“Are You Just Looking to ‘Survive’?”: A Qualitative Study of Importance of Oncology Endpoints Beyond Overall Survival in Early-Stage Cancer
Shelagh M. Szabo, Sarah Walker, Evelyn Griffin, Aya McMillan, Robert Bick, Frances Simbulan, Eon Ting, Stephanie Snow

TL;DR
This study shows that cancer patients value outcomes like being free of cancer recurrence and returning to normal life, not just living longer.
Contribution
It demonstrates patient perspectives on non-survival endpoints in oncology trials and supports their use for faster treatment access.
Findings
Patients value non-survival endpoints like recurrence-free survival as meaningful outcomes.
Participants emphasized timely and equitable access to new treatments based on non-survival endpoints.
Importance of endpoints varied by cancer type, prognosis, and life stage.
Abstract
This study explored how people treated for early-stage or curable cancer in Canada view outcomes measured in clinical trials. Traditionally, trials focus on overall survival (how long people live), but newer studies often use other outcomes, such as being free of cancer returning (recurrence-free survival), staying free from signs that the cancer is worsening (event-free survival), or showing no cancer after treatment (pathological complete response). Thirty-three people treated for breast, lung, or gastrointestinal cancers were interviewed. Participants said living longer was important, but they also valued outcomes that reflect living without cancer and being able to return to normal life. Many emphasized the importance of timely and fair access to new treatments, even when results are based on these non-survival outcomes. Overall, the study shows that patients see these measures as…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
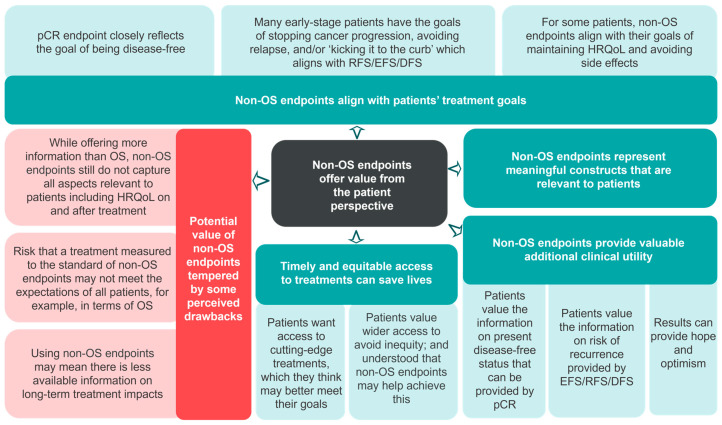 Figure 1
Figure 1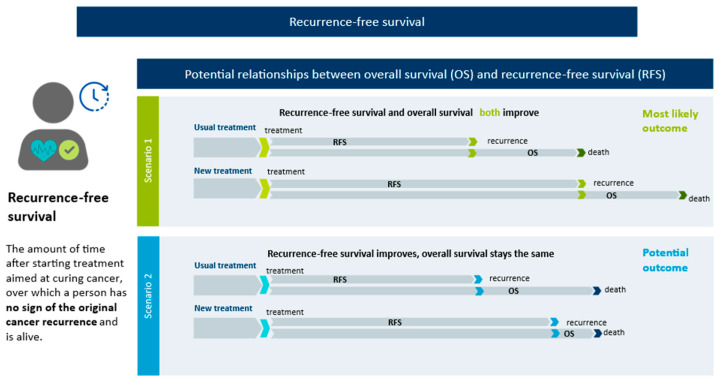 Figure 2
Figure 2- —AstraZeneca Canada
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBRCA gene mutations in cancer · Global Cancer Incidence and Screening · Cancer survivorship and care
1. Introduction
Despite advancements in screening, diagnosis, and treatments, which have substantially improved survival, cancer remains a leading cause of death worldwide [1]. For individuals with early-stage cancer, treatments vary based on stage and type, biomarker status, and clinical factors [2]. The treatment landscape for early-stage disease across most cancer types has been rapidly evolving, with increasing evidence supporting the use of neoadjuvant and/or adjuvant treatments to reduce the risk of recurrence, thereby improving long-term survival [3,4,5,6,7].
New treatments in oncology have traditionally been evaluated by improvements in overall survival (OS), “the time from randomization until death from any cause”, providing a standardized measure of efficacy for comparison across trials [8]. As an outcome measure, OS is understood by clinicians and patients, and accepted by regulatory and health technology assessment (HTA) decision-makers. However, many trials employing OS have been conducted in advanced, metastatic settings where OS may be observed over a shorter trial period, and there may be substantial challenges with assessing OS as the primary outcome, which has been garnering increasing attention [8,9,10]. For example, in early-stage cancer trials, patients are often treated with curative intent, and observing OS over many years can be infeasible. Estimates of OS in early-stage cancer may be confounded by the efficacy of subsequent treatments, the risk of relapses or progression, and other comorbidities [11]. Relying on OS data for regulatory and reimbursement approval could delay access to effective and potentially lifesaving therapies [8,9,10]. Further, in both early- and advanced-stage cancers, there is an increased recognition of the inherent value of aspects not directly measured by OS, especially from the perspective of patients and their caregivers. These include impact on health-related quality of life (HRQoL), short- and long-term treatment-related adverse effects, and level of physical functioning, knowledge of which would require assessment of alternative endpoints [11,12,13].
Due to the limitations of relying solely on OS data for establishing therapeutic benefit [10], endpoints assessed at earlier time points are being considered for decision-making [8,10,14]. These ‘non-OS’ endpoints—which include pathologic complete response (pCR), recurrence-free survival (RFS), disease-free survival (DFS) or event-free survival (EFS)—enable timely measures of treatment efficacy in advance of mature OS data [8,13,14,15]. While there is some recognition of the value of non-OS endpoints for some tumor types [8,16], non-OS endpoints are not yet widely accepted by HTA bodies for quantifying treatment value. This reflects the reality HTA bodies and payers face regarding the ‘OS impasse’ and how to weigh potential benefits of new therapies against financial considerations and established value metrics [10,17]. Given the rapid advancements in new treatments for early-stage cancers, it is also important to understand the perspectives of people with cancer on the value of non-OS endpoints, as endpoints used in clinical trials should be patient-relevant and meaningful [18]. Previous quantitative research found that cancer patients consider pCR, DFS and OS as distinct and relevant endpoints [19]. Qualitative assessments of non-OS endpoints, which can be useful to understand the context and significance patients attach to these [20], are limited [21]. An understanding of the perceived value and limitations of these endpoints from a patient perspective is important in order to ensure that assessments of the value of new cancer therapies reflect the priorities of patients and their families [22]. The objective of this study was to explore the perspectives of Canadians with early-stage cancer on the perceived value of non-OS endpoints.
2. Materials and Methods
2.1. Study Design
In this cross-sectional study, we recruited Canadian residents aged > 18 years who were currently receiving treatment or were previously treated with curative intent for the following cancer types and stages: stage I-IIIC breast cancer, I-IIIC non-small-cell lung cancer, limited-stage small-cell lung cancer, or gastrointestinal (GI) cancer (stage I-IIIB esophageal, I-IIIC gastric, or stage 0/A/B liver cancer). These stages were selected according to each type of cancer to represent cancer of early stage or treatable with curative intent and were intentionally selected to include stages beyond stage 1 cancer. Participants were deemed ineligible if they did not speak fluent English, were not able to provide informed consent, or were diagnosed with other GI cancers outside of those listed previously (e.g., colorectal cancer).
2.2. Sample Size and Recruitment Criteria
The target sample size was 30–35 participants to allow diversity in cancer type, stage, and treatments received (relevant to treatment with curative intent or for individuals considered to have early-stage cancer). The sample size was informed by published guidelines for achieving information saturation in qualitative interviews and prior study design [21,23,24,25,26]. We purposively aimed to recruit 10–12 individuals diagnosed with breast cancer, 10–12 with lung cancer, and 5–10 with GI cancer from across Canada.
2.3. Participant Recruitment
Participants were recruited through CanCertainty, a coalition of Canadian cancer patient groups, charities, and caregiver organizations that work with cancer care professionals to improve the affordability and accessibility of cancer treatment. Recruitment invitations were sent to the CanCertainty network through distribution lists. For harder to recruit segments (e.g., those with GI cancer), recruitment was ultimately supplemented via the patient databases of a recruitment partner, Global Perspectives.
Potential participants were provided with details of the study objectives and protocol. During screening, participants’ cancer type and stage were ascertained; no relationship between participants and interviewers existed prior to the interview.
2.4. Data Collection
Semi-structured interview guides were developed in collaboration with a medical oncologist (SS) and a patient expert partner with experience with breast cancer (AM). Endpoint definitions were developed from the published literature [8,13,14,15,27,28,29], adapted for a lay audience, illustrated with explanatory graphics (Appendix A; Figure A1), and validated by our clinical and patient expert collaborators. All study materials were pilot tested with three members of the general population and our patient collaborator.
At the beginning of the one-on-one virtual interviews, the explanatory graphics were shared on screen. Interviewers used these graphics to explain the clinical endpoints being discussed, allowing time to ask questions and clarify understanding before proceeding. Participants then discussed their treatment and provided perspectives on OS and non-OS endpoints; including how well endpoints aligned with their treatment priorities, and their thoughts on the implications of evaluating a new therapy based on non-OS endpoints. Participant clinical history and demographics were also collected. Interviews were conducted by three researchers (SMS, EG and SW) with qualitative training. To the best of our knowledge, no one was present aside from the interviewer and participant at each interview. Key points within the interview were summarized by the interviewer throughout the interview; further member checking was not performed [30].
As interviews progressed, materials were iteratively updated based on participant feedback, and interviewers met regularly to discuss any challenges and promote consistency. Incoming data were regularly reviewed, and recruitment continued until saturation was judged to be reached. This was defined as no new strengths or drawbacks to non-OS endpoints identified after five consecutive interviews. Interviews lasted approximately one hour and were audio-recorded. Informed consent was obtained from all subjects involved in the study. All participants received remuneration.
2.5. Analyses
Interviews were transcribed; transcripts were independently reviewed by two analysts for data familiarization. Reflexive thematic analysis was used to explore patterns in responses [31]. Codes were assigned to describe treatment experiences, views on endpoints, and alignment of endpoints with treatment goals, priorities, and preferences. Coding was iterative, with continuous addition of new codes and refinement of existing codes. Codes were grouped into categories that formed the basis for constructed themes. Supportive quotations were identified from transcripts, and themes were visualized using a thematic map representing the underlying coding tree.
The qualitative analysis was conducted by two researchers (SMS and SW), collaborating with the broader team for theme development. The analysis was performed iteratively alongside rounds of data collection to help identify topics requiring further investigation and whether further recruitment was necessary.
The clinical and sociodemographic characteristics of the sample were summarized.
Coding for reflexive thematic analysis was performed using NVivo 14 (Lumivero, Denver, CO, USA), and Microsoft Excel (Microsoft Corporation, Redmond, WA, USA) was used to tabulate quotations and quantitative analyses.
2.6. Reflexivity and Ethics
We acknowledge that our own likely treatment goals if confronted with cancer could have influenced our interpretations of participant statements. Conversely, given that we largely do not have personal cancer experience, there may be perspectives overlooked. This gap in personal insight was addressed by including a patient partner and an oncologist on the study team. As many of the research team work in health economics, our understanding of how clinical trial data are used by decision-makers may have resulted in us over-interpreting the words of participants, attributing to them a depth of understanding that would be unlikely for someone with lesser familiarity.
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2013. Ethical approval was obtained from the WCG IRB in January 2025 (file number: 1370874), and study reporting guided by the COREQ (COnsolidated criteria for REporting Qualitative research) checklist (Appendix B).
3. Results
3.1. Demographics and Clinical Characteristics
Of thirty-three participants, twelve reported a diagnosis of breast cancer, eleven of lung cancer, and ten of GI cancer; mean age was 54.8 (standard deviation = 12.9) years, and twenty-one were female (Table 1). No individuals withdrew after providing consent. Eleven participants were receiving treatment at the time of the interview, including five with recurrence. Twenty-eight participants had undergone surgery, twenty-six received chemotherapy, and twenty-one were treated with both (ten specified neo-adjuvant and nine adjuvant). Eighteen participants had no evidence of disease at the interview (Table 1).
3.2. Participant Perspectives on OS as a Trial Endpoint
All participants highly valued survival, noting several strengths to using OS as an endpoint (Table 2). They found the concept of OS easy to understand, and acknowledged it provides a benchmark for understanding how different therapies perform. They often regarded survival as a principal goal of treatment:
“It helps you plan for the rest of your life. If somebody says to you, ‘You have one year to be alive’ or ‘You have 10 years to be alive’ I think you would behave differently. You would pack these 10 years in one year…[OS] has some importance for the quality of life and what you want to achieve in your life”—ID11
However, participants also noted that OS alone does not capture all relevant aspects of their experiences. Other noted limitations included length of time needed to measure OS; that OS estimates can be misleading in early-stage cancers because of the inability to account for competing mortality risks; and that details of prognosis based on population averages may have limited personal relevance. Many participants expressed that OS does not explicitly consider HRQoL, focusing instead on length, and noted survival without good HRQoL was not desirable by most.
“It’s a funny word, ‘survival,’ because that … captures the essence of everything you’re asking, really. Are you just looking to ‘survive’? Are you looking to really lead a completely normal and healthy life going forward, and where is the gap between those two things?”—ID26
3.3. Participant Perspectives on Non-OS Endpoints
Participants felt non-OS endpoints offered value (Figure 1; Table 3), as they reflect their treatment goals and priorities. These included maintaining HRQoL and avoiding side effects; getting back to ‘normal’ after treatment by being disease-free; stopping cancer progression; and avoiding relapse over a longer term. Participants believed the information conveyed by non-OS endpoints provided additional clinical details beyond survival, and that knowledge of being cancer-free provides hope. As such, they felt clinical benefits demonstrated by early endpoints are sufficiently compelling to want access to new treatments (Table 4).
Participants placed high value on timely and equitable access to treatments, feeling this imperative to saving lives (Figure 1; Table 3). They equated having more treatment options with having better options, and desired access to cutting-edge treatments that better meet treatment goals (Table 4). Participants understood that treatments for early-stage cancer would take longer to be approved if OS was the primary endpoint, which would result in delayed access, and they expressed concerns that inequitable access could arise if treatments were available in certain places but not others:
“I can’t imagine them waiting for overall survival to put something on the market. Then I find it amazing how many people are saying ‘‘Well, the drug is available in the States, but it’s not available here yet,’ or…It’s not covered by our insurance yet, but it’s covered by so-and-so’s insurance.’… I don’t think they can wait for [OS]. They just have to do it. You have to save as many of us as possible.”–ID22
However, participants did identify some drawbacks to the use of non-OS endpoints (Figure 1; Table 3). Some noted that treatments measured to the standards of non-OS endpoints may not meet the expectations of all patients, and they still felt these endpoints did not capture all relevant aspects to decision-making. Finally, there was some concern that use of non-OS endpoints may compromise research transparency, and there would be less available information on long-term clinical benefits and side effects of the new treatment.
3.4. Valuing Specific Non-OS Endpoints Differently
Participants did not obviously distinguish between RFS, DFS, and EFS in terms of importance (Table 4). When asked about RFS or DFS, participants articulated the value of knowing disease status or the potential for a recurrence or new cancer to occur. However, EFS was more difficult for participants to conceptualize given the varied outcomes that the definition could encompass.
Participants generally agreed that achieving pCR was a priority in their own treatment journey, providing important information conveying hope for future treatment success, or peace of mind if they had no evidence of disease. For some (e.g., those undergoing mastectomy or lobectomy for lung cancer), having pCR identified on their surgical pathology was a principal goal. These individuals valued pCR as reassurance towards being disease-free in the short term rather than focusing on longer-term survival. Participants believed that achieving pCR would lead to extended RFS, DFS or EFS, and that clinical benefits in these endpoints would result in longer OS—even when informed that evidence for these associations is presently limited. The sense of hope and reassurance associated with achieving pCR or prolonged DFS or RFS appears to be an important part of how participants valued non-OS endpoints. Nonetheless, participants found pCR as an endpoint within a clinical trial context more difficult to conceptualize. As a result, the cohort predominantly favored medium- to long-term outcomes such as maintaining HRQoL and remaining cancer-free that are reflected in endpoints like RFS, DFS and EFS.
“[Being] recurrence-free would be more aligned with what I would want, because obviously the goal would be not to have to go through chemo, radiation, [and] surgeries again. So, of course, overall survival is important, but if I’m living but I’m living with other cancer and going through treatment, that wouldn’t be the goal.”—ID05
3.5. Other Factors Influencing Perspectives of Importance of Endpoints
Across tumor types, the relative importance of being disease- or recurrence-free versus maximizing length of life differed based on age, recurrence status, prognosis, life stage, and treatment history (Table 4).
Specific to age, younger participants and/or those with better prognoses—which included many with breast or liver cancer—typically valued having more and better treatment options. Many exercised choice in their treatment, often selecting options ensuring physical tumor removal. These individuals often expressed that their main goal was to be disease-free, and a corresponding preference for non-OS endpoints.
“I was hoping to be cured, of course. That was my main goal. If not, something that would extend my life for another few years. The other one, of course, was to be able to continue on with my life and return to work and spend time with my family.”—ID14
In contrast, those diagnosed at older ages, who had relapsed or continued to have evidence of disease (including many participants with lung or non-liver GI cancer) often described changing perspectives since diagnosis. For these participants, survival was important but being cured may not still be an option. This reinforces the importance of considering treatment impact beyond OS as maintaining HRQoL in the need for potentially longstanding cancer management became a more important personal treatment goal. As many of these individuals had progressed through multiple therapies and were worried about exhausting treatment options, they placed high importance on therapeutic innovation. As highlighted by a participant for whom the only option after surgery was a clinical trial, many would try almost anything to achieve the best possible outcome:
“After my surgery, when the clinical trial was offered, I was told that the immunotherapy drug had not been tried on my type of cancer. So, I was the first one to get it. Throwing something at the wall and seeing if it would stick. But it was all that was being offered … so I jumped at it.”—ID36
3.6. Patient Agency and Decision-Making at an Individual and Population Level
Some participants desiring a more active role in decision-making noted they do not always feel empowered to advocate for their own treatment goals, particularly when these differ from those of their care teams or emphasize outcomes other than survival. These participants expressed their desire for clinicians to consider the needs of patients as individuals when providing information to guide treatment decision-making. Some felt they had received insufficient information on the risk of recurrence or HRQoL impact when starting therapy—information that may have been conveyed by data on RFS, DFS or EFS—that resulted in them making a treatment decision they might not have had they had more information (Table 4).
Participants expressed a desire for decision-makers to consider access to treatments for early-stage cancers based on non-OS endpoints. Many, but not all, participants would value the opportunity to consider treatments with efficacy expressed in non-OS endpoints, even in the absence of OS data. Conversely, participants recognized the need to balance considerations around treatment novelty and shorter-term evidence of efficacy, with considerations around costs, side effects, and the lack of proven long-term survival benefit associated with non-OS endpoints. Even among those who felt non-OS endpoints strongly aligned with their treatment values, they remained concerned about side effects that “could be worse than the disease” or could negatively impact their lifestyle.
Finally, participants were encouraged by timely scientific research, particularly in situations where they felt existing treatment options were insufficient. Many expressed interest in joining clinical trials if it meant they could receive cutting-edge care without waiting for a lengthy drug-approval process. Particularly for those who had a recurrence, never attained ‘no evidence of disease’, or had run out of treatment options, they saw scientific innovation as a direct path to survival. Nonetheless, participants had different perspectives on how innovative research should intersect with their own treatment options. Novel treatments were not necessarily ‘right’ for all individuals, but even those not personally interested in innovative treatments felt that patients should have the opportunity to consider them, should the results for clinical benefits align with their treatment goals.
“It’s really encouraging to know that alternative endpoints are being considered that can provide patients with greater options for therapy … Whether it’s a complete response or a cure or just maintaining quality of life, all of those things are important. … My guess is that in talking to cancer patients, you will be hearing a lot of the same feedback, that people are willing to take those risks because the alternative is worse, and that if people are willing to try that with the guidance of their medical teams, those options should be available.”—ID02
4. Discussion
The treatment landscape for early-stage cancers continues to advance, and strategies to support the timely evaluation of treatment benefits, including considering endpoints beyond OS, are needed [10]. In addition to needing buy-in from decision-makers on these endpoints, they also should be patient-relevant and meaningful, ensuring that outcomes measured in clinical trials matter to patients and their families [33]. Our research highlights that, from the perspective of Canadians with early-stage cancer, non-OS endpoints like RFS, DFS or EFS are personally meaningful and highly related to their treatment priorities. These findings extend on a previous qualitative study reporting that lung cancer survivors found DFS to be intrinsically meaningful to treatment outcomes and aligned with patient goals, believing that longer DFS would help maintain better HRQoL [21]. Another study reported that liver cancer patients noted that OS does not take into account HRQoL, which they highlighted is an important concept when discussing the life expectancy of patients with cancer [34]. While these sentiments were echoed by our study participants, we also noted a moderating effect of age and life stage across cancer types; potentially due to the larger sample size and diversity of patient experiences within our sample.
The study findings also complement those of a discrete choice experiment (DCE) by Batchelder et al., reporting that early-stage breast cancer patients had the highest preference for pCR, followed by OS and DFS [35]. Another mixed-methods study reported that pCR was a patient-relevant outcome for neoadjuvant therapy in breast cancer, valued more highly than OS or DFS [19]. Those authors theorized that the importance placed on pCR could be due to participants’ assuming their response to therapy would translate to the destruction of circulating cells and result in them achieving a cancer-free status [19]. Participants in our study also valued the hope that attaining pCR could provide. However, they also considered this hope to be a benefit provided by RFS, DFS, and EFS as well; using language such as ‘getting back to normal’ and ‘kick [ing] it to the curb’ to relate the importance of knowing they were disease-free. Overall, our qualitative findings provide a deeper understanding of the reasons that people prefer different non-OS endpoints, and in which situations. For example, while participants found pCR relevant to their own personal experience, when considering the clinical utility of the non-OS endpoints, they valued RFS, DFS and EFS for the longer-term information on HRQoL and recurrence they believed these endpoints provide.
Batchelder et al. also noted that endpoint importance differed according to age and that breast cancer patients with more recent diagnoses placed more relative importance on pCR vs. those with longer times since diagnosis valuing OS [35]. We also identified variability in age, prognosis, and treatment status impacts the perceived importance of being cancer-free. Taken together with the present study, these findings underscore the importance of patient characteristics when considering which endpoints are most relevant.
Achieving personal treatment goals is not the only reason that participants valued non-OS endpoints—broader treatment access issues were also a priority. A recent US-based DCE reported that participants with cancer were willing to wait for a potential treatment with a survival benefit (vs. an existing treatment with low certainty of survival benefit); conversely, they also valued faster access to new treatments [36]. We also noted that participants valued the long-term safety and efficacy information that the OS endpoint can provide. Nonetheless, most participants were very concerned about timely access to innovative treatment, which they understood could be facilitated through using non-OS endpoints in decision-making [13]. These conflicting viewpoints may be partly explained by the subset of participants with lower tolerance of risk for novel treatments, but who nonetheless support their development and more widespread access.
Participants also highlighted their interest in the information conveyed by non-OS endpoints on HRQoL impact and risk of recurrence. A drawback to the current focus on OS to evaluate treatment efficacy is that it may make it challenging for patients to understand information provided on less familiar non-OS outcomes, and further education around non-OS endpoints will help ensure patients can make informed treatment decisions. This gap has been documented in a mixed-methods study that noted that, although information on clinical endpoints (OS, progression-free survival, response rate) was readily available online, endpoint definitions relied on technical language that may not be easily understood. In focus groups, few participants demonstrated a deep understanding of these concepts even after the endpoints were explained; for example, many assumed that all endpoints could indicate whether a cure was achieved or length of life extended [34]. These findings underscore the complexity of communicating clinical outcomes to patients and raise important considerations with how to balance patient desires for novel treatments with expectations for evidence-based decision-making that also considers economic value. Patient input pathways for HTA can help ensure rigorous patient-derived evidence informs decisions being made [37,38], and deliberative processes facilitating continued evaluation of evolving evidence, such as those proposed for precision oncology medicine, may also offer a path forward [39].
In this study, we focused specifically on patients with esophageal, gastric, and liver subtypes of GI cancer for two reasons. Firstly, compared to colorectal cancer, which has a substantial body of psychosocial literature, esophageal, gastric, and liver cancers remain under-represented in qualitative research [40,41,42]. Secondly, these cancers present unique clinical and experiential challenges in the curative setting, including complex multimodal treatments and uncertainties around long-term prognosis [42,43]. Similarly, we focused not only on patients with stage I (early stage cancer) but also those with later stage cancers who were treated with curative intent, to collectively explore the preferences and priorities of Canadians navigating treatment journeys most relevant to outcomes being documented using non-OS endpoints.
The robust qualitative methods used enabled a deep exploration of the perspectives driving patient preferences, complementing available quantitative preference data [44]. Additional strengths include the diversity of experience and perspectives offered by including participants with different cancer types and disease stages (among those treated with curative intent). While strata were set for key clinical characteristics, recruitment targets for characteristics such as province, cultural background, or educational attainment were not. As a result, this study has limited representation of ethnic minorities, lung cancer participants were mostly female despite a higher incidence in males, and approximately one-third held postgraduate degrees. This represents a limitation to generalizability as those with higher educational attainment may have different health literacy, access to care, or attitudes towards and awareness of the outcomes discussed. Although conducting research online may reduce barriers to participation, it may exclude those who are less comfortable with online technology [45]. Finally, disease status was self-reported and not corroborated clinically.
This study highlights several important directions for future work. First, understanding HTA body perspectives on this research and non-OS endpoints in general would be valuable as a next step to help ensure trials are measuring outcomes that are meaningful to patients while also providing the necessary data for understanding treatment value. Additionally, extending this research to incorporate the perspectives of lesser-represented or marginalized groups, and including people with a broader variety of cancers will help promote equity and ensure that patient-centered evidence is representative and inclusive.
5. Conclusions
This study used reflexive thematic analysis to explore the importance of cancer trial endpoints beyond OS for individuals treated for early-stage cancers or with curative intent, through the lens of their own treatment goals and priorities. Participants highlighted the value they perceived the non-OS endpoints to have due to their alignment with treatment goals, such as being ‘cured’, minimizing side effects, avoiding recurrence, and maintaining quality of life. Participants also valued the clinical details those endpoints convey. Participants were invested in access to novel treatments with meaningful improvements in HRQoL and non-OS endpoints, even in the absence of OS data. These findings provide evidence of the patient-perceived value of non-OS oncology endpoints to support decision-making, and highlight the impact of patient context and experiences on treatment goals and endpoint preferences.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Canadian Cancer Statistics Advisory Committee in collaboration with the Canadian Cancer Society, Statistics Canada and the Public Health Agency of Canada. Canadian Cancer Statistics 2021 Available online: https://cancer.ca/en/research/cancer-statistics/past-editions(accessed on 6 October 2025)
- 2Akbari M.E. Ghelichi-Ghojogh M. Nikeghbalian Z. Karami M. Akbari A. Hashemi M. Nooraei S. Ghiasi M. Fararouei M. Moradian F. Neoadjuvant VS adjuvant chemotherapy in patients with locally advanced breast cancer; a retrospective cohort study Ann. Med. Surg.20228410492110.1016/j.amsu.2022.104921 PMC 975837336536751 · doi ↗ · pubmed ↗
- 3Esteva F.J. Hubbard-Lucey V.M. Tang J. Pusztai L. Immunotherapy and targeted therapy combinations in metastatic breast cancer Lancet Oncol.201920 e 175e 18610.1016/S 1470-2045(19)30026-930842061 · doi ↗ · pubmed ↗
- 4Forde P.M. Spicer J. Lu S. Provencio M. Mitsudomi T. Awad M.M. Felip E. Broderick S.R. Brahmer J.R. Swanson S.J. Neoadjuvant Nivolumab plus Chemotherapy in Resectable Lung Cancer N. Engl. J. Med.20223861973198510.1056/NEJ Moa 220217035403841 PMC 9844511 · doi ↗ · pubmed ↗
- 5Wakelee H. Liberman M. Kato T. Tsuboi M. Lee S.H. Gao S. Chen K.N. Dooms C. Majem M. Eigendorff E. Perioperative Pembrolizumab for Early-Stage Non–Small-Cell Lung Cancer N. Engl. J. Med.202338949150310.1056/NEJ Moa 230298337272513 PMC 11074923 · doi ↗ · pubmed ↗
- 6Tang W.F. Ye H.Y. Tang X. Su J.W. Xu K.M. Zhong W.Z. Liang Y. Adjuvant immunotherapy in early-stage resectable non–small cell lung cancer: A new milestone Front. Oncol.202313106318310.3389/fonc.2023.106318336776323 PMC 9909200 · doi ↗ · pubmed ↗
- 7Wu Y.-L. Tsuboi M. He J. John T. Grohe C. Majem M. Goldman J.W. Laktionov K. Kim S.-W. Kato T. Osimertinib in Resected EGFR-Mutated Non–Small-Cell Lung Cancer N. Engl. J. Med.20203831711172310.1056/NEJ Moa 202707132955177 · doi ↗ · pubmed ↗
- 8U.S. Food and Drug Administation Clinical Trial Endpoints for the Approval of Cancer Drugs and Biologics: Guidance for Industry U.S. Food and Drug Administation Silver Spring, MD, USA 2018