Navigating Therapies, Challenges, and Recommendations for Treatment-Resistant Peripartum Depression: A Comprehensive Review
Afshan Zeeshan Wasti, Sarah Almutairi, Mohsina Huq, Amal Hussain, Amal Mohamad Husein Mackawy, Farah Jabeen, Basmah Alharbi, Anjuman Gul Memon, Mawahib Ahmed

TL;DR
This review explores effective and safe treatments for peripartum depression that doesn't respond to standard therapies, focusing on both drugs and non-drug options.
Contribution
The paper provides a comprehensive review of treatment-resistant peripartum depression with a focus on balancing maternal and fetal safety.
Findings
Pharmacological treatments like SSRIs and zuranolone show efficacy but raise fetal safety concerns.
Non-pharmacological interventions such as CBT and rTMS offer safe and effective alternatives.
Personalized treatment plans and expanded mental health infrastructure are recommended for better TRPD care.
Abstract
Treatment-resistant peripartum depression (TRPD) is a significant public health concern due to the dual imperative of maternal symptom relief and fetal/neonatal safety with complex therapeutic challenges, particularly among expecting mothers worldwide. This comprehensive review focused on current pharmacological and non-pharmacological interventions for treatment-resistant depression (TRD)/peripartum depression (PPD), highlighting their mechanisms, efficacy, safety profiles, and practical considerations. The search strategy is based on PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analysis), using a systematic search of PubMed, Cochrane Library, and EMBASE for English-language articles published between 2000 and 2024, with a combination of Medical Subject Headings (MeSH) and free-text terms for TRD/TRPD. After screening, the initial search yielded 142 articles; only…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
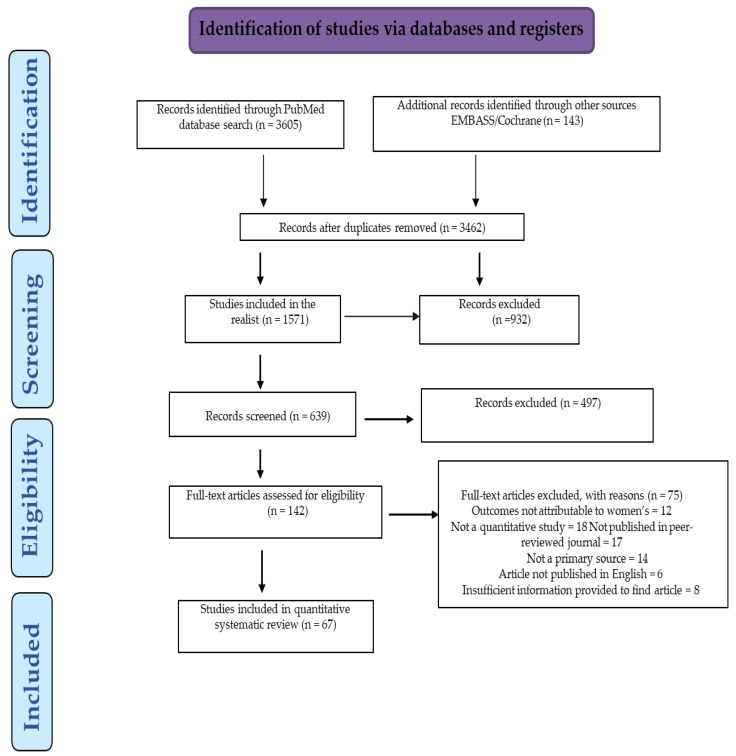 Figure 1
Figure 1| Category | Agent/Class | Mechanism of Action/Modality | Level of Evidence (TRD) | Level of Evidence (PPD) | Main Safety Warnings (Perinatal) | References |
|---|---|---|---|---|---|---|
| First-line Antidepressants | SSRIs (e.g., fluoxetine, sertraline) | Selective serotonin reuptake inhibition | Common first-line; often insufficient alone in TRD | Widely used; sertraline preferred in breastfeeding | Good safety profile; low infant exposure via breast milk | [ |
| SNRIs (e.g., venlafaxine, duloxetine) | Serotonin and norepinephrine reuptake inhibition | Used when SSRIs fail; moderate efficacy | Used cautiously postpartum | Venlafaxine frequently used postpartum; monitor for side effects | [ | |
| Bupropion | Dopamine–norepinephrine reuptake inhibition | Alternative option; especially for fatigue, anhedonia | Limited use in breastfeeding | Limited data in lactation; caution advised | [ | |
| Mirtazapine | Noradrenergic and specific serotonergic action | Often used as augmentation; sedation useful in insomnia | Limited safety data in lactation | Consider if insomnia or appetite loss dominate | [ | |
| Vortioxetine | Multimodal serotonergic activity | Modest efficacy in TRD; well tolerated | Not commonly used in PPD | Cognitive benefit in TRD | [ | |
| Agomelatine | Melatonergic agonist and 5-HT2C antagonist | Mild-moderate benefit in TRD | Limited data in PPD | Non-sedative; supports circadian rhythm | [ | |
| Second-line/Other Antidepressants | TCAs (e.g., amitriptyline) | Serotonin and norepinephrine reuptake inhibition | Used after SSRI/SNRI failure | Not typically used in PPD | Side effect burden, especially anticholinergic | [ |
| Quetiapine, trazodone | Multi-receptor activity | Used for augmentation; quetiapine has evidence in TRD | Not recommended in PPD due to sedation | Monitor metabolic and sedative side effects | [ | |
| Vilazodone, levomilnacipran | Serotonergic and norepinephrine/dopamine action | Considered after SSRI failure | Limited to no use in PPD | Novel agents, limited perinatal data | [ | |
| MAO Inhibitors | Phenelzine, tranylcypromine, etc. | Inhibit MAO-A/B, prevent monoamine breakdown | High efficacy in atypical/TRD | Contraindicated in pregnancy/lactation | Dietary restrictions and hypertensive crisis risk | [ |
| Neurosteroid | Brexanolone (IV allopregnanolone) | Positive allosteric modulator of GABA-A receptors | Not indicated for TRD | FDA-approved for PPD | Rapid action; 60-hour IV infusion required | [ |
| Zuranolone | positive allosteric modulator of GABA-A receptor) | Not indicated for TRD | FDA (2023) approved for PPD | Oral alternative to brexanolone’s IV infusion, with evidence for rapid, sustained symptom control from multiple RCTs. | [ | |
| NMDA Receptor Modulators | Esketamine (intranasal) | NMDA receptor antagonist; enhances glutamate signaling | FDA-approved for TRD; rapid effect | Not approved in pregnancy; possible postpartum use | In-clinic monitoring due to dissociation | [ |
| Ketamine (IV) | Non-selective NMDA receptor antagonist | Effective in 60–70% of TRD cases | Experimental use in severe PPD | Short-acting; some pilot postpartum trials | [ | |
| (2R,6R)-HNK | Ketamine metabolite; NMDA-independent | Promising early trials; non-dissociative | Not yet studied in PPD | Still investigational | [ | |
| Augmentation Strategies | Lithium, atypical antipsychotics | Enhance monoamine function; antipsychotic modulation | Effective as augmentation in TRD | Lithium not preferred during breastfeeding | Requires serum monitoring; side effect risk | [ |
| Immunomodulators | Infliximab, tocilizumab | Anti-cytokine (TNF-α, IL-6) inhibition | Promising in inflammation-related TRD | Not approved or studied in PPD | Off-label; biomarker-guided therapy | [ |
| Anti-inflammatory Agents | NSAIDs (e.g., celecoxib), cytokine blockers | Inhibit peripheral and CNS inflammation | Moderate benefit in inflamed TRD cases | Limited peripartum safety data | GI and cardiovascular risks; adjunctive only | [ |
| Psychedelic-Assisted Therapy | Psilocybin, MDMA | 5-HT2A receptor agonism, neuroplasticity facilitation | Rapid effects in trials for TRD | Not studied or approved for PPD | Requires psychotherapeutic setting | [ |
| Cannabinoids | CBD (cannabidiol) | Endocannabinoid modulation, serotonin activity | Preliminary TRD evidence | Insufficient safety data for PPD | Not FDA-approved; formulation challenges | [ |
| Novel Agents | Kappa opioid antagonists, sigma-1 modulators, etc. | Non-monoaminergic targets | Early-phase trials in TRD | No data in PPD | Potential future treatments | [ |
| Nutritional Adjuncts | Omega-3 fatty acids (EPA/DHA) | Anti-inflammatory; membrane fluidity; serotonin modulation | Safe adjunct in TRD | Safe during pregnancy and lactation | Modest efficacy; neurodevelopmental benefit in PPD | [ |
| Intervention | Modality/Mechanism | Evidence and Efficacy | Level of Evidence (TRD) | Level of Evidence (PPD) | Main Safety Warnings (Perinatal) | References |
|---|---|---|---|---|---|---|
| Cognitive Behavioral Therapy (CBT) (including CBTi) | Psychotherapy to restructure thoughts and behaviors; CBTi targets insomnia | Strong RCT/meta-analysis support; effective monotherapy or adjunct in TRD and PPD | Widely used and effective | Strong efficacy in pregnancy and postpartum | Safe during pregnancy/lactation; flexible delivery (teletherapy, group, individual) | [ |
| Mindfulness-Based Cognitive Therapy (MBCT) | Combines CBT with mindfulness to reduce rumination | Evidence supports relapse prevention in TRD | Effective in residual symptoms, relapse prevention | Limited data, but likely safe and beneficial | Gentle, non-invasive, supports emotional regulation | [ |
| Digital Therapeutics | App-based CBT and mood regulation tools | Growing evidence for mild/moderate TRD | Beneficial as adjunct or for access-limited patients | Under investigation for PPD | High accessibility; digital literacy dependent | [ |
| Virtual Reality Therapy | Immersive environments for therapeutic exposure | Emerging data in TRD, especially PTSD comorbidity | Promising in emotional regulation | Not yet studied in PPD | Costly and niche; not first-line | [ |
| Electroconvulsive Therapy (ECT) | Induces seizure via electrical stimulation | Gold standard in severe TRD (50–70% response) | Widely used in refractory TRD | Rarely used in PPD (case-based) | Not first-line in peripartum due to anesthesia/memory concerns | [ |
| Bifrontal ECT | Modified ECT with fewer cognitive side effects | Comparable efficacy to bilateral ECT | Considered safer cognitively in TRD | No data in PPD | Still requires anesthesia | [ |
| Repetitive Transcranial Magnetic Stimulation (rTMS) | Magnetic pulses stimulate dorsolateral prefrontal cortex | ~50% response in TRD; FDA-approved | Widely used in TRD | Demonstrated safety and efficacy in postpartum depression | Medication-free; non-invasive; safe during lactation | [ |
| Deep TMS (rdTMS) | Reaches deeper cortical and subcortical areas | Some evidence of superior efficacy in TRD | Effective in TRD | Not yet validated for PPD | High cost, limited availability | [ |
| tDCS (Transcranial Direct Current Stimulation) | Low current alters cortical excitability | 30–40% response in TRD | Used as low-cost, portable option | Limited data in PPD | Theoretical safety; not mainstream in perinatal settings | [ |
| Deep Brain Stimulation (DBS) | Implanted electrodes target deep brain regions | Up to 60% response in severe, refractory TRD | Experimental in advanced TRD | Not applicable in PPD | Invasive; contraindicated in pregnancy | [ |
| Neurofeedback | Brainwave training via real-time feedback | Promising early TRD studies | Potential for self-regulation support | No current data for PPD | Training-intensive; not routine | [ |
| Exercise/Physical Activity | Enhances BDNF, endorphins, circadian rhythm | Strong efficacy in mild-moderate depression; adjunct in TRD | Effective adjunct in TRD | Reduces PPD symptoms (SMD −0.41 to −0.53) | Safe, low-cost, improves physical/mental health | [ |
| Mind-Body Practices (e.g., Yoga) | Integrates movement, breathing, and mindfulness | Beneficial in both TRD and PPD | Used as adjunctive support | Particularly effective postpartum | Improves mood, sleep, and bonding | [ |
| Peer/Social Support and Psychoeducation | Group sessions, home visits, non-specialist support | Strong community-based evidence in PPD | Limited evidence in TRD; emerging in group therapy | Effective in reducing PPD, especially in low-resource settings | Safe, culturally adaptable, scalable | [ |
| Gene Therapy | Modifies gene expression via viral vectors | Preclinical success in TRD models | Experimental stage in TRD | No use in PPD | Ethical issues; not ready for clinical use | [ |
| Aspect | Pharmacological Interventions | Non-Pharmacological Interventions | |
|---|---|---|---|
| 1. | Treatment Modalities and Mechanisms | TRD: Targets monoamine systems (serotonin, norepinephrine, dopamine), glutamate (e.g., ketamine), neurosteroids, inflammation. Often biochemical. | TRD: Includes neuromodulation (ECT, TMS, DBS), psychotherapy (CBT, MBCT), and lifestyle/digital tools. Aims to restore neuroplasticity, cognition, emotional processing. |
| 2. | Efficacy and Evidence Base | TRD: Esketamine and ketamine offer rapid symptom relief. Antidepressants often need augmentation. MAOIs and glutamatergic agents show promise. Broad evidence base. | TRD: ECT and rTMS show robust short-term results; CBT/MBCT support long-term remission; digital tools are emerging. |
| 3. | Safety and Side Effects | TRD: Risk of sedation, metabolic and cardiovascular side effects; ketamine has misuse potential. Requires monitoring (e.g., lithium levels, MAOI diets). | TRD: Side effects include cognitive effects (ECT), discomfort (TMS), but minimal systemic toxicity. |
| 4. | Practical Considerations | TRD: Widely available agents; some novel treatments are expensive (e.g., esketamine). Pharmacogenomics in early use. | TRD: Access limited by cost/availability (TMS, DBS); therapy requires time and engagement. Long-term cost-effective. |
- —Deanship of Graduate Studies and Scientific Research at Qassim University
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMaternal Mental Health During Pregnancy and Postpartum · Child and Adolescent Psychosocial and Emotional Development · Adolescent and Pediatric Healthcare
1. Introduction
Peripartum depression (PPD) affects 15–20% of expecting mothers worldwide in the months following childbirth, also called postpartum depression. Effective management of PPD is not only a clinical priority due to profound implications for maternal, fetal, and infant health but also a public health imperative [1,2]. To discriminate between different interlinked terminologies clearly, it is evident that peripartum depression (PPD) is a subtype of major depressive disorder (MDD) occurring during pregnancy or within 12 months postpartum. MDD is characterized by persistent low moods, anhedonia, exhaustion, and cognitive deficits lasting at least two weeks. Treatment-resistant depression (TRD) is defined as a major depressive episode that fails to respond to at least two adequate antidepressant trials at an adequate dose and duration, consistent with established TRD criteria. TRD significantly impairs maternal health, child development, and family functioning. Treatment-resistant peripartum depression (TRPD) is diagnosed when the challenges of both PPD and TRD occur during the peripartum period [3,4].
Despite multiple antidepressant trials, reported studies observed that up to 40% of peripartum depressed women may not respond to the initial therapy, while up to 60% do not achieve remission [4,5], and these figures may indicate a pressing need to better understand and manage TRD. Treatment-resistant peripartum depression (TRPD) is defined as peripartum depression that fails to remit after at least two adequate trials of antidepressant therapy, consistent with established TRD criteria [6]. TRPD can severely impact a mother’s physical and mental health and ability to form strong attachments to her child, leading to a negative impact on a child’s health, increasing the risk of behavioral problems, cognitive challenges, and developmental delays [7,8,9]. The condition may exhibit a variety of typical symptoms, including consistent sorrow, loss of interest in activities, exhaustion, impatience, changes in appetite, sleep troubles, and concentration difficulties and are linked to certain conditions, according to the DSM-V criteria [10]. In addition, anxiety, mood swings, and suicidal thoughts may occur frequently in individuals with TRPD [11,12].
This review focuses exclusively on maternal treatment-resistant peripartum depression (TRPD), as most available epidemiological data and clinical trials address women, reflecting both the higher prevalence of peripartum depression in mothers and substantial gaps in paternal TRPD research. While paternal peripartum depression affects approximately 10% of fathers, the literature on treatment resistance, unique risk factors, and specific interventions in fathers remains limited due to pervasive stigma and under-recognition in clinical settings. Future reviews should consider this unmet need as this evidence base grows.
1.1. Associated Factors/Comorbidities
A complex interaction of genetic, neurobiological, and psychosocial factors is linked with TRD. Genetic factors have been found to influence both a person’s chance of getting depression and how likely they are to respond to treatment. During the peripartum period, hormonal fluctuations, particularly in estrogen and progesterone, have been associated with increased risk for depression and may contribute to treatment resistance [13].
While psychosocial factors contribute to peripartum depression and may increase TRPD risk, biological mechanisms—such as altered serotonin, dopamine, and norepinephrine neurotransmitter levels, and HPA axis dysregulation—are also implicated in its pathophysiology [4,14].
TRD is frequently combined with other mental health conditions, such as anxiety, post-traumatic stress disorder, and substance use disorders. These comorbidities complicate diagnosis and treatment, and are associated with increased risks of cardiovascular disease, reduced quality of life, and functional impairment. Additionally, medical conditions like thyroid dysfunction and chronic pain contribute to reduced productivity and higher healthcare costs, which may further influence the incidence and severity of TRPD [4,14].
1.2. Diagnostics Obstacles
Accurate diagnosis remains challenging due to the complex and varied nature of TRD in individuals with peripartum depression, and its overlap with other mental health problems. Persistent depressive symptoms despite at least two adequate antidepressant trials, in the absence of reliable biomarkers, complicate clinical decision-making [4].
It is important to note that a considerable proportion of evidence for TRPD is extrapolated from general TRD studies. Due to physiological, hormonal, and psychosocial differences in the peripartum period, the generalizability of TRD findings to TRPD may be limited. Dedicated perinatal research is urgently needed.
The present review highlights the current challenges and emerging evidence, with critical assessment of the efficacy and limitations of both pharmacological and non-pharmacological interventions in treatment-resistant depression (TRD) and peripartum depression (PPD), to inform clinical practice and guide future research to better support women experiencing treatment-resistant peripartum depression (TRPD).
2. Methods
In the present review, the search strategy is based on PRISMA-Preferred Reporting Items for Systematic Reviews and Meta-Analysis criteria [15] to evaluate the current and emerging therapies for individuals with treatment-resistant peripartum depression.
The inclusion criteria were based on a systematic search of PubMed, Cochrane Library, and EMBASE for English-language articles published between 2000 and 2024. The review focused on (applied filters: abstract, full text, meta-analysis, systematic review) with a combination of Medical Subject Headings (MeSH) and free-text terms were used, including (“treatment resistant depression” OR “TRD”) AND (“peripartum depression” OR “postpartum depression” OR “perinatal depression” OR “PPD” OR “treatment resistant peripartum depression” OR “TRPD”) AND (“therapy” OR “treatment” OR “intervention”). Search terms included “peripartum depression”, “postpartum depression”, and “perinatal depression” were not entered as exact phrases to maximize inclusion of international studies and nomenclature, but as Boolean combinations to maximize sensitivity and capture relevant variations in terminology.
Studies were limited by exclusion criteria, including studies not related to peripartum or postpartum depression, outcomes not attributable to women, not a quantitative study, not meeting criteria for treatment resistance (TRD/PPD/TRPD), not published in a peer-reviewed journal, published in another language, and having insufficient information. However, we restricted our inclusion to studies on maternal TRPD to ensure consistency in the population studied and due to the scarcity of high-quality research on paternal TRPD. Likewise, while child developmental outcomes are mentioned in context, our primary focus remains on maternal outcomes and interventions, as dictated by the scope and prevalence of current evidence.
After screening, the initial search yielded 142 articles; only 67 articles were qualified for eligibility. Although this number may limit the generalizability of some conclusions, it provides an analytically manageable and clinically meaningful dataset for review. A larger set may have introduced redundancies or diluted specificity. Most current PPD/TRPD studies are limited by small sample sizes, heterogeneity in patient populations, and short-term follow-up; this constrains the generalizability of findings and warrants further large-scale, long-term trials. The quality assessment was performed using the Newcastle–Ottawa Scale for observational studies and the Cochrane Risk of Bias tool for randomized trials. Of the 67 included studies, quality appraisal analyses found that 38 were at low risk of bias, 20 at moderate risk, and 9 at high risk. High-quality studies were prioritized in the synthesis. With two independent reviewers’ assessments, discrepancies were resolved by consensus (Figure 1).
2.1. TRPD Current Therapeutics
Numerous interventions were evaluated in the previous studies, including pharmacotherapy, psychotherapy, and neuro-modulation techniques. Below, we provide a more detailed synthesis of the evidence for each intervention, with emphasis on effectiveness and limitations in the peripartum context. Table 1 and Table 2 summarize the targeted pharmacological and non-pharmacological interventions for TRD and PPD, with details of available drugs, mode of action, and outcomes where available. Table 3 depicts the integrated comparison with various fundamental aspects of these interventions.
2.2. Pharmacological Interventions
Pharmacological interventions for TRD/PPD include switching to a different antidepressant, augmenting current medication, or combining multiple antidepressants. SSRIs are commonly used as first-line pharmacological therapy for peripartum depression, but evidence for their effectiveness in TRPD is mixed. Some studies report modest improvements, but remission rates remain low in this population [6]. Intranasal esketamine [16], immunomodulators [17], and glutamate modulators [18] have been explored in small trials, but data specific to peripartum populations are limited.
The main pharmacological bridge between TRD and PPD is SSRIs and SNRIs, as demonstrated in Table 1, suggesting that, with sertraline considered safest in lactation, brexanolone and zuranolone are unique to PPD [19,20]. The other drugs, such as ketamine/esketamine, show rapid efficacy, while omega-3s are low-risk, evidence-supported adjuncts in both TRPD, especially for severe cases having inflammation-linked symptoms. Emerging evidence indicates that a subset of severe TRPD cases exhibits elevated inflammatory markers (e.g., C-reactive protein, interleukin-6), suggesting an inflammation-linked endophenotype. This raises the prospect of targeted immunomodulatory or anti-inflammatory therapies, though further research is needed to clarify treatment response and the impact of perinatal hormonal-immune changes on inflammation-driven depression [20]. Moreover, several agents like MAOIs, TCAs, and atypical antipsychotics are effective in TRD but are not suitable during the peripartum period due to safety concerns.
2.3. Augmentation Strategies
Augmentation Strategies involve adding a second medication to an existing antidepressant regimen. Several medications, such as lithium and atypical antipsychotics, have been investigated as potential augmenting agents in TRD patients [21]. Switching to a different medication and adding adjunctive therapies were associated with a higher likelihood of remission in TRD than augmenting or combining medications [22]. However, there is little data to back up medication used for TRD [6], but most studies excluded peripartum populations, limiting generalizability [23]. Overall, there is a paucity of high-quality evidence specific to TRPD, and most recommendations are extrapolated from general TRD populations.
The other treatment option is the use of adjunctive drugs for non-response or partial response to an antidepressant, including Aripiprazole, Quetiapine, and Risperidone as a first line, and Brexpiprazole, Bupropion, Lithium, Mirtazapine/Mianserin, Modafinil, Olanzapine, Triiodothyronine as a second line, and Esketamine for TRD [24]. A rational pharmacologic approach for TRPD includes reevaluating diagnosis, assessing prior treatment response and tolerability, using adjunctive medications judiciously, discontinuing ineffective medications, and closely monitoring symptoms and adverse effects [25].
2.4. Non-Pharmacological Interventions
Non-pharmacological interventions for TRD include psychotherapy, electroconvulsive therapy (ECT), and transcranial magnetic stimulation (TMS). ECT has demonstrated response rates of 60–70% in severe TRD, including peripartum cases, but stigma and side effects limit its use [36]. Digital therapeutics [37] and virtual reality therapy [38] are evidence-based therapies potentially effective in treating depression, including TRD. Smartphones and other electronic devices can access software-based interventions, or “digital therapeutics,” explicitly designed to treat depression and other mental health conditions. TMS and digital therapeutics have shown promise in non-peripartum TRD, but data in peripartum populations are sparse and further research is needed [39]. Virtual reality therapy and neurofeedback are emerging modalities with limited but growing evidence.
Psychotherapy, particularly cognitive-behavioral therapy (CBT) and interpersonal therapy (IPT), is recommended for TRPD, especially in individuals with a history of trauma or comorbid anxiety disorders. However, there is insufficient evidence to support psychotherapy as a stand-alone treatment for TRPD; most studies suggest benefit as part of a multimodal approach. Lifestyle modifications such as regular exercise, a healthy diet, and stress management may provide additional benefit [40,41].
Table 2 explains the double comparison between non-pharmacological interventions effective in both TRD and PPD, the CBT and exercise. Efficacious with high safety in perinatal contexts, while rTMS shows strong dual-utility, and is FDA-approved for TRD and supported by meta-analyses in PPD. Peer support is uniquely potent in PPD, especially in low-resource or culturally sensitive contexts; however, several invasive or high-tech interventions (DBS, ECT, VR) are TRD-specific and not applicable to peripartum populations due to safety or practicality. Additionally, Lifestyle interventions such as exercise and yoga offer low-cost, high-accessibility options particularly suited for postpartum recovery and mood support in TRPD.
Pharmacological and non-pharmacological interventions with TRD and PPD in comparison with different aspects like treatment modalities and mechanisms, efficacy and evidence base, safety and side effects, and practical considerations were illustrated in Table 3. It suggests that the pharmacological options remain foundational, especially in moderate to severe cases of TRD and PPD but are often limited due to safety concerns during pregnancy and lactation in PPD. Multimodal strategies and frequent augmentation are the basic requirements for the TRD treatment, while early detection and individualization with low-risk support systems helped PPD interventions. However, non-pharmacological approaches offer safe, effective, and scalable alternatives, especially important in TRPD settings where drug-free treatments are preferred.
2.5. Critical Appraisal
This review offers valuable pathways toward personalized and safe care for peripartum depression, highlighting that both pharmacological and non-pharmacological interventions each with unique strengths and limitations.
While pharmacological therapies remain foundational, especially for moderate to severe TRPD, they are often constrained due to fetal or neonatal safety concerns [12]. Despite SSRIs like sertraline having a well-established safety profile during lactation and significant efficacy in moderate to severe cases [59]. Being widely used off-label for PPD with favorable safety data, the absence of FDA approval can lead to insurance restrictions and varying levels of acceptance among clinicians and patients. This drug has strong evidence for efficacy in PPD but is not specifically FDA-approved for PPD; caution is warranted and individual risk–benefit must be considered. Conversely, FDA-approved agents like brexanolone and zuranolone increase access and clinician confidence but face challenges related to cost and delivery (e.g., brexanolone’s 60-hour infusion requirement).
MAOIs have high efficacy in TRD but are not recommended in perinatal populations due to significant safety concerns. Caution is advised with other antidepressants, and shared decision-making is critical, especially during pregnancy, where the balance between maternal benefits and fetal risks must be carefully navigated [60].
Recently, the role of GABA–glutamate dysregulation has emerged as a key mechanism in TRD and TRPD, particularly through modulation of GABA-A receptors. Novel agents like brexanolone and zuranolone, a GABA-A receptor modulator and ketamine analogs specifically approved for PPD, have demonstrated rapid, sustained symptom relief, though access and cost remain barriers [19]. It provides a more practical option for patients while maintaining robust efficacy in improving depressive symptoms within days, and may represent a breakthrough for women who do not respond to traditional antidepressants [19,20].
In contrast, non-pharmacological interventions—notably psychotherapy modalities such as cognitive behavioural therapy (CBT) and mindfulness-based cognitive therapy (MBCT), neurostimulation techniques including repetitive transcranial magnetic stimulation (rTMS), and adjunctive lifestyle interventions such as structured exercise—offer safe, effective, and increasingly accessible alternatives or complements to pharmacotherapy.
These approaches avoid systemic drug exposure and align well with patient preferences for non-medication options, especially during pregnancy and breastfeeding. However, barriers including limited availability, treatment adherence challenges, and costs persist, underscoring the need for expanded infrastructure and integration of digital therapeutics to improve reach. Meta-analyses support CBT and MBCT as highly efficacious for reducing depressive symptoms, while rTMS and physical activity show moderate to strong benefits with minimal risk [57,61,62,63,64,65].
The limited inclusion of peripartum women in clinical trials has left a significant gap in safety data. International bodies are now calling for better-designed studies and registries to ensure evidence-based pharmacological care in this vulnerable population. Personalizing pharmacological strategies in TRPD requires careful assessment of prior treatment responses, safety profiles during pregnancy and lactation, and close symptom monitoring. More studies are needed to evaluate the safety and effectiveness of these treatments; for those who have not reacted to conventional antidepressant therapy, the fact that so many alternative therapies exist is reassuring that there may still be hope.
2.6. Challenges and Prospects
The preceding sections provided an integrated, section-by-section critique of pharmacological, augmentation, and non-pharmacological strategies, while this section highlights overarching challenges across all approaches.
Treatment-resistant peripartum depression (TRPD) is the worldwide health issue impact people from various cultures and geographical areas, particularly complex for expecting mothers and has significant challenges besides other genders, like common fluctuations in hormonal levels and/or comorbid conditions and family and social pressures, inhibition of willingness to seek treatment, and further exploitation to worsen the depressive symptoms and complicate the treatment of TRPD [66,67].
It is assumed that in clinical practice, the most realistic and effective approach to TRPD is a personalized, multidisciplinary treatment model that judiciously integrates pharmacological and non-pharmacological strategies. This model prioritizes symptom severity, patient safety, and preference while leveraging the complementary strengths of rapid symptom control via medication and sustainable remission supported by psychotherapy and neurostimulation.
Long-standing depression, variability in treatment response, financial stress, personal and social issues, and women’s reproductive health are other contributing factors that could further complicate the issue, and it may require more intensive and multifaceted treatment approaches to address these challenges. Looking forward, ongoing research into novel agents with improved safety profiles, refinement of neurostimulation protocols, and scalable digital therapeutics hold promises for advancing TRPD care. Equally important is the enhancement of the perinatal mental health services infrastructure to ensure equitable access to comprehensive treatment options.
2.7. Recommendations for TRPD
Early identification of TRPD, close monitoring, and collaborative decision-making with patients are paramount to optimizing outcomes. Strengths of the current literature include growing recognition of the need for tailored approaches in peripartum populations and emerging evidence for novel interventions (e.g., digital therapeutics, neuromodulation). However, weaknesses include small sample sizes, lack of standardized definitions for TRPD, and limited long-term outcome data.
Individual treatment decisions should consider the patient’s preferences, risks, and potential advantages of using pharmacological or non-pharmacological interventions for TRD/PPD in women. Future studies should work to deepen our comprehension of the root causes and risk factors for TRD/PPD and create secure and efficient treatment alternatives for the women at risk for TRPD and offer prompt and effective alternative therapies; raising awareness and enhancing screening and diagnostic methods is vital. To improve outcomes for this vulnerable population, researchers and clinicians are urged by this critical review to give alternate treatments for TRPD in women with peripartum depression top priority.
An interdisciplinary approach is added in the recommendations involving the team of experts, which may include psychiatrists, psychologists, social workers, nutritionists, and other specialists to offer the most appropriate treatment for TRPD patients according to the individual’s needs, with an evidence-based treatment plan.
Furthermore, adopting and adapting effective framework models (e.g., the “Perinatal Mental Health Community Services” model-UK; MumSpace model perinatal depression and anxiety—Australia), that demonstrate investment in multidisciplinary perinatal mental health teams, universal screening, integrated care pathways, and digital mental health solutions can dramatically improve maternal outcomes and service access. Using such proven models in local health systems should be prioritized in future policy and practice initiatives [68,69].
In summary, the future of PPD/TRPD care lies not in choosing between pharmacological and non-pharmacological interventions, but in strategically combining them to support each woman’s unique needs, values, and life circumstances. Continued research, education, and policy-level commitment are essential to closing the treatment gap and enhancing the mental health of mothers and their children.
3. Conclusions
Treatment-resistant peripartum depression (TRPD) poses a significant clinical challenge due to the complex interplay of maternal physiological changes, fetal safety considerations, and the profound psychosocial impact of untreated maternal mental illness. This review examines various contributing factors, challenges, and recommendations that highlight the potential interventions for the TRD/PPD, which offers a substantial therapeutic issue in women with limited evidence-based treatment options and considerable negative impacts on mother and child health outcomes.
Comparison of the relative effectiveness of pharmacological interventions like SSRIs, brexanolone, and zuranolone demonstrates moderate-to-strong evidence for symptom reduction in TRPD (particularly moderate-to-severe cases), while non-pharmacological methods such as CBT and rTMS also show robust efficacy and often superior safety/tolerability profiles in perinatal women. Meta-analyses suggest that the magnitude of benefit for CBT in mild-to-moderate PPD may equal or exceed that of some pharmacological agents, and combined therapy is recommended for the most resistant cases.
Our findings imply that no one treatment works for all cases of TRPD and that a combination of therapy and an interdisciplinary approach with a team of experts may be the most successful strategy.
Future research should prioritize randomized controlled trials specifically enrolling peripartum individuals with TRD; standardized definitions of treatment resistance and head-to-head comparisons of interventions, with a critical lens on their feasibility, efficacy, and safety within the peripartum context; and also address safety data gaps by including pregnant and lactating participants in clinical trials.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sidhu G.S. Sidhu T.K. Kaur P. Lal D. Sangha N.K. Evaluation of Peripartum Depression in Females Int. J. Appl. Basic. Med. Res.2019920120510.4103/ijabmr.IJABMR_23_1931681543 PMC 6822329 · doi ↗ · pubmed ↗
- 2Gelaye B. Rondon M.B. Araya R. Williams M.A. Epidemiology of maternal depression, risk factors, and child outcomes in low-income and middle-income countries Lancet Psychiatry 2016397398210.1016/S 2215-0366(16)30284-X 27650773 PMC 5155709 · doi ↗ · pubmed ↗
- 3Alzahrani J. Al-Ghamdi S. Aldossari K. Al-Ajmi M. Al-Ajmi D. Alanazi F. Aldossary A. Alharbi A. Postpartum Depression Prevalence and Associated Factors: An Observational Study in Saudi Arabia Medicina 202258159510.3390/medicina 5811159536363552 PMC 9696672 · doi ↗ · pubmed ↗
- 4Guintivano J. Manuck T. Meltzer-Brody S. Predictors of Postpartum Depression: A Comprehensive Review of the Last Decade of Evidence Clin. Obstet. Gynecol.20186159160310.1097/GRF.000000000000036829596076 PMC 6059965 · doi ↗ · pubmed ↗
- 5Al Nasr R.S. Altharwi K. Derbah M.S. Gharibo S.O. Fallatah S.A. Alotaibi S.G. Almutairi K.A. Asdaq S.M.B. Prevalence and predictors of postpartum depression in Riyadh, Saudi Arabia: A cross-sectional study P Lo S ONE 202015 e 022866610.1371/journal.pone.022866632040495 PMC 7010279 · doi ↗ · pubmed ↗
- 6Yonkers K.A. Blackwell K.A. Glover J. Forray A. Stroud L.R. Antidepressant use in pregnant and postpartum women Annu. Rev. Clin. Psychol.20141036939210.1146/annurev-clinpsy-032813-15362624313569 PMC 4138492 · doi ↗ · pubmed ↗
- 7Prenoveau J.M. Craske M.G. West V. Giannakakis A. Zioga M. Lehtonen A. Davies B. Netsi E. Cardy J. Cooper P. Maternal postnatal depression and anxiety and their association with child emotional negativity and behavior problems at two years Dev. Psychol.201753506210.1037/dev 000022128026191 PMC 5191902 · doi ↗ · pubmed ↗
- 8Murray L. Halligan S. Cooper P. Effects of Postnatal Depression on Mother–Infant Interactions and Child Development The Wiley-Blackwell Handbook of Infant Development Wiley Hoboken, NJ, USA 201019222010.1002/9781444327588.ch 8 · doi ↗