Effect of the Primary Nursing Model on Self-Care Skills of Hospitalized Older Patients with Multimorbidity: A Quasi-Experimental Study
Isabel Gonçalves, Sofia Almeida, Élvio Jesus, Elisabete Nunes

TL;DR
This study found that the primary nursing model improves self-care skills in older patients with multiple health conditions during and after hospitalization.
Contribution
The study provides empirical evidence that the primary nursing model enhances therapeutic self-care in multimorbid older patients.
Findings
The intervention group had lower initial self-care scores but showed greater improvement over time.
The primary nursing model significantly improved self-care skills compared to standard care.
Results suggest the model supports patient autonomy and better care continuity for complex cases.
Abstract
Background/Objective: The global increase in life expectancy has led to a higher prevalence of multimorbidity among older patients, often requiring frequent and complex healthcare. Enhancing self-care skills during hospitalization is a key priority in promoting patient autonomy and improving outcomes. The objective of the study was to analyze the effect of the primary nursing model on the therapeutic self-care of older patients with multimorbidity during hospitalization. Methods: It was a quasi-experimental study conducted in two comparable medical-surgical units of a private hospital in Portugal. The intervention unit adopted the primary nursing model, while the control unit maintained standard nursing care. A convenience sample of older patients with multimorbidity was recruited (n = 206; intervention group = 106, control group = 100). Therapeutic self-care was measured using the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
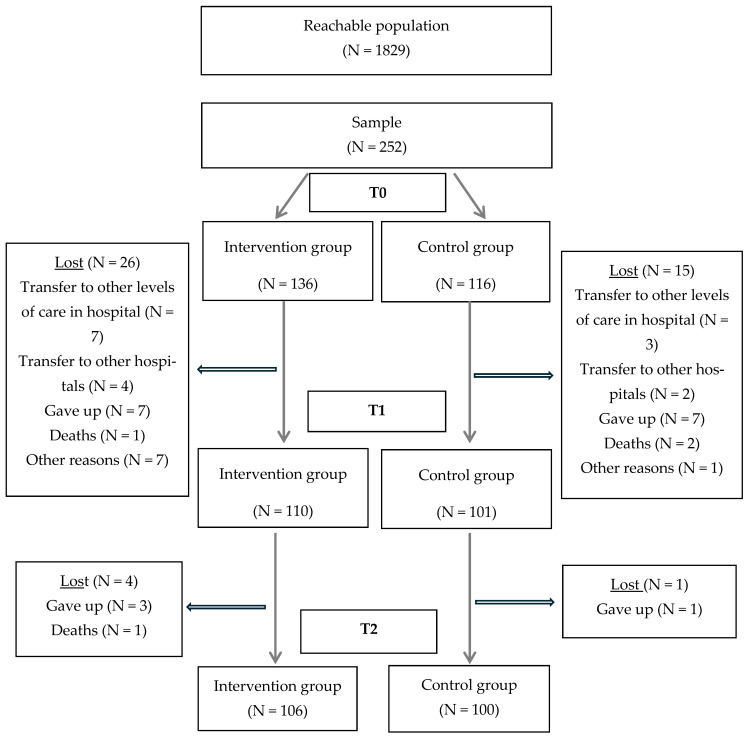 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsChronic Disease Management Strategies · Palliative Care and End-of-Life Issues · Family and Patient Care in Intensive Care Units
1. Introduction
Nurses play a pivotal role in contemporary healthcare systems, particularly amid rising demands caused by ageing populations, resource constraints, and the increasing burden of chronic and complex conditions [1]. Hospitalized patients with multimorbidity, defined as the coexistence of two or more chronic conditions [2] require comprehensive, coordinated care, making nurse-led care management models especially valuable.
Patient-centered care is central to modern nursing practice, with a strong emphasis on supporting self-care, preparing patients for discharge, and ensuring continuity of care [3]. Organizational models of nursing practice, defined as the structures and processes that guide nursing care delivery [4] can significantly influence patient outcomes, especially when designed to foster therapeutic relationships.
Historically, nursing care in hospitals has been delivered through various models, including functional nursing, team nursing, total patient care, and the -primary nurse model [5,6,7,8]. Among these, the primary nursing model stands out for promoting continuity, accountability, and patient-centered by assigning one nurse to be responsible for a patient’s care throughout their hospital stay [9]. Unlike individualized care, where different nurses assume responsibility on a shift-by-shift basis, primary nursing provides consistency and a therapeutic nurse–patient relationship [5].
Primary nursing is a patient-centered care model based on the relationship between nurse and patient [10]. The primary nurse is responsible for ensuring that decision-making is patient-centered, establishing the care plan and strategies for implementing it, and providing direct interpersonal communication with other members of the multidisciplinary team [10]. The coordination of the care plan is always of the primary nurse. They assume the patient’s care when on shift. They delegate it to other members of their team when absent.
To assess the effectiveness of such models, it is essential to identify outcomes that are sensitive to nursing interventions. Therapeutic self-care skills have been widely recognized as one such outcome, reflecting a patient’s ability to manage treatment, symptoms, and lifestyle adjustments independently [11,12].
With global life expectancy rising and the proportion of older patients increasing, hospitals are challenged by higher patient complexity, shorter lengths of stay, high readmission rates, and workforce constraints. Nurse managers must ensure safe, individualized, and outcome-focused care delivery [13,14]. In this context, the primary nursing model may serve as a viable strategy for enhancing care quality, especially for vulnerable populations such as older patients with multi-morbidity.
While previous studies have linked primary nursing to reduced adverse events, less is known about its potential to improve positive outcomes, such as enhanced self-care capabilities [15]. Implementing the primary nursing model appears to reduce infections related to venous catheters, pressure ulcers, falls, medication errors and urinary tract infections [16].
A systematic review analyzing studies that evaluated the impact of nursing care organization models in hospitals on patients’ health outcomes concluded that conclusive results could not be obtained due to the scarcity and lack of robustness of the studies [17].
Addressing this gap, the present study aimed to evaluate the effect of the primary nursing model on therapeutic self-care skills in hospitalized older patients with multimorbidity.
2. Materials and Methods
2.1. Design and Participants
This was a quasi-experimental, longitudinal study with a control group, conducted between April 2022 and August 2023 in two medical-surgical units of a private acute care hospital in Lisbon, Portugal. The hospital has 315 beds. The intervention unit received an organizational change in nursing care (implementation of the primary nursing model, see Table 1), while the control unit maintained the usual individualized care model. Both units had similar characteristics: the intervention unit had 34 beds and the control unit 35, and both admitted the same patient profiles. Each unit had a nursing team of 24 members. The study followed the Transparent Reporting of Evaluations with Nonrandomized Designs (TREND) guidelines [18]; see Table A1.
Participants were selected by convenience sampling. Inclusion criteria were as follows: (1) age ≥ 65 years (older patients); (2) diagnosis of at least two chronic conditions, one of which had to be cardiovascular disease, cancer, chronic obstructive pulmonary disease, or diabetes; (3) expected hospital stay > 48 h; and (4) cognitive ability to read, write, and understand the study information. Exclusion criteria included transfers to other units or levels of care within or outside the organization.
From 1829 eligible patients hospitalized in 2022 (980 in the intervention unit; 849 in the control), a total of 252 were recruited: 136 in the intervention group and 116 in the control group. The minimum required sample was 122 participants (61 per group), based on power analysis using G*Power 3.1, with an effect size of Cohen’s d = 0.66 [19], significance level of 0.05, and power of 0.95.
2.2. Intervention
The intervention was coordinated with the nurse director and head nurses. Primary nurses in the intervention unit were identified by the head nurse and invited to participate. Four training sessions on the primary nursing model were delivered by the principal investigator over four weeks (February–March 2022). Additional briefings occurred during shift handovers, supported by printed teaching materials. The model was implemented at the end of March 2022.
Patient recruitment began in both units in April 2022. Eligible patients were informed about the study and invited to participate. Those who consented signed a written informed consent form. In the intervention unit, patients were assigned to a primary nurse responsible for care throughout the hospital stay; in the control unit, care continued to be shift-based.
Objectives and Hypotheses
The general objective was to analyze the effect of the primary nursing model on the therapeutic self-care of older patients with multimorbidity during hospitalization.
Specific objectives:
To compare self-care scores between admission (T0) and discharge (T1).
To compare self-care scores between discharge (T1) and 30-day follow-up (T2).
To compare self-care scores between admission (T0) and follow-up (T2).
Hypotheses:
H1. There is a statistically significant difference in therapeutic self-care scores between groups at baseline (T0).
H2. The increase in self-care scores from T0 to T1 is greater in the intervention group.
H3. The increase in self-care scores from T1 to T2 is greater in the intervention group.
H4. The increase in self-care scores from T0 to T2 is greater in the intervention group.
2.3. Measures
Sociodemographic and clinical data were collected through a structured questionnaire and patient medical records. Variables included age, sex, education level, household and caregiver. Clinical data included reasons for hospitalization and the number and type of chronic conditions.
Therapeutic self-care (dependent variable) was assessed using the Therapeutic Self-Care Scale—European Portuguese version (TSCS-EP), validated by Cardoso et al. [20], with Cronbach’s alpha = 0.979. This instrument assesses the following areas of therapeutic self-care: management of the therapeutic regimen; ability to recognize symptoms or changes in health status, particularly those that may be indicative of complications; ability to perform normal activities; and ability to identify and implement strategies to adapt to the health condition. The scale consists of 12 items, with responses rated on a 6-point Likert scale ranging from 0 (“I don’t know/I can’t”) to 5 (“I know/I can”).
2.4. Data Collection
The principal investigator and unit head nurses collected data. Newly admitted, eligible patients were approached, informed, and consented. TSCS-EP assessments were completed at three time points: T0 (within 48 h of admission), T1 (on discharge), and T2 (30 days post-discharge, via telephone). Completed questionnaires were submitted in sealed envelopes with participant codes.
2.5. Data Analysis
Data were analyzed using SPSS^®^ version 28 for Windows (IBM, Chicago, IL, USA). Descriptive statistics were used for participant characterization. Categorical variables were presented as frequencies and percentages; continuous variables as means and standard deviations.
Levene’s test was used to test homogeneity of variances. Student’s t-test for independent samples compared group means. Chi-squared or Fisher’s exact tests were used for categorical comparisons [21]. Effect size was calculated using Cohen’s d [22].
An exploratory factor analysis (EFA) was performed to validate the psychometric properties of the TSCS-EP in the study sample, hereafter referred to as Therapeutic Self-Care Scale applied to People with Multimorbidity in Hospital (EATPPMH). The analysis followed standard criteria: KMO > 0.70, Bartlett’s test p < 0.001, Cronbach’s alpha > 0.70, communalities > 0.5, and factor loadings ≥ 0.4. Varimax rotation and eigenvalue > 1 were used. Correlations were interpreted as: low (0.2–0.39), moderate (0.4–0.69), high (0.7–0.89), and very high (0.9–1.0).
Multiple regression and logistic models were tested.
A significance level of 0.05 was adopted for all tests.
3. Results
A total of 252 participants were recruited at baseline: 136 in the intervention group and 116 in the control group. During hospitalization, 26 participants were lost in the intervention group and 15 in the control group. Between discharge and follow-up, an additional 4 participants were lost in the intervention group and 1 in the control group. In total, 106 patients in the intervention group and 100 in the control group completed the study, as illustrated in Figure 1.
Regarding participants’ sociodemographic characteristics, there were no statistically significant differences between the groups (p > 0.05). The mean age in both groups was approximately 75 years, and the majority were female. Most participants in the intervention group had primary education, while higher education was more frequent in the control group. In both groups, the majority lived with a spouse, who was also the primary caregiver. The average length of stay was two days longer in the intervention group than in the control group, and this difference was statistically significant (p = 0.020).
The reason for hospitalization showed a significant association with the distribution of participants between the two units (p < 0.001). Respiratory system diseases were the most frequent reason for admission in the intervention group, whereas musculoskeletal and connective tissue diseases, as well as skin and subcutaneous tissue diseases, were more common in the control group.
Most participants in both groups had two chronic diseases belonging to one of the selected study categories: cardiovascular disease, cancer, chronic obstructive pulmonary disease or diabetes. There was a significant association in the distribution of the number of chronic diseases between the groups (p = 0.002). Circulatory system diseases were the most prevalent chronic condition in both groups, and the majority of participants also presented other chronic conditions beyond those included in the study. Table 2 presents the sociodemographic and clinical characteristics of the participants.
3.1. Validation of the Psychometric Properties of the Therapeutic Self-Care Scale—Portuguese Version for People with Multimorbidity in Hospital (EATPPMH)
The EATPPMH was administered to the intervention group (N = 106) and the control group (N = 100). EFA was conducted to evaluate the psychometric properties of the scale at three points: admission, discharge, and follow-up, in both groups. The analysis used principal component analysis with varimax rotation.
No comparable factor structure was found across the groups and time points. The number of factors ranged from two to four, with a maximum explained variance of 75.5%. A three-factor solution was then forced for each time point to improve comparability, with the follow-up results showing the most stable solution and optimal variance explanation.
Kaiser-Meyer-Olkin values were 0.83 (intervention group) and 0.76 (control group), both considered good. Bartlett’s test of sphericity was significant in both groups (χ^2^(66) = 1415.81, intervention; χ^2^(66) = 873.49, control; p < 0.001), indicating appropriate correlations among items.
At follow-up, the three-factor model explained 81.7% of the variance in the intervention group and 72.5% in the control group:
- Factor 1—Recognizing and managing signs and symptoms (4 items): explained 60.7% (intervention) and 49.5% (control) of variance.
- Factor 2—Managing changes in health status (5 items): explained 13.7% (intervention) and 10.8% (control).
- Factor 3—Managing medication (3 items): explained 7.2% (intervention) and 12.3% (control).
Internal consistency was very high in the intervention group (Cronbach’s α = 0.934) and high in the control group (Cronbach’s α = 0.895).
3.2. Therapeutic Self-Care at Admission, Discharge, and Follow-Up
Therapeutic self-care was assessed at three points: admission (T0), discharge (T1), and 30-day follow-up (T2). The mean scores for overall self-care and for each component were compared between the intervention and control groups at each time point. The two groups were also compared in terms of the difference in self-care between the various assessment points in the study.
At admission, the intervention group presented a significantly lower mean score for overall therapeutic self-care and for the “Recognizing and managing signs and symptoms” component, compared to the control group. No statistically significant differences were observed for the remaining components. The Cohen’s d effect size is low for all components. Results are detailed in Table 3.
Differences in self-care over time are shown in Table 4. From admission to discharge (T1−T0), the intervention group showed a significantly greater increase in overall self-care (p = 0.024) and in the “Recognizing and managing signs and symptoms” component (p = 0.037) compared to the control group.
Between discharge and follow-up (T2−T1), no significant differences were observed between groups in overall self-care or in any component.
Between admission and follow-up (T2−T0), the intervention group showed a significantly greater improvement in overall self-care (p = 0.008), and in the components “Recognizing and managing signs and symptoms” (p = 0.033) and “Managing medication” (p = 0.014). No significant differences were observed for the “Managing changes in health status” component. The Cohen’s d effect size is low for all components.
4. Discussion
The main aim of this study was to analyze the effect of the primary nursing model on therapeutic self-care in hospitalized older patients with multimorbidity. The findings revealed that the mean self-care score at baseline (T0) was significantly higher in the control group. At discharge (T1), the intervention group demonstrated a greater and statistically significant improvement in self-care compared to the control group. Although no significant differences were observed between the groups at follow-up (T2) relative to discharge, the change from admission to follow-up showed a significantly greater improvement in self-care in the intervention group.
Multiple regression and logistic models were tested using the sociodemographic and clinical variables. However, none of these models demonstrated statistical adequacy or acceptable explanatory power. They explained little of the data and were therefore not presented or discussed.
Sociodemographic characteristics were relatively homogeneous between groups, with no significant differences, except for the length of hospital stay, which was significantly longer in the intervention group by an average of two days. This may be related to the characteristics of hospitalization, as there was a significant association between reason for admission and hospital unit. It should be noted that the longer average length of stay observed in the intervention group could indicate more interactions with nurses and more time for health education. This may have contributed to the more positive self-care results. Cumulatively, respiratory and circulatory system diseases accounted for 45.3% and 40.5% of hospitalizations, respectively. These findings align with previous studies, such as Zhang et al. [23], who identified circulatory diseases as prevalent chronic conditions in hospitalized older patients with multimorbidity. The intervention group had a higher prevalence of respiratory and circulatory diseases. They may have been more receptive to the health education interventions led by nurses, which could explain the improvements in self-care observed. The intervention group also had a higher proportion of patients with three or four chronic conditions. This could have created scope for enhancing self-care scores.
The presence of multiple chronic diseases has been associated with greater difficulty in understanding health information and a higher risk of loss of functional independence [23,24]. At admission, participants in the intervention group had significantly lower mean self-care scores, particularly in the component “recognizing and managing signs and symptoms.” This may be partially explained by a lower socioeconomic status in this group, including lower education levels and professional activity in working age, factors known to negatively impact the development of self-care abilities [25]. These individuals may also face more difficulties in accessing health services, navigating the healthcare system, or obtaining necessary resources [26]. These findings confirm Hypothesis 1 (H1): a statistically significant difference existed in baseline global self-care scores between groups. To address the first specific objective, self-care was assessed at discharge and compared to admission. The intervention group demonstrated a significantly greater improvement in self-care, particularly in the “recognizing and managing signs and symptoms” component, confirming Hypothesis 2 (H2). These findings are consistent with Faessler et al. [27], who reported that patients receiving nurse-led care demonstrated significantly greater improvements in self-care than those receiving usual care. It should be noted that the analysis did not adjust for baseline differences between groups. This might have influenced the observed outcomes.
For the second objective, self-care was assessed at one-month post-discharge. Although the intervention group maintained higher self-care scores, the differences compared to the control group were not statistically significant, and Hypothesis 3 (H3) was not confirmed. These findings highlight the importance of continuity of care in the community. A systematic review analyzed 30 studies on the integration of primary healthcare after hospital discharge. The studies, which involved older people being followed up by primary healthcare after discharge from hospital, were compared with those in which no such follow-up took place. It was found that people who received follow-up care had a 32% lower risk of being readmitted to hospital within 30 days, and a 17% lower risk within six months [28]. Interventions that include self-management support, telephone follow-up, and medication reconciliation are particularly effective in reducing readmission rates in older adults [29].
The third objective compared the change in self-care from admission to follow-up between groups. The intervention group showed significantly greater gains, confirming Hypothesis 4 (H4). Notably, improvements were observed across all components in the intervention group, with significant gains in “recognizing and managing signs and symptoms” and “managing medication.”
The dropout rate was higher in the intervention group than in the control group. This may be partly explained by the fact that participants in the intervention group had a higher disease burden and a lower level of education [24].
Overall, the primary nursing model appears to have had a positive effect on therapeutic self-care among older patients with multimorbidity during hospitalization. However, the sustainability of these gains -seems to require coordinated community-based support. Nurse-led care models have shown potential to improve medication adherence, reduce emergency department use, and prevent hospital readmissions in this population [30].
Recommendations and Limitations
For human resource and time reasons, participants were selected by convenience sampling rather than random sampling, which would allow for greater generalizability of the results, this is a limitation of the study.
No comparative analysis was performed between retained and lost participants, which may introduce bias and affect the generalizability of the findings.
Although multivariate models including sociodemographic, clinical, and hospitalization-related variables were tested, they did not demonstrate acceptable statistical adequacy or explanatory power. Consequently, adjusted analyses were not retained. As a result, baseline differences between groups (e.g., disease profiles, multimorbidity load, and length of stay) may have influenced the outcomes and confounded the observed effects.
In addition, it would be important to know the nurses’ opinions about the primary nursing model and its impact on nurse retention and satisfaction, which is a suggestion for future research.
5. Conclusions
The study suggests that the primary nursing model may be beneficial in improving self-care outcomes among older patients with multimorbidity during hospitalization. The components of self-care showing the greatest gains were recognizing and managing signs and symptoms and managing medication. However, these findings should be interpreted with caution because of baseline differences between groups, the loss of participants during the study, and the absence of adjusted analyses, which may have confounded the observed effects. Further studies using robust designs and appropriate adjustment for potential confounders are needed to confirm these results.
For any patient to be able to actively participate in the management of their health condition, they must have the skills to manage it effectively and efficiently. Nurses, by the nature of their interventions, whether through health education, empowerment or acquisition of self-care skills, are able to influence these patients’ health outcomes. At the same time, the nurse is a privileged interlocutor between the older patient’s with multimorbidity/family and the rest of the multiprofessional team.
Implementing this model may contribute to better health outcomes and reduced readmissions, emphasizing the nurse’s central role in empowering patients and coordinating multidisciplinary care.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Moulton J.E. Withanage N.N. Subasinghe A.K. Mazza D. Nurse-Led Service Delivery Models in Primary Care: A Scoping Review Protocol Nurse-Led Service Delivery Models in Primary Care: A Scoping Review Protocol BJGP Open 20226 BJGPO.2021.019410.3399/BJGPO.2021.019435292428 PMC 9680750 · doi ↗ · pubmed ↗
- 2Mercer S. Salisbury C. Fortin M. ABC of Multimorbidity Wiley BMJ Books John Wiley & Sons Hoboken, NJ, USA 2014
- 3Gonçalves M.I.R. Mendes D.A. Caldeira S. Jesus E. Nunes E. Nurse-Led Care Management Models for Patients with Multimorbidity in Hospital Settings: A Scoping Review J. Nurs. Manag.2022301960197310.1111/jonm.1362135403299 · doi ↗ · pubmed ↗
- 4Hoffart N. Woods C.Q. Elements of a Nursing Professional Practice Model J. Prof. Nurs.19961235436410.1016/S 8755-7223(96)80083-48979639 · doi ↗ · pubmed ↗
- 5Fairbrother G. Chiarella M. Braithwaite J. Models of Care Choices in Today’s Nursing Workplace: Where Does Team Nursing Sit?Aust. Health Rev.20153948949310.1071/AH 1409126143068 · doi ↗ · pubmed ↗
- 6Fawcett J. More Thoughts About Models of Nursing Practice Delivery Nurs. Sci. Q.20213445846110.1177/0894318421103158434538169 · doi ↗ · pubmed ↗
- 7Fawcett J. Thoughts About Models of Nursing Practice Delivery Nurs. Sci. Q.20213432833010.1177/0894318421101046034212806 · doi ↗ · pubmed ↗
- 8Parreira P. Santos-Costa P. Neri M. Marques A. Queirós P. Salgueiro-Oliveira A. Work Methods for Nursing Care Delivery Int. J. Environ. Res. Public Health 202118208810.3390/ijerph 1804208833669955 PMC 7924841 · doi ↗ · pubmed ↗