Diagnostic and Therapeutic Management of Mesothelioma of the Tunica Vaginalis Testis: A Population-Based Study in Italy
Giovanni Luca Ceresoli, Simona Stella, Barbara Dallari, Riccardo Perduri, Cinzia Storchi, Luigi Vimercati, Sara Piro, Lucia Giovannetti, Ugo Fedeli, Veronica Casotto, Enrica Migliore, Antonella Stura, Carlo Genova, Lucia Benfatto, Francesca Larese Filon, Flavia D’Agostin

TL;DR
This study analyzes the diagnosis and treatment of a rare testicular tumor called mesothelioma of the tunica vaginalis testis in Italy, finding surgery as the main treatment with limited success from additional therapies.
Contribution
This is the largest population-based study on MTVT, providing detailed clinical data and survival analysis from a national registry.
Findings
The median survival for MTVT patients was 26.2 months with a 49% 3-year survival rate.
Surgery was the primary treatment, but adjuvant therapy was associated with higher mortality.
Older age and distant metastasis were identified as negative prognostic factors.
Abstract
Mesothelioma of the tunica vaginalis testis (MTVT) is an extremely rare tumor, for which only case reports, small case series and case reviews have been published. To our knowledge, this is the largest population-based study on MTVT, including rigorous assessment of asbestos exposure and a full review of medical records with detailed clinical data on diagnosis and treatment. This study was based on data extraction from the Italian Mesothelioma Registry (Registro Nazionale Mesoteliomi, ReNaM) dataset and confirmed the extreme rarity of MTVT, with a crude incidence rate in 1994–2021 of 0.17 per million person-years in Italy. Epidemiological characteristics of the disease included late age onset, prevalent epithelioid histology and relationship with predominantly occupational exposure to asbestos. Overall median survival was 26.2 months. Surgery was confirmed as the cornerstone of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
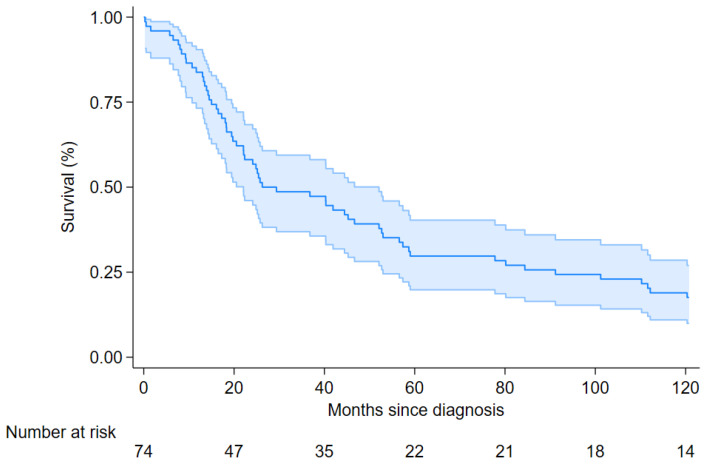 Figure 1
Figure 1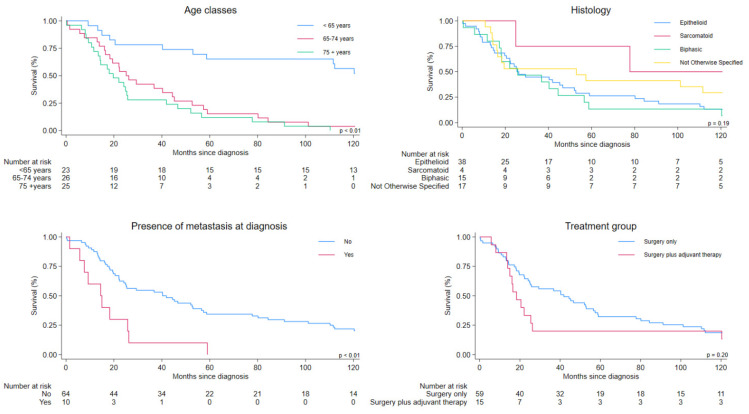 Figure 2
Figure 2- —Italian Insurance Against Accidents at Work (INAIL: Istituto Nazionale per l’Assicurazione contro gli Infortuni sul Lavoro)
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOccupational and environmental lung diseases
1. Introduction
In 2009, the International Agency for Research on Cancer (IARC) identified additional asbestos-related tumor sites: to lung cancer and mesothelioma of all sites, laryngeal and ovarian cancers have been added [1].
Mesothelioma of the tunica vaginalis testis (MTVT) is an extremely rare cancer arising from the serosal membrane lining the cavities of the scrotum, and accounting for less than 1% of all mesotheliomas [2,3,4,5]. The SEER (Surveillance, Epidemiology and End Results) Program from the US National Cancer Institute estimated for MTVT a mean annual standardized incidence rate in 1973–2013 of 0.054 per million person-years [6]. In Italy, in the 1993–2015 period, the mean standardized (world standard population as reference) incidence rate of the disease was 0.095 per million person-years [7]. Asbestos is an established risk factor; in a recent study on 80 patients, occupational exposure to asbestos was found for 47 (59%) cases and associated with a three-fold increased risk of MTVT [7]. Trauma, prolonged inflammation and recurrent hydrocele have also been correlated with the development of the disease [8].
Due to the rarity of MTVT, only case reports and small case series have been published so far [9,10], hampering the development of new knowledge and expertise, and particularly of a recognized diagnostic and therapeutic algorithm. Clinical presentation of MTVT is unspecific; the most frequent signs and symptoms at the onset are a testicular/scrotal mass or swelling, hydrocele and pain [2,3,4]. A timely, extensive surgical treatment is currently considered the best option of care [11,12], but the role of adjuvant treatments (including local radiotherapy and/or chemotherapy or other systemic treatments) remains undefined [2,3,4]. Preoperative imaging with scrotal ultrasonography and abdominal CT scan may reveal subtle anomalies in the tunica surface or more overt soft-tissue masses [2,3,4]. However, preoperative diagnosis can be challenging, and most cases are diagnosed incidentally during surgery or after the pathological examination [3]. Only a few cases of metastatic MTVT have been reported. The benefit of systemic treatments in these patients is unclear, as they were excluded from the main trials in mesothelioma [13,14,15], which have established the current standard therapy of unresectable pleural mesothelioma.
Rare cancers pose challenges for uncertainty of diagnosis, lack of established therapies, poor research opportunities and difficulties in clinical trials [16]. For these reasons, patients with rare tumors frequently face delays in diagnosis and care, and receive suboptimal treatment [17]. For these cancers, centralized data collection by population-based registries remains fundamental in reporting patient care and outcomes in the real world. Here, we report the results of an analysis of clinical data of a large series of MTVT patients, systematically recorded by the Italian National Mesothelioma Registry (ReNaM, Registro Nazionale Mesoteliomi) from 1994 to 2021. This study aimed to review the diagnostic and therapeutic management of these patients, with the ultimate goal to improve the knowledge on natural history and clinical approach to this rare cancer.
2. Materials and Methods
2.1. Study Design, Participants and Data Sources
This study is based on data extracted from the Italian Mesothelioma Registry (Registro Nazionale Mesoteliomi, ReNaM) dataset. ReNaM is a population-based registry that collects information on individuals with mesothelioma (any site: pleura, peritoneum, pericardium and tunica vaginalis testis) from all regions in Italy [18]. It is organized as a network of 21 regional centers (Centri Operativi Regionali, COR), which periodically send information to the ReNaM; some regions started collecting mesothelioma cases in 1993, others started later [18]. Reporting of mesothelioma cases to CORs is compulsory by law (277/1991 and 81/2008) [18]. However, to ensure complete reporting, an active search of mesothelioma cases is routinely performed by exploiting several sources, including hospital discharge records and mortality datasets. Hospital medical records regarding mesothelioma are reviewed by each COR. Patients or their next-of-kin are interviewed using a standardized questionnaire by qualified personnel to investigate lifetime occupational and non-occupational asbestos exposure. Asbestos exposure is evaluated and classified according to ReNaM guidelines as: occupational, non-occupational (including familial, environmental and leisure-related) and not exposed [18].
2.2. Variables and Outcomes
For each case of MTVT, the following variables are routinely recorded by ReNaM: year of diagnosis, patient age at diagnosis, histological subtype (epithelioid, biphasic, sarcomatoid), source of asbestos exposure and modality of exposure evaluation (with direct or indirect interview). Additional clinical information include clinical presentation, presence of distant metastases at diagnosis and therapeutic management, including the type of surgical intervention and adjuvant therapies (chemotherapy and/or loco-regional radiotherapy) administered.
For all patients, we ascertained vital status and date and cause of death information as of 31 December 2023.
2.3. Statistical Analysis
A descriptive analysis of patient characteristics was performed. We calculated crude and standardized rates for the period 2000–2021 using the standard European (2013) and world (Segi’s) populations. Patients with no treatment information were excluded from further analyses. Overall survival was measured from the date of diagnosis to the date of death from any cause. Follow-up time was truncated at 10 years after the diagnosis. To evaluate potential risk factors, we performed Kaplan–Meier analysis and fitted multivariate Cox regression models to calculate hazard ratios (HR) and 95% confidence intervals (CI) for selected variables, including age at diagnosis (<65, 65–74, and ≥75 years), period of diagnosis (1994–1998, 1999–2004, 2005–2010, 2011–2016, 2017–2021), histotype, presence of distant metastasis at diagnosis (no vs. yes) and treatment group (surgery only or surgery plus any adjuvant therapy). All statistical analyses were performed using Stata 18, StataCorp, TX, USA [19].
3. Results
Between January 1994 and December 2021, 104 cases of MTVT were registered by ReNaM. The crude rate was 0.17 per million person-years, and rates standardized based on European and world populations were 0.18 and 0.08, respectively. Patient baseline characteristics are shown in Table 1. Overall, median age was 72 years (range 17–92), with nearly 70% of patients older than 65 years. Epithelioid histotype was the most frequent, being diagnosed in 54 (52%) cases in the whole population. Nearly half of patients received a direct interview for exposure evaluation. Previous asbestos exposure, almost exclusively occupational, was identified in two thirds of evaluated cases. Among unexposed cases, no clusters of residents in geographical areas known for the presence of naturally occurring asbestos were found. Median latency (years between first exposure and diagnosis) was 54 years (13–75) in occupationally exposed cases. In patients with other sources of exposure, latency was between 30 to 60 years.
Complete data on therapeutic management were available for 74 cases (71%); no differences were observed between this subgroup and the whole case list regarding age, histological subtype and asbestos exposure.
Table 2 summarizes the clinical characteristics of these 74 patients. The most frequent presentation was a scrotal or testicular swelling or mass, observed in 52 of 74 cases (70%), followed by the presence of hydrocele (46 patients, 62%). Scrotal or inguinal pain was reported in a minority of cases (17 patients, 23%). Unexpectedly, imaging evaluation, including, in most patients, scrotal and abdominal ultrasonography and chest and abdominal computed tomography scans, detected distant metastasis at diagnosis in one out seven patients (14%). In the majority of cases (70%), metastasis site was the lung. Only 19 patients (26%) had a pre-operative histological diagnosis of mesothelioma.
All patients underwent surgery (Table 3), mostly with orchi-funicolectomy (58 cases, 78%). A few patients (7, 10%) were treated with a more extended surgery including orchi-funicolectomy, hemiscrotectomy and homolateral inguinal lymphadenectomy. Eight patients (11%) underwent minor surgical procedures, while for one patient the extent of surgical resection was not reported (Table 3). Adjuvant therapy was administered to 15 patients (20%); 9 received chemotherapy alone, 2 loco-regional radiotherapy on scrotal and homolateral inguinal areas and 4 received both treatments. Chemotherapy was platinum-based in the majority of cases.
Overall median survival of the 74 patients was 26.2 months (95% CI 22.1–52.1), Figure 1); 3 yr, 5 yr and 10 yr survival rates were 49%, 30% and 18%, respectively.
Table 4 shows survival in prespecified patient groups. Patients aged 65 years or older had strongly worse survival (Figure 2, Age classes). The presence of distant metastasis at diagnosis was associated with increased mortality (Figure 2, Histology). No important differences in survival were observed according to histological subtype (Figure 2, Presence of metastasis at diagnosis). Patients receiving adjuvant therapy had more than twofold increased risk of death (median survival 18.3 months vs. 41.9 months), (Figure 2, Treatment group).
4. Discussion
Our study confirmed the extreme rarity of MTVT, with 104 cases registered on a national basis in a 28-year span. Similarly to other more common sites of mesothelioma [20], MTVT was a disease of the elderly, with a median age of 72 years at diagnosis. Most patients had epithelioid histology, and in the majority of cases, a history of occupational asbestos exposure was reported. Surgery was the mainstay of treatment in all cases, with only a minority of patients receiving adjuvant chemotherapy and/or radiotherapy, with no improvement in outcome. Age older than 65 years, presence of distant metastasis at diagnosis and administration of adjuvant therapy were negative prognostic factors.
One of the major difficulties in managing MTVT is the lack of an accurate preoperative diagnosis. In accordance with previously published data [2,3,4], histological diagnosis in our cases was mostly achieved during or after primary surgery. Clinical presentation was consistent with previous series or reviews, with scrotal or testicular swelling and the presence of a hydrocele, often with local inflammation [2,3,4,9,10]. Notably, the rapid growth or recurrence of a hydrocele (particularly when hemorrhagic) and the presence of a scrotal/testicular mass should be suspicious for the diagnosis of MTVT, and should prompt imaging with ultrasonography and abdominal CT scan. In these cases, serum tumor markers can help in ruling out germ cell testicular cancer [21].
Surgery is the mainstay of treatment of MTVT [11,12]. In our series, all patients underwent intervention with the aim of macroscopic removal of the tumor. Most patients were treated with major surgery comprising orchi-funicolectomy, with hemiscrotectomy and/or inguinal lymphadenectomy in a minority of cases. Although it is difficult, based on literature data, to establish the optimal extent of surgery and, in particular, the benefit of adding hemiscrotectomy and lymphadenectomy of inguinal or even retroperitoneal nodes [4,22], it seems reasonable to achieve the maximum possible cytoreduction with surgery. For men with an incidental diagnosis of MTVT during hydrocelectomy, a timely completion of a hemiscrotectomy with en bloc orchi-funicolectomy is recommended, due to potential tumor seeding [4].
Adjuvant treatments after surgery were administered in a minority of patients (15 of 74, 20%), with heterogeneous regimens, which mainly comprised platinum-based chemotherapy, postoperative radiotherapy or both. The delivery of post-operative treatments was detrimental for survival, indicating confounding by indication (adjuvant treatments performed in patients with larger tumors with higher risk of recurrence) [23]. Similarly, in a review of 289 published cases of MTVT, 49 patients (17%) only received adjuvant therapy, with no improvement in survival as compared to patients treated with surgery alone; median survival was 24 months in both groups [2]. Due to the limited number of cases receiving post-operative treatments, and the lack of prospective or randomized data, the role of a multimodality approach in MTVT remains undefined.
Age older than 65 years and stage were negative prognostic factors. Similar results were reported in large case reviews [3]. Unexpectedly, metastases were detected in 14% of patients, with lung as the most frequent site, suggesting a mainly hematogenous pattern of disease spread.
Epithelioid histology was the most commonly found variety, similarly to what was reported in all major published series [2,3,4]. However, the favorable prognostic role of epithelioid subtype [2,24] was not confirmed in our series, likely due to the small number of non-epithelioid tumors, particularly of the sarcomatoid variant. The immunohistochemical profile of MTVT is similar to that of pleural mesothelioma, including markers such as calretinin, cytokeratin 5/6 and WT-1 [25]. MTVT exhibits a mutational profile similar to that of the pleura and peritoneum; however, alterations in CDKN2A and BAP1 (BRCA1-associated protein 1) are less common. Therefore, BAP1 and MTAP (methylthioadenosine phosphorylase) expression may be lost [26], but their sensitivities in MTVT appear to be lower. Histologic features, including architectural patterns and nuclear grade, have prognostic significance in pleural mesothelioma, although their correlation with genetic alterations has not been well studied yet [27]. Data on this correlation are lacking in MTVT, however the integration of molecular markers with histological features has the potential to improve its diagnosis and therapeutic management.
Finally, MTVT should be differentiated from exceedingly rare entities such as mesothelioma of uncertain malignant potential (MUMP) and well-differentiated papillary mesothelial tumor (WDPMT) of the tunica vaginalis testis, which are characterized by a benign course if completely resected [28].
5. Conclusions
In summary, to our knowledge, this is the largest population-based study on MTVT, including clinical details on diagnosis and treatment. It has the strength of a national surveillance evaluation of a very rare cancer, with strict inclusion criteria (cases were included only after review of all medical records, including imaging and cyto-histological data), and with thorough assessment of asbestos exposure made by experienced personnel using a standardized structured questionnaire. On the other hand, the study has the limitation of sometimes incomplete clinical data and of the lack of specific data quality evaluation. In particular, the registry does not routinely collect data on clinical presentation, tumor size, T-stage (including metastasis at presentation) or extent of surgical resection, which are risk factors for mortality. This information is almost complete for the regions in Northern Italy, in which most patients (72 out of 104) were residents. Therefore, although there is the potential for selection bias, we think our findings are fairly representative of clinical management of MTVT in our country.
Data provided by dedicated cancer registries remain essential, but their quality has to improve, especially on clinical presentation and therapeutic information that needs to be collected routinely. The integration of population-based registries with clinical national and international networks [16,17,18,27] and the implementation of prospective observational studies with detailed clinical and treatment information will offer the opportunity to improve knowledge, centralization of treatment, clinician expertise and, ultimately, the quality of patient management.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Straif K. Benbrahim-Tallaa L. Baan R. Grosse Y. Secretan B. El Ghissassi F. Bouvard V. Guha N. Freeman C. Galichet L. WHO International Agency for Research on Cancer Monograph Working Group. A review of human carcinogens—Part C: Metals, arsenic, dusts, and fibres Lancet Oncol.20091045345410.1016/S 1470-2045(09)70134-219418618 · doi ↗ · pubmed ↗
- 2Stella S. Ceresoli G.L. Dallari B. Barile R. Maisenti F. Rugarli S. Marinaccio A. Consonni D. Mensi C. Mesothelioma of the Tunica Vaginalis Testis: Diagnostic and Therapeutic Management. A Comprehensive Review, 1982–2024 Cancers 202416395610.3390/cancers 1623395639682143 PMC 11639812 · doi ↗ · pubmed ↗
- 3Plas E. Riedl C.R. Pflüger H. Malignant mesothelioma of the tunica vaginalis testis: Review of the literature and assessment of prognostic parameters Cancer 1998832437244610.1002/(SICI)1097-0142(19981215)83:12<2437::AID-CNCR 6>3.0.CO;2-G 9874447 · doi ↗ · pubmed ↗
- 4Grogg J.B. Fronzaroli J.N. Oliveira P. Bode P.-K. Lorch A. Issa A. Beyer J. Eberli D. Sangar V. Hermanns T. Clinicopathological characteristics and outcomes in men with mesothelioma of the tunica vaginalis testis: Analysis of published case-series data J. Cancer Res. Clin. Oncol.20211472671267910.1007/s 00432-021-03533-633559739 PMC 8310841 · doi ↗ · pubmed ↗
- 5Cai Y. Xu C. Lin J. Wang Q. Wang W. Guo Z. Song Z. Li Z. Liu A. Yu J. Expert Consensus on the Diagnosis and Treatment of Malignant Mesothelioma of the Tunica Vaginalis Testisi Meta Med 20251 e 7000310.1002/imm 3.70003 · doi ↗
- 6Nazemi A. Nassiri N. Pearce S. Daneshmand S. Testicular Mesothelioma: An Analysis of Epidemiology; Patient Outcomes; and Prognostic Factors Urology 201912614014410.1016/j.urology.2019.01.00930668959 · doi ↗ · pubmed ↗
- 7Marinaccio A. Consonni D. Mensi C. Mirabelli D. Migliore E. Magnani C. Di Marzio D. Gennaro V. Mazzoleni G. Girardi P. Association between asbestos exposure and pericardial and tunica vaginalis testis malignant mesothelioma: A case-control study and epidemiological remarks Scand. J. Work Environ. Health 20204660961710.5271/sjweh.389532253443 PMC 7737812 · doi ↗ · pubmed ↗
- 8Dytor T.B. Verril C. Alizadeh Y. Malignant mesothelioma of the tunica vaginalis and epididymis Diagn. Histopathol.20232925525810.1016/j.mpdhp.2023.02.003 · doi ↗