources, and implementation efforts should be made to encourage physical therapists to use effective behavior change strategies that target long-term change in activity behaviors [72].
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Global, regional, and national burden of neurological disorders, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016 Lancet Neurol.20191845948010.1016/s 1474-4422(18)30499-x 30879893 PMC 6459001 · doi ↗ · pubmed ↗
- 2Kalb R. Brown T.R. Coote S. Costello K. Dalgas U. Garmon E. Giesser B. Halper J. Karpatkin H. Keller J. Exercise and lifestyle physical activity recommendations for people with multiple sclerosis throughout the disease course Mult. Scler. J.2020261459146910.1177/1352458520915629 PMC 757530332323606 · doi ↗ · pubmed ↗
- 3Ginis K.A.M. van der Scheer J.W. Latimer-Cheung A.E. Barrow A. Bourne C. Carruthers P. Bernardi M. Ditor D.S. Gaudet S. de Groot S. Evidence-based scientific exercise guidelines for adults with spinal cord injury: An update and a new guideline Spinal Cord 20185630832110.1038/s 41393-017-0017-329070812 · doi ↗ · pubmed ↗
- 4Billinger S.A. Arena R. Bernhardt J. Eng J.J. Franklin B.A. Johnson C.M. Mac Kay-Lyons M. Macko R.F. Mead G.E. Roth E.J. Physical Activity and Exercise Recommendations for Stroke Survivors Stroke 2014452532255310.1161/str.000000000000002224846875 · doi ↗ · pubmed ↗
- 5Kleindorfer D.O. Towfighi A. Chaturvedi S. Cockroft K.M. Gutierrez J. Lombardi-Hill D. Kamel H. Kernan W.N. Kittner S.J. Leira E.C. 2021 Guideline for the Prevention of Stroke in Patients with Stroke and Transient Ischemic Attack: A Guideline From the American Heart Association/American Stroke Association Stroke 202152 e 364e 46710.1161/STR.000000000000037534024117 · doi ↗ · pubmed ↗
- 6Gordon N.F. Gulanick M. Costa F. Fletcher G. Franklin B.A. Roth E.J. Shephard T. Physical Activity and Exercise Recommendations for Stroke Survivors Circulation 20041092031204110.1161/01.CIR.0000126280.65777.A 415117863 · doi ↗ · pubmed ↗
- 7Bhalsing K.S. Abbas M.M. Tan L.C.S. Role of Physical Activity in Parkinson’s Disease Ann. Indian Acad. Neurol.20182124224910.4103/aian.AIAN_169_1830532351 PMC 6238554 · doi ↗ · pubmed ↗
- 8Dalgas U. Stenager E. Exercise and disease progression in multiple sclerosis: Can exercise slow down the progression of multiple sclerosis?Ther. Adv. Neurol. Disord.20125819510.1177/175628561143071922435073 PMC 3302199 · doi ↗ · pubmed ↗