Increased Eplet Mismatch Load and Reduced Immunosuppressive Exposure Elevate the Risk of Baseline Lung Allograft Dysfunction
Victor M. Mora, Emilio Rodrigo, Elena González-López, Javier Gonzalo Ocejo-Vinyals, David San Segundo, David Iturbe-Fernández, Sheila Izquierdo, Sandra Tello, Marcos López-Hoyos, Maria Mar García-Saiz, Pilar García-Berbel, José M. Cifrián

TL;DR
Higher eplet mismatch and lower immunosuppressive drug levels increase the risk of poor lung function after lung transplants.
Contribution
Identifies eplet mismatch load and immunosuppressive exposure as novel risk factors for baseline lung allograft dysfunction.
Findings
BLAD patients had higher eplet mismatch burden compared to non-BLAD patients.
Lower tacrolimus TTR and MPA AUC0–12 levels were observed in BLAD patients.
DR/DQ eplet mismatches and MPA AUC0–12 were independently linked to worse lung function.
Abstract
Background/Objectives: Some lung transplant (LungTx) recipients do not achieve the expected lung function within the first year, a condition known as baseline lung allograft dysfunction (BLAD). Our objective was to analyze the risk factors associated with BLAD, focusing on the variables associated with a higher risk of developing a more intense alloimmune response. Methods: We carried out a prospective study including 88 LungTx recipients. BLAD was defined as failure to reach 80% of the predicted value for forced expiratory volume in one second (FEV1) and/or forced vital capacity (FVC) on two tests conducted at least three weeks apart. Tacrolimus time in therapeutic range (TTR) and mycophenolic acid area under the curve (MPA AUC0–12h) were measured at the third month. Donor–recipient compatibility was assessed using HLA eplet mismatch analysis, performed via HLA Matchmaker 3.1. Results:…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
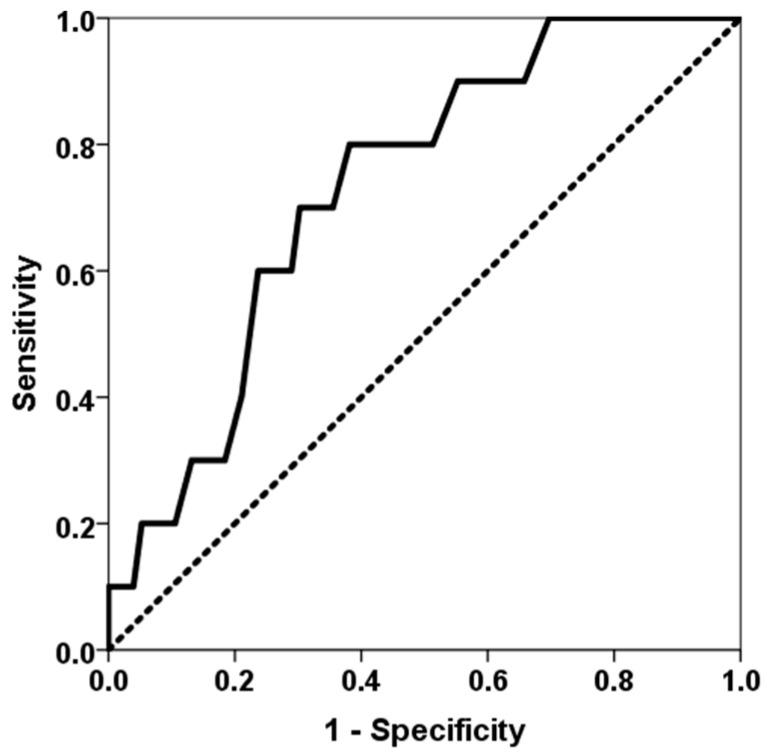 Figure 1
Figure 1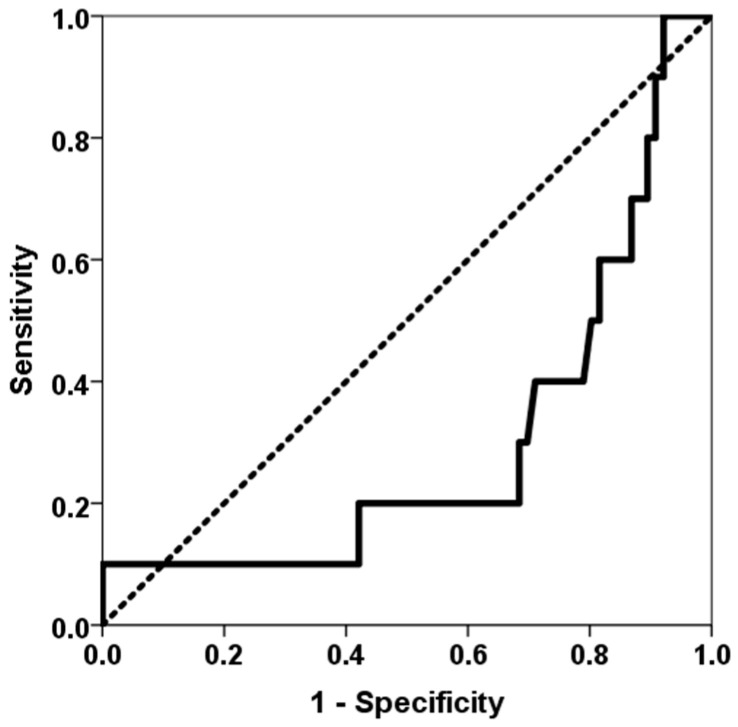 Figure 2
Figure 2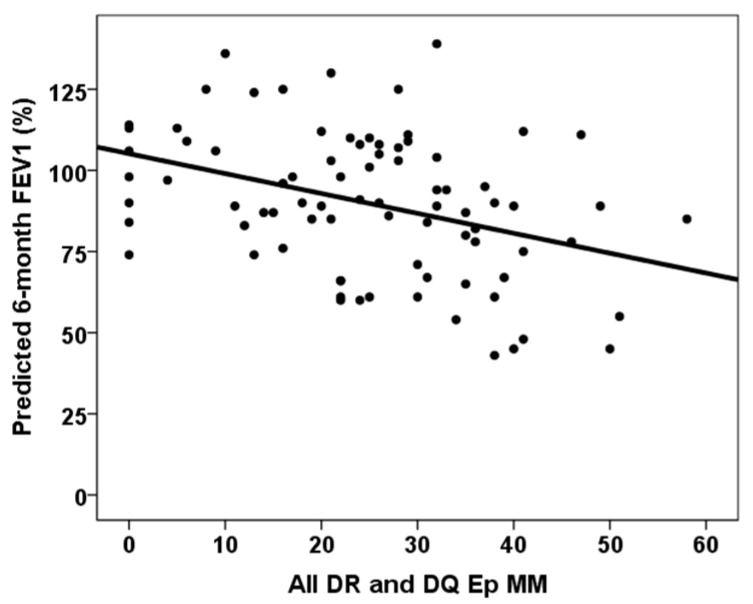 Figure 3
Figure 3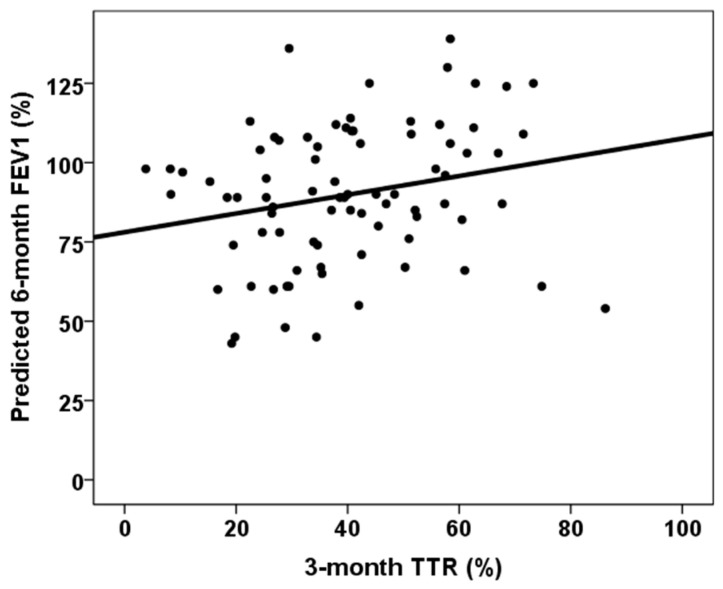 Figure 4
Figure 4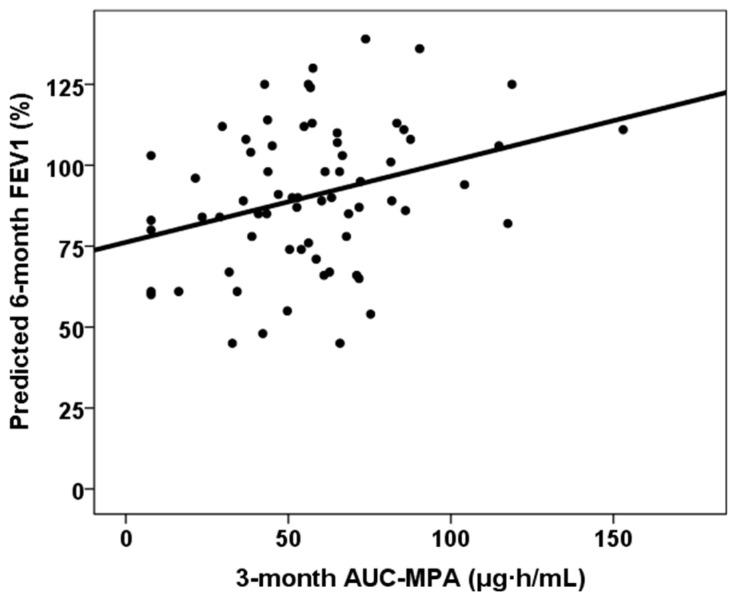 Figure 5
Figure 5- —Fondo de Investigaciones Sanitarias-ISCIII
- —RICORS2040
- —“Financiado por la Unión Europea—NextGeneration EU,” Mecanismo para la Recuperación y la Resiliencia [MRR]
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTransplantation: Methods and Outcomes · Renal Transplantation Outcomes and Treatments · Respiratory viral infections research
1. Introduction
A lung transplant (LungTx) is the preferred treatment option for patients with chronic respiratory diseases who have exhausted all available treatment options and have irreversible respiratory failure that limits their quality of life and life expectancy. The primary goal of lung transplantation is to restore normal lung function, thereby improving both quality of life and survival [1,2]. In most cases, the highest possible lung function is achieved between six and twelve months after transplantation [3]. However, some lung transplant recipients do not achieve the expected lung function within the first year, a condition known as baseline lung allograft dysfunction (BLAD) [4]. The presence of BLAD is linked to a diminished quality of life and an increased risk of chronic lung allograft dysfunction (CLAD) and mortality [4,5,6].
The risk factors associated with partial lung function recovery and BLAD are not yet fully understood. It has been established that certain postoperative recovery variables are associated with an elevated risk of BLAD. These include severe primary graft dysfunction (PGD), mechanical ventilation time, ICU length of stay, initial admission stay length and perioperative blood loss. Furthermore, there is an established correlation between certain donor and recipient variables and BLAD, as well as diminished lung function. These variables include interstitial lung disease as native pulmonary disease, heavy donor smoking, donor age and sex, recipient younger age and recipient obesity [1,2,4,6,7,8,9,10,11].
As BLAD relates to a higher CLAD risk, it is reasonable to hypothesize that both may share some common pathogenic causes. Research has demonstrated a clear association between CLAD and a stronger alloimmune response when considered alongside other variables. Research has indicated that cellular and antibody-mediated rejection episodes, pretransplant and de novo donor-specific antibodies (DSAs), the number of HLA mismatches, and the intensity and adherence to immunosuppressive therapy have been reported as factors associated with CLAD risk [12,13,14,15,16]. It is important to note that some of these variables, such as acute rejection or de novo DSAs, have not been associated with a higher BLAD risk, and their association is controversial. In addition, other variables have not been analyzed in depth [2,17]. Furthermore, various studies have identified discrepancies in the relationship between a well-identified biomarker of alloimmune damage in the lung allograft, such as cell-free DNA, and BLAD [6,18]. The objective of our study was to analyze whether variables associated with a higher risk of developing a more intense alloimmune response, such as greater HLA eplet mismatch number and lower exposure to immunosuppressive drugs, were associated with a higher risk of BLAD.
2. Materials and Methods
A prospective study was conducted involving all patients (88, 45 male and 43 female; mean age 60 ± 8 years) who underwent lung transplantation at our center between January 2021 and April 2023 and consented to participate. The study was conducted in accordance with the principles outlined in the Declaration of Helsinki and received approval from the institution’s Regional Ethics Committee (PI20/01710; approved on 22 December 2020). Each participant received a bilateral lung transplant from a deceased donor. Post-transplant immunosuppressive treatment comprised mycophenolate mofetil (1000 mg every 12 h), corticosteroids and tacrolimus, targeting trough levels of 12–15 ng/mL during the first six months. Basiliximab was used as induction therapy, and all patients were given azithromycin as a preventive measure against CLAD.
Data on recipient, donor, transplant-related characteristics and clinical outcomes were collected prospectively from electronic health records (see Table 1). Recipient and donor HLA class-I (A, B, C) and class-II (DR, DQ) typing was performed by a high-resolution sequence-specific primer (Life Technologies, Brown Deer, WI, USA). Donor–recipient compatibility was assessed using HLA eplet mismatch analysis, performed via HLA Matchmaker 3.1 (accessible at http://www.epitopes.net/downloads.html, accessed 1 April 2024). Acute rejection was diagnosed in accordance with the ISHLT Working Formulation, based on findings from transbronchial biopsies [19]. Primary graft dysfunction (PGD) was defined and staged per ISHLT guidelines [20]. Baseline lung allograft dysfunction (BLAD) was defined as failure to reach a minimum of 80% of the predicted value for forced expiratory volume in one second (FEV1) and/or forced vital capacity (FVC) on two tests conducted at least three weeks apart within the first year following transplantation [4].
Tacrolimus trough levels (ng/mL) in whole blood were analyzed using a chemiluminescent microparticle immunoassay on the Architect iSystem (CMIA; Abbott Laboratories, Abbott Park, IL, USA). These levels were recorded up to 90 days post-transplant. The time in therapeutic range (TTR), defined as the proportion of time within 12–15 ng/mL, was calculated using the Rosendaal method [13]. Variability in tacrolimus levels was expressed as the coefficient of variation (CV), using the formula
where σ is the standard deviation and μ is the mean tacrolimus level [21]. The cumulative tacrolimus exposure at three months was estimated by calculating the area under the curve (AUC) of all trough concentrations from the time of transplant to month three [22].
Plasma trough concentrations of mycophenolic acid (MPA) were measured using a homogeneous enzyme immunoassay (Emit 2000; Siemens, Munich, Germany). The full MPA AUC_0–12h_ at three months was estimated using a limited sampling strategy at time points 0, 30 min and 2 h after administration, as described by Pawinski et al. [23]. This measurement was available for 72 patients; 3 declined the procedure and 11 were no longer taking MPA by month three.
Peripheral blood was collected from transplant recipients three months after their transplant using Streck Cell-Free DNA BCT tubes. Plasma was obtained by centrifuging the blood at 1600× g for 20 min, followed by 16,000× g for a further 10 min. Cell-free DNA was then isolated using a QIAamp Circulating Nucleic Acid Kit (Qiagen, Redwood City, CA, USA). A targeted next-generation sequencing (NGS) panel assessing 202 single-nucleotide polymorphisms (SNPs) (AlloSure^®^, CareDx, Brisbane, CA, USA) was used to determine the relative level of cell-free DNA (cfDNA). Sequencing was performed using Illumina MiSeq equipment, and the results were analyzed using AlloSeq cfDNA software version 1.0 (CareDx). A dd-cfDNA level of ≥1.0% was considered abnormal, in line with the manufacturer’s recommendations.
Statistical Methods
Continuous variables were summarized using medians and interquartile ranges (IQRs), while categorical variables were reported as proportions. The chi-squared test was used to assess relationships between categorical variables. Spearman’s rank correlation was applied to explore associations between continuous variables. Differences in continuous outcomes between the two groups were tested using the Mann–Whitney U test. Linear regression analyses (both univariate and multivariate) were conducted to identify variables associated with lung function at six months. A p-value of less than 0.05 was considered statistically significant. All analyses were performed using SPSS software (version 22.0; SPSS, Inc., Chicago, IL, USA).
3. Results
The study included 88 lung transplant recipients who underwent surgery between January 2021 and April 2023. Two patients died during the immediate postoperative period, and ten patients (11.6%) met the criteria for BLAD. The main patient characteristics and their comparison between patients with and without BLAD are shown in Table 1. A higher proportion of BLAD recipients were female, younger and had received more lung grafts from female donors. Patients who developed BLAD experienced longer ventilation times after surgery, as well as longer stays in the ICU and at initial admission. A higher number of class-I and class-II HLA mismatches was associated with a higher BLAD risk (AUC ROC 0.732, 95% CI 0.590–0.873, p = 0.018) (Figure 1). Lower time in the therapeutic range of tacrolimus was associated with a higher BLAD risk (AUC ROC 0.299, 95% CI 0.117–0.480, p = 0.039) (Figure 2). Furthermore, BLAD patients were less likely to receive an adequate dose of MPA above 30 mg × h/L. As expected, pulmonary function parameters six months after transplantation were significantly lower for patients with BLAD.
The correlation between continuous variables and six-month predicted forced vital capacity (FVC) and forced expiratory volume in one second (FEV1) is shown in Table 2. All DR and DQ Ep MM, third-month % time in therapeutic range and third-month MPA AUC_0–12_ showed statistically significant correlations with both six-month predicted FVC% and FEV1%. Figure 3, Figure 4 and Figure 5 show the relationship between six-month predicted FVC%, all DR and DQ epitope mismatches, third-month percentage time in therapeutic range and third-month MPA AUC_0–12_, respectively. Female recipients were associated with a lower six-month predicted FVC% (93.0, RIC 30.0 vs. 87.0, RIC 26, p = 0.029), but not with a lower six-month predicted FEV1% (90.0, RIC 33 vs. 89.0, RIC 30, p = 0.268). In a similar manner, female donors were associated with a lower predicted 6-month FVC% (92.0, RIC 30.0 vs. 87.0, RIC 29, p = 0.034), but not with a lower predicted 6-month FEV1% (92.5, RIC 35 vs. 89.0, RIC 31, p = 0.296). Patients with cellular rejection and PGD3 did not show worse pulmonary function test results at six months (p > 0.05). Lung transplant recipients with COPD as the underlying lung disease showed a higher six-month predicted FVC% (86.0, RIC 31 versus 92.0, RIC 30, p = 0.011) and six-month predicted FEV1% (86.0, RIC 29 versus 103.0, RIC 27, p = 0.001). Those with ILD as the native lung disease showed a lower predicted FEV1% at six months (97.5, RIC 34 vs. 88.0, RIC 30, p = 0.032), but no significant difference in predicted FVC%. Patients in the lowest quartile of TTR showed a lower six-month predicted FVC% (80.5, RIC 27 vs. 92.5, RIC 25, p = 0.001), but a similar six-month predicted FEV1% (89.0, RIC 32 vs. 90.0, RIC 34, p = 0.103).
Table 3 shows the results of the multivariate linear regression analysis for six-month predicted FVC% and six-month predicted FEV1%. The models included female recipient sex (only for six-month predicted FVC%), interstitial lung disease (ILD) as the native lung disease (only for six-month predicted FEV1%), ventilation length, all donor–recipient DR and DQ epitope mismatches (All DR and DQ EpMM) and time in the therapeutic range. A second model included the MPA AUC_0–12_ at three months for the 72 lung transplant recipients for whom data were available. DR and DQ eplet mismatches and third-month MPA AUC_0–12_ were independently associated with six-month predicted FVC% and FEV1%.
4. Discussion
Although the exact causes of BLAD are not fully understood, most studies have found that damage to the lung graft during the initial post-transplant period makes it difficult to achieve maximum lung function. Therefore, consistent with previous studies, we found that patients requiring prolonged mechanical ventilation and ICU and initial hospital stays were at a higher risk of BLAD [2,5,9,11]. However, we did not observe an association between BLAD and a higher proportion of severe PGD or longer second lung ischemia time, in line with the findings of Mohanka et al. and Keller et al. [1,5,6,7,11]. Of the various variables analyzed, we found that younger recipient age increased the risk of developing BLAD, as previously reported [2,6,7]. Due to body size adjustment between donors and recipients during matching, lung grafts from female donors are commonly used for female recipients. We found that both female recipients and donors were associated with a higher BLAD risk. In our series, however, we found no relationship between BLAD and other previously identified variables such as older donor age, interstitial cause of lung disease, and body size of both donor and recipient, probably due to the low number of BLAD cases identified [2,4,5,6,7,11]. Like other authors, we also found no association between BLAD and donor smoking [5,6], although previous studies have observed an association between severe tobacco use (>20 pack-years) and BLAD. Our practice is to accept donors with a lower tobacco burden (<10 pack-years) [4,7,10,11].
Our most significant finding was that variables linked to an increased risk of a more severe alloimmune response, such as greater HLA donor–recipient mismatches and reduced exposure to tacrolimus and MPA immunosuppressive therapy, were associated with an elevated risk of BLAD. Patients with BLAD had a higher number of class-I and class-II mismatches overall, and this epitope discordance load demonstrated the ability to determine whether patients might develop BLAD, with an area under the ROC curve of 73%. However, a previous prospective study by Keller et al. involving 173 lung transplant recipients found that the degree of HLA mismatch at the antigenic level between donor and recipient was not associated with BLAD risk [6]. However, our study showed that analyzing epitope differences increases sensitivity in predicting the appearance of alloimmune responses. Similarly, while several studies have not related BLAD to rejection or DSA development [1,2,6], a more recent study has shown that the appearance of DSAs doubles the risk of BLAD, even in DSA-positive patients without evidence of antibody-mediated rejection (OR 2.14, 95% CI 1.45–3.17, p = 0.0001) [17]. Therefore, our findings suggest that BLAD is related not only to initial damage but also to an impending alloimmune response that limits improvement in functional tests. Furthermore, patients with BLAD spent less time within the appropriate tacrolimus therapeutic range (12–15 ng/mL). Notably, patients in the first quartile of time in the therapeutic range (<26.7%) were three times more prevalent in the BLAD group. Similarly, patients with a mycophenolic acid area under the curve of >30 mg × h/L in the third month, which represents a cut-off point associated with adequate exposure to mycophenolate and fewer complications following kidney transplantation, were significantly more prevalent in the non-BLAD group [24]. These findings suggest that more intense immunosuppressive therapy could reduce the incidence of BLAD in cases involving higher HLA mismatch between donor and recipient. However, the small number of BLAD patients limited our ability to perform a multivariate analysis to determine whether these associations were independent of other confounding variables.
To overcome this limitation, we analyzed which variables were associated with predicted pulmonary function tests at month six, which directly relate to the definition of BLAD. As mentioned in Table 2 and Table 3, indicators of greater initial damage, such as a longer duration of mechanical ventilation, ICU and hospital stays, and cold ischemia time, were associated with lower predicted FVC and FEV1 values at month six. These relationships have been reported previously by Yoon et al. and Mohanka et al., and as mentioned above, are explained by residual lung graft damage caused by a complicated early postoperative course [1,8]. Therefore, improving surgical times could contribute to better subsequent lung function and reduce the risk of BLAD. However, the most significant finding of our study was the association between an intense alloimmune response and impaired lung function during the initial year after transplant. In an aforementioned study, Alnababteh et al. reported a relationship between DSAs and CLAD and found that DSA+ lung transplant recipients (most of whom had anti-DQ antibodies) exhibited a significantly lower rate of post-transplant spirometric improvement and declining FVC% and FEV1% slopes after DSA development compared with DSA-negative patients [17]. In line with this finding, we found that greater eplet mismatching, primarily class-II, between donor and recipient increased the risk of poorer lung function at month six independently.
The influence of HLA eplet mismatching on lung transplant outcomes for the development of CLAD, dnDSA and long-term graft survival has been previously reported [16]. However, this influence has not been analyzed for such an early phase of lung grafting. Our findings suggest that measuring eplet mismatch load for all donor–recipient pairs could improve the functional outcomes of lung transplantation by enabling more intensive immunosuppressive strategies to be employed, thereby improving medium- and long-term prognoses.
Importantly, we observed that lung transplant recipients could benefit from greater exposure to MPA than from higher exposure to calcineurin inhibitors. The area under the curve for MPA levels at month three was associated with better lung function test results at month six, independent of the other variables. As previously explained, patients with adequate MPA levels were also less likely to experience BLAD. This relationship was not observed with MMF levels alone, which highlights the importance of measuring the area under the curve for MPA at least once after lung transplantation to optimize treatment and improve lung function during the first year. Although mycophenolic acid and mycophenolate mofetil are usually administered at a fixed dose in routine clinical practice for monitoring solid organ transplant recipients, therapeutic drug monitoring to maintain an MPA AUC_0–12h_ of between 30 and 60 mg × h/L has been shown to prevent both acute rejection and toxicity after kidney transplantation [24]. The relationship between MPA exposure and the course of lung transplantation has not been studied in depth. Interestingly, Yabuki et al. reported that among 59 lung transplant recipients, those with CLAD had been exposed to significantly lower MPA AUC 0–12 values (21 ± 10) than the event-free group (30 ± 7), whereas those with infections had higher values (37 ± 11) [14]. Notably, the authors did not find any relationship between tacrolimus exposure and CLAD development.
Although our data suggest that BLAD patients may be experiencing greater alloimmune damage, we did not find that the percentage of circulating dd-cfDNA, a marker of molecular graft injury, was elevated in BLAD patients, or that higher values were associated with poorer lung function at month six. Similarly to our findings, Keller et al. reported that neither the percentage value of dd-cfDNA nor its reduction over the first 90 days post-transplant was related to a higher risk of BLAD. They argued that BLAD is a highly heterogeneous process influenced by both parenchymal and extraparenchymal lung diseases, as well as the physical state of the patient [6,7]. Interestingly, we found that the percentage of patients with dd-cfDNA values above 1% was almost double in BLAD patients compared with non-BLAD patients. However, this difference was not statistically significant, which could be because of the small number of BLAD patients. Recently, Zajacova et al. reported that BLAD patients had significantly higher absolute dd-cfDNA levels (39 cp/mL vs. 26 cp/mL, p = 0.01) than non-BLAD patients. However, the percentage of dd-cfDNA did not differ significantly between the two groups (0.23% vs. 0.15%, p = 0.2). The authors demonstrated that absolute dd-cfDNA (OR 3.121, 95% CI 1.444–6.987, p = 0.004) but not the percentage of dd-cfDNA had significant predictive value for BLAD [18]. Therefore, subclinical lung allograft injury throughout the first post-transplant year may be associated with BLAD. However, the most effective method of measuring molecular graft injury by analyzing dd-cfDNA (absolute versus percentage) is still under debate.
The main limitation of our study was the small number of patients included, which was partly due to the single-center approach. Nevertheless, we conducted a prospective study focusing on our lung transplant population. For the first time, we analyzed the HLA eplet discordance load between donor and recipient, as well as the continuous exposure to immunosuppressive drugs such as tacrolimus and MPA, in this population. Furthermore, the results were limited by the low incidence of BLAD (12%), which is lower than other studies that reported incidences of greater than 27% [2,4,6,9,11,18]. While we have no definitive explanation for our low BLAD incidence, organ procurement, preservation and surgical procedures are carried out with particular care at our center. In addition, donor–recipient matching is performed with special attention. In two recent studies from our group, we showed that differences in donor–recipient total lung capacity of more than 20% were present in only 10% of cases, and such discrepancies had no impact on survival or the risk of developing CLAD when analyzed separately [25,26]. Moreover, almost 80% of the pairings were sex-matched, which may also contribute to reducing functional mismatches after transplantation. Regarding donor characteristics, nearly two-thirds had never smoked, and the median donor age was 56 years. These data suggest that strict donor selection, with emphasis on age, sex and anthropometric compatibility, could partly explain the relatively low incidence of BLAD observed in our cohort. Additionally, all our lung transplant recipients received azithromycin prophylaxis, which reduces the risk of BLAD by almost half (OR 0.53, 95% CI 0.33–0.85, p = 0.046) [27,28]. Our study links the presence of BLAD with lower exposure to immunosuppressive drugs and a higher burden of HLA mismatch between donor and recipient, suggesting that alloimmunity mechanisms may contribute to its development. Consequently, another relevant limitation is the absence of a systematic histological study to determine whether patients with BLAD experience more underlying rejection. Finally, because of our findings, it would have been very interesting to record tacrolimus blood levels beyond the third month to know its influence on the appearance of BLAD throughout the first-year post-transplant.
5. Conclusions
In conclusion, our study is the first to analyze the influence of donor–recipient mismatch and exposure to immunosuppressive drugs on the risk of BLAD and poor early lung graft function. Our findings suggest that BLAD is related not only to early graft damage but also to an underlying alloimmune response. We found that among other variables, greater eplet discordance, especially class-II, was associated with a higher risk of BLAD, as well as worse predicted FVC% and FEV1% at month six. Furthermore, we observed, for the first time, that higher MPA exposure was associated with a lower risk of BLAD and better subsequent lung function. If confirmed in subsequent studies, these findings highlight the importance of determining eplet discordance in lung transplant recipients to optimize immunosuppressive therapy for those with greater discordance. One potential strategy could be to specifically measure the area under the MPA curve to identify those with low MPA exposure who are at a higher risk of BLAD and poorer lung function and could benefit from dose adjustment by MPA AUC_0–12h_.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Mohanka M.R. Kanade R. Garcia H. Mahan L. Bollineni S. Mullins J. Joerns J. Kaza V. Torres F. Zhang S. Significance of Best Spirometry in the First Year After Bilateral Lung Transplantation: Association with 3-Year Outcomes Transplantation 20201041712171910.1097/TP.000000000000304632732851 PMC 7373484 · doi ↗ · pubmed ↗
- 2Hage R. Steinack C. Schuurmans M.M. Baseline Lung Allograft Dysfunction: Real-World Data for an Emerging Early Posttransplant Clinical Phenotype Exp. Clin. Transplant.20252340941410.6002/ect.2025.009740626822 · doi ↗ · pubmed ↗
- 3Bando K.O. Paradis I.L. Keenan R.J. Yousem S.A. Komatsu K. Konishi H. Guilinger R.A. Masciangelo T.N. Pham S.M. Armitage J.M. Comparison of outcomes after single and bilateral lung transplantation for obstructive lung disease J. Heart Lung Transplant.1995146926987578177 · pubmed ↗
- 4Liu J. Jackson K. Weinkauf J. Kapasi A. Hirji A. Meyer S. Mullen J. Nagendran J. Lien D. Halloran K. Baseline lung allograft dysfunction is associated with impaired survival after double-lung transplantation J. Heart Lung Transplant.20183789590210.1016/j.healun.2018.02.01429602706 · doi ↗ · pubmed ↗
- 5Verleden G.M. Bos S. The ABC of transplant: ALAD, BLAD, and CLAD: Definition and significance Curr. Opin. Pulm. Med.20253139740310.1097/MCP.000000000000117040165763 · doi ↗ · pubmed ↗
- 6Keller M.B. Sun J. Alnababteh M. Ponor L. Shah P.D. Mathew J. Kong H. Charya A. Luikart H. Aryal S. Baseline Lung Allograft Dysfunction After Bilateral Lung Transplantation Is Associated with an Increased Risk of Death: Results from a Multicenter Cohort Study Transplant. Direct 202410 e 166910.1097/TXD.000000000000166938953039 PMC 11216668 · doi ↗ · pubmed ↗
- 7Li D. Weinkauf J. Kapasi A. Hirji A. Varughese R. Lien D. Nagendran J. Halloran K. Baseline lung allograft dysfunction in primary graft dysfunction survivors after lung transplantation Respir. Med.202118810661710.1016/j.rmed.2021.10661734571454 · doi ↗ · pubmed ↗
- 8Yoon B.R. Park J.E. Kim C.Y. Park M.S. Kim Y.S. Chung K.S. Song J.H. Paik H.C. Lee J.G. Kim S.Y. Factors Associated with Lung Function Recovery at the First Year after Lung Transplantation Yonsei Med. J.2018591088109510.3349/ymj.2018.59.9.108830328324 PMC 6192893 · doi ↗ · pubmed ↗