Improving Advanced Communication Skills Towards the Family System: A Scoping Review of Family Meeting Training in Oncology and Other Healthcare Settings
Sara Alquati, Loredana Buonaccorso, Nuria Maria Asensio Sierra, Francesca Sassi, Francesco Venturelli, Maria Chiara Bassi, Stefano David Scialpi, Silvia Tanzi

TL;DR
This review summarizes research on training healthcare professionals to conduct family meetings, highlighting a focus on communication skills but a lack of interprofessional and long-term approaches.
Contribution
The study provides a comprehensive overview of family meeting training for healthcare professionals, emphasizing communication skills and gaps in interprofessional and longitudinal training.
Findings
Communication skills training is the dominant focus in family meeting education for healthcare professionals.
There is a lack of interprofessional collaboration and long-term assessment in family meeting training programs.
Role-play and simulation are the most common teaching methods used in these training programs.
Abstract
This review aimed to provide an overview of the available research evidence on family meetings education for healthcare professionals. We discussed some specific findings that emerged from our data, which we believe can guide clinicians in designing effective interventions. Data revealed that communication skills training dominated the literature. The topic of communication skills is directly related to the theoretical frameworks of the training, which emphasize the importance of empathy and active listening in communicating and supporting the family system. The training topics are related to advanced communication, but there is a lack of an interprofessional perspective and long-term assessment of the skills learned. According to clinical practice guidelines, family meetings should be conducted by a multiprofessional team, including a physician and a nurse or another key figure…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
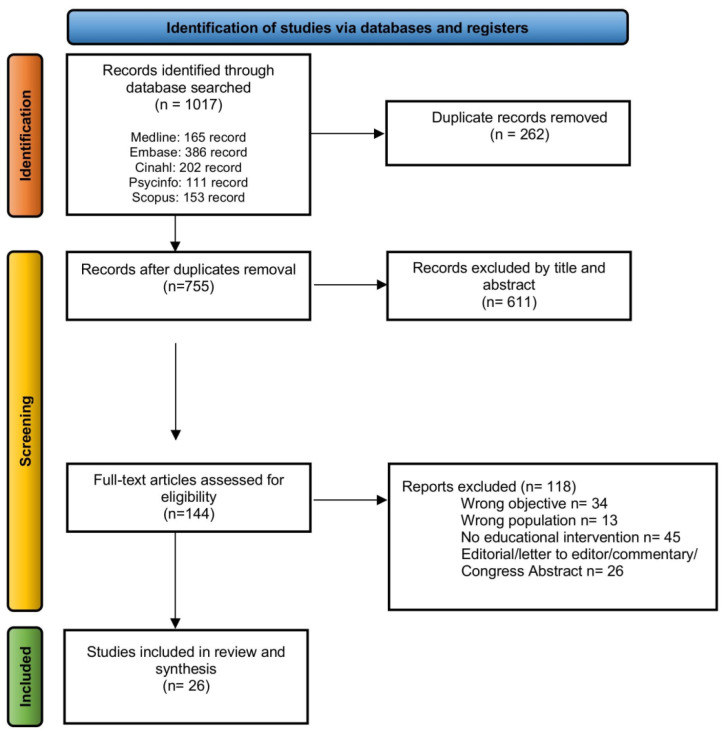 Figure 1
Figure 1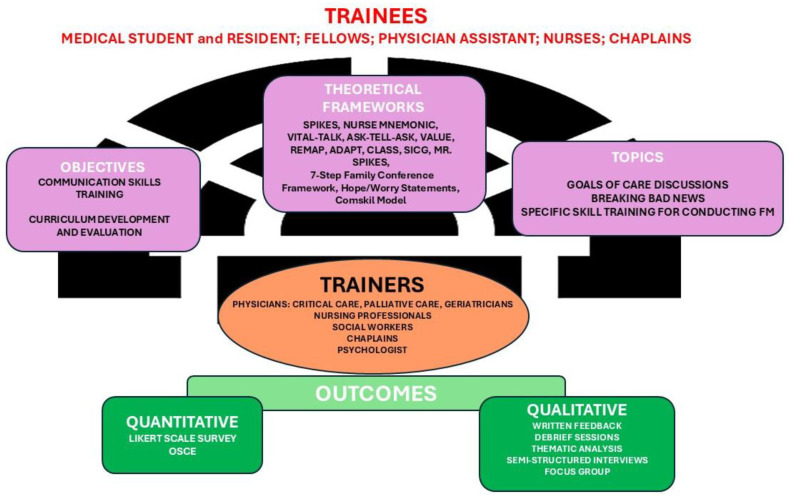 Figure 2
Figure 2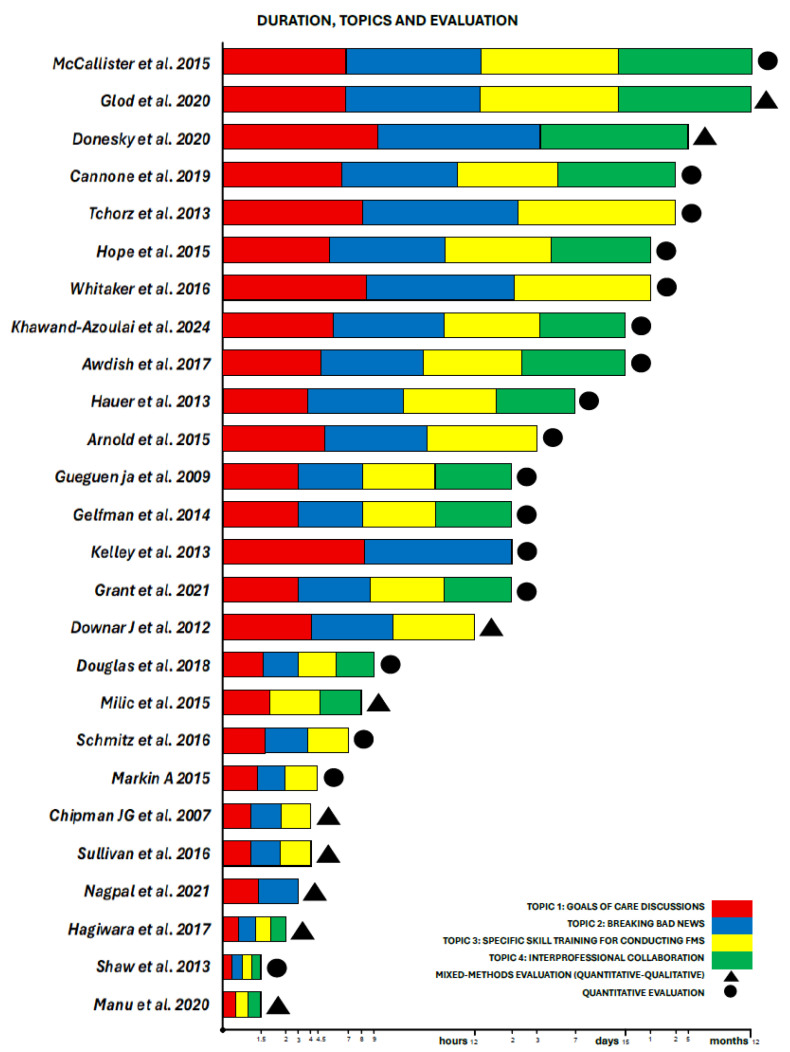 Figure 3
Figure 3- —Italian Ministry of Health
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPalliative Care and End-of-Life Issues · Patient-Provider Communication in Healthcare · Family and Patient Care in Intensive Care Units
1. Background
Effective communication between patients, families, and healthcare professionals (HPs) is essential for high-quality care [1]. The literature indicates that honest and open communication with cancer patients can improve adherence to treatment programs [2,3] and benefit physicians [4]. Family meetings (FMs) are clinical encounters in a structured space involving the patient, their family, and caregivers conducted for multiple purposes, including sharing information and concerns, clarifications regarding goals of care, discussions on diagnosis, treatment, prognosis, and the development of a plan for the care and assistance of the patient and their family members [5,6,7].
FMs have been shown to improve concordance of care with expressed wishes and to reduce post-traumatic stress disorder, anxiety, and depression among bereaved family members [8,9]. They are also associated with reduced length of inpatient stay and higher quality ratings of the dying experience [10]. Although FMs are often used in the patient care pathway, data show how infrequently family members’ concerns are addressed as a fundamental element of family care, which indirectly affects patient care [11,12,13].
The literature shows that most HPs do not receive specific training and consequently do not feel adequately prepared to participate, which can accentuate the challenges of conducting them effectively [11,12]. It is widely documented that developing and implementing communication training courses is necessary for hospital HPs, since difficult conversations frequently occur in hospital settings, and all HPs should receive specific training [2,6,14,15,16].
This scoping review aims to provide an overview of the available research evidence on FMs’ education for HPs.
2. Methods
The review question was “How are training programs on family meetings for healthcare professionals designed, organized and evaluated?”. Following the Arksey and O’Malley framework [17], our scoping review process comprised five key phases: research question formulation, study identification and selection, data charting, data collection and synthesis, and results reporting. This review was reported following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses-extension for Scoping Review (PRISMA-ScR) guidelines [18]. The PCC (Population-Concept-Context) framework was used to structure the search strategy and to define the inclusion criteria [19].
Review protocol has been registered in the OSF registry (https://doi.org/10.17605/OSF.IO/2Y836).
2.1. Search Strategy
We conducted an electronic search of the literature from inception up to 28 February 2025 on the following databases: MEDLINE (through PubMed), Embase, CINAHL, PsycINFO, and Scopus. We included articles in English, Italian, and Spanish. The search strategy employed the following terms: (‘family meeting’[Title/Abstract] OR ‘family conference’[Title/Abstract]) AND (education* OR learning OR training OR course* OR workshop* OR teaching OR seminar* OR class* OR instruction). No additional searching was conducted, but we screened the reference list of included articles to identify additional relevant publications.
2.2. Inclusion Criteria
We included studies that described an educational intervention on FMs (Concept) aimed at HPs in all settings of care and students of medicine and nursing sciences (Population) treating adult patients (>18 years old) with oncological and non-oncological diseases (Context).
We adopted a comprehensive approach to identify eligible educational intervention, starting from Moneymaker’s definition of FM [5]: “The Family Meeting are meeting between the patient, their family and healthcare professionals are undertaken for multiple purposes including the sharing of information and concerns, clarifying the goals of care, discussing diagnosis, treatment, prognosis and developing a plan of care for the patient and family carers”. The eligible interventions included FMs and family conference training. We included studies utilizing diverse research methodologies, encompassing quantitative, qualitative, and mixed methods programs. Outcomes were described when available in the included studies to provide information about how training was structured and evaluated.
2.3. Exclusion Criteria
We excluded studies if they (1) described an educational intervention on advanced communication without a specific focus on FMs; (2) included only pediatric settings or pediatric HPs. We also excluded conference abstracts, case reports, systematic reviews, expert opinions, guidelines, ongoing trials, protocol articles, and book chapters.
2.4. Screening and Selection of Studies
Four authors (S.A., L.B., A.S.N.M., F.S.) independently screened titles and abstracts on inclusion and exclusion criteria. After multiple screening rounds, a 100% agreement was reached on articles judged to be eligible for full-text examination. All potentially eligible articles were independently examined in full text by four authors working in two evaluation groups. Final eligibility decisions required 100% consensus, with a supervising author (ST) consulted to resolve any discrepancies. The results of the study selection process are summarized in the flow chart (Figure 1).
2.5. Data Extraction
Two reviewers (SA and LB) performed data extraction from included full-text articles using a data extraction tool developed by the working group. The data extraction form included the first author’s name, year of publication, country, objective, study design, trainers, trainees, setting and duration of training, delivery of intervention, type/program of training, quantitative evaluation tools, qualitative evaluation, quantitative and qualitative outcomes, and refeence to the definition of FM (Table 1).
2.6. Quality Assessment of Included Studies
Given the descriptive aims of the scoping review, according to Johann Briggs institute guidance for scoping review, it was deemed that the assessment of the quality of included studies was not needed [19].
2.7. Synthesis of the Results
The results from the included studies were reported according to the following topics: Study Objective, Study Design, Trainers, Trainees, Setting of Training, Intervention (Duration, Teaching Methods, Theoretical Framework), Topics, and Evaluation of Training (Quantitative Evaluation Tools and Outcomes, Qualitative Evaluation and Outcomes). In Figure 2, we summarized the articles included in the scoping review, highlighting the principal characteristics of the intervention: -objectives, theoretical frameworks and the topics; -trainers and trainees; -outcomes. In Figure 3, we summarized the highlighting characteristics of the analyzed studies.
3. Results
The search yielded 1017 records, which were reduced to 755 after duplicate removal. Initial title/abstract screening excluded 611 more articles. Of the 144 full-text articles retained for further screening, 121 were discarded primarily because the sample did not involve HPs or students, or lacked focus on FMs training. Other papers were excluded because of editorials, letters to the editor, commentaries, and congress abstracts (Figure 1). Twenty-six articles were ultimately included in the scoping review (Table 1).
Geographically, studies focused on North America, with only one Canadian study [43] and no European studies. The training had as its primary aims the communication skills [20,21,22,23,26,27,28,29,30,31,32,33,34,35,36,37,38,39,41,42,43,44,45] and curriculum development/evaluation [43,44,45]. For the most part, palliative care physicians served as trainers [20,22,24,25,26,27,29,33,34,36,37,38,39,40]. Studies predominantly targeted physicians, particularly medical students. Only four studies involved nurses. The role-play and simulation were the most common delivery methods. Quantitative methods predominated, with a smaller proportion [22,33,35,38,43] incorporating longitudinal follow-up to assess skill retention.
3.1. Study Objective
The systematic analysis revealed two primary aims: (i) communication skills training and (ii) curriculum development and evaluation.
(i)Communication Skills Training [20,21,22,23,26,27,28,29,30,31,32,33,34,35,36,37,38,39,41,42,43,44,45]
Studies in this category aimed to enhance specific communication competencies, including delivering bad news or prognosis [33], conducting FMs [29], and discussing goals of care [22]. For example, Khawand-Azoulai et al. [20] focused on end-of-life discussions for medical students; Sullivan et al. [31] targeted Intensive Care Unit (ICU) residents’ skills in family communication; and Chipman et al. [45] developed an Objective Structured Clinical Examination (OSCE) to assess surgical residents’ ability to lead family conferences and formalized assessment tools to evaluate surgical residents’ conference leadership skills. Training emphasized collaborative skills across disciplines. For example, Grant et al. [21] trained physician assistant students and chaplains jointly to address spiritual dissonance during prognosis delivery; Milic et al. [37] empowered nurses to engage in interdisciplinary prognosis discussions.
(ii)Curriculum Development and Evaluation [43,44,45]
These studies piloted or assessed novel curricula: Kelley et al. [40] evaluated a retreat-style course for geriatrics fellows; Glod et al. [24] designed a hybrid ICU FMs curriculum integrating didactics with real-world facilitation; while Manu et al. [25] tested a seminar format for dementia-related communication.
3.2. Trainers
Physicians served as trainers in 24 of the 26 studies reviewed [20,21,22,24,25,26,27,28,29,30,31,32,33,34,35,36,37,39,40,41,42,43,44,45]. For the most part, they were palliative care physicians [22,25,26,27,29,30,31,33,34,39,40,43,44,45], followed by critical care specialists [24,27,28,31,32,33,34,36,37,43,45]. Nursing professionals participated explicitly in seven studies [20,24,27,28,34,37,45] of training programs. Other HPs included social workers [20,24], chaplains [21,37], and psychologists [20,36,37].
Most studies reported multiprofessional training teams [20,21,22,24,25,28,30,31,33,34,36,37,38,39,40,41,42,43,44,45], for example physician-and-nurse trainer teams [20,24,28,31,34,37,38,43,45].
3.3. Trainees
A total of 1914 trainees participated across 26 studies. Medical students represented the largest cohort (n = 851), driven by three studies: Hagiwara et al. (n = 674) [29], Tchorz et al. (n = 97) [42], and Khawand-Azoulai et al. (n = 80) [20]. Trainee roles exhibited significant heterogeneity across disciplines. Medical residents constituted the second-largest group [20,23,26,27,28,32,35,36,37,39,40,41,44,45], primarily from internal medicine disciplines [22,25,31,32,35,39], with additional representation from surgery [30,45] and neurology [25,27]. Fellows and physician assistant students were prominent in critical care and inter-professional contexts [21,44]. Internal medicine was the most common specialization, primarily made up of residents engaged in ICU rotations [24,31,32,35,39] or palliative care training [24,35,39]. Critical care included fellows [33,34,36,43], nurses [37,41] and residents, reflecting the ICU context of most interventions [24,28,31,32,33,34,35,36,37,41,43,45]. Other HPs included chaplains [21,23,41].
3.4. Setting of Training
The distribution of training settings reveals a pronounced emphasis on clinical environments: ICU [23,28,31,32,33,37,41,42,44] and non-ICU [20,22,25,30,39,44]. Simulation centers also emerged as a setting [21,22,23,26,44,45] providing controlled environments for high-stakes communication practice. Also, exclusively academic-hosted studies were reported, primarily using classrooms or lecture halls [21,22,26,29,45].
A distinct set of studies [21,24,25,26,31,32,33,35,36,37,38,39,41,42,44,45] adopted mixed settings, blending simulation with clinical or academic environments. Only one study [33] utilized a specialized non-clinical, off-site retreat setting for ICU fellows (no more specifics provided). Direct involvement of oncology staff (trainees or trainers) resulted in rare cases, with only a few exceptions where oncology intersects with palliative care or surgical training. Only two studies explicitly include oncology professionals as trainees: -Cannone et al. [26] trained oncology fellows and radiation oncology residents at the Center for Learning and Innovation in Lake Success, NY—a setting affiliated with cancer and palliative care programs; -Gueguen et al. [44] involved multi-specialty professionals, including medical, surgical, and radiation oncologists, in a communication skills workshop at Memorial Sloan-Kettering Cancer Center in New York.
3.5. Intervention
We analyzed the type of intervention through three principal topics: (i) duration; (ii) teaching methods; and (iii) theoretical framework.
(i)Duration
The data demonstrate a preference for longitudinal training formats [20,23,24,26,32,34,36,39,42], with some programs spanning weeks to months, exemplified by McCallister’s [36] year-long pulmonary fellowship curriculum and Tchorz’s [42] eight-week surgical clerkship incorporating structured clinical examinations. Shorter interventions were distributed between intensive single-day workshops [21,23,25,37,41,43], including Milic’s [37] 8 h nursing communication training, and focused multi-day retreats [33,38,40,43,44], such as Arnold’s [33] three-day intensive care fellowship program. Compact 1–4 h sessions accounted for the other interventions [20,22,24,27,29,31,35], typified by Nagpal’s [22] 3 h simulation for internal medicine residents and Sullivan’s [31] 4 h ICU communication workshop.
(ii)Teaching Methods
The pedagogical approach highlighted a preference for active learning methodologies. Simulation-based training dominates, employed in 24 studies through various formats including standardized patient encounters, role-playing exercises, and high-fidelity clinical scenarios [20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,40,41,42,43,44,45]. This experiential approach frequently combines with other methods in blended designs, creating multimodal learning experiences that integrate didactic instruction with hands-on practice and clinical application [21,22,25,26,27,28,29,30,31,32,33,34,35,37,38,40,43,44,45].
(iii)Theoretical Framework
The most frequently cited model was SPIKES [46], a six-step protocol for delivering bad news, which appeared in 11 out of 26 articles [20,24,26,27,29,34,36,37,38,41,43]. This model emphasizes structured communication through the steps of Setting, Perception, Invitation, Knowledge, Emotions, and Strategy/Summary. The NURSE mnemonic, designed to address emotional responses with the steps Name, Understand, Respect, Support, and Explore, was the second most prevalent, appearing in eight articles [20,24,27,34,35,36,37,38]. Other notable models included VitalTalk and Ask-Tell-Ask (ATA), each cited in five articles [22,23,24,27,28,32,35,36,37]. VitalTalk focuses on structured communication for serious illness discussions, while ATA is a technique for clarifying understanding by asking, explaining, and verifying comprehension.
Less frequently cited models included VALUE [24,36,43], a framework for family-centered communication; REMAP (two articles) [20,24], a protocol for care goal discussions; and ADAPT [20], CLASS [20], Serious Illness Conversation Guide (SICG) [22], MR. SPIKES [26], 7-Step Family Conference Framework [40], Hope/Worry Statements [37], and Comskil Model [44] are present as unique models.
These models address diverse aspects of communication, such as prognosis discussions, general communicative strategies, and family conferences. In particular, our analysis revealed that the training focused on the following topics:
- Goals of Care Discussions: It was universally present across all studies, underscoring its critical role in patient-centered care. The discussions often focused on aligning treatment plans with patient preferences and values.
- Breaking Bad News: Reported in 24 out of 26 of the studies [20,21,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44], this theme highlighted the challenges and strategies involved in delivering difficult diagnoses or prognoses. Studies such as Khawand-Azoulai et al. [20], Grant et al. [21], and Nagpal et al. [22] emphasized the importance of sensitivity and clarity in these conversations. Moreover, the prognostication was frequently tied to discussions about disease trajectories and treatment expectations. “Code Status Discussions-Do Not Resuscitate/Intubate (DNR/DNI)” was present in ten studies [25,28,30,32,34,36,37,38,42,43]; these discussions were often framed as part of broader goals of care conversations, in critical or end-of-life scenarios. Seven studies focused on the challenges and strategies for transitioning patients to hospice care, often involving sensitive discussions about prognosis and quality of life [22,29,33,35,38,42,44]. Finally, in five studies [20,33,34,40,43], discontinuing life-sustaining treatments involved ethically and emotionally complex decisions.
- Specific skill training for conducting FMs: A significant majority of studies (23/26) [20,22,23,24,25,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,44,45] addressing preparation for conducting FMs emphasized the value of preparation before difficult conversations (pre-meeting), including reviewing patient history and anticipating family concerns. Furthermore, conflict mediation was identified as a critical skill for resolving disagreements among families or between families and healthcare teams. All studies addressed the necessity of empathy in healthcare communication. Moreover, the importance of active listening is discussed in 22 of the studies [20,22,23,24,25,26,27,28,29,31,32,33,34,35,36,37,39,40,41,42,43,44], with a focus on its role in understanding patient concerns.
3.6. Evaluation of Training
We presented a summary of two principal types of evaluation and outcome: (i) quantitative evaluation tools and outcomes, and (ii) qualitative evaluations and outcomes.
(i)Quantitative evaluation tools and outcomes
Quantitative methodologies are represented in all studies. Likert scale surveys were the most common tool [20,22,24,25,28,29,30,31,32,34,35,36,38,39,41,43,45], followed by Objective Structured Clinical Examinations (OSCEs) [26,29,30,42,45]. Patient/family satisfaction surveys and feedback were used in two studies [22,28]. Three unique tools—Family Meeting Communication Assessment Tool (FaMCAT) [38], JeffSATIC [23], and Mini-CEX [22]—were each used once.
A significant subset adopted mixed-methods approaches [22,23,24,25,29,31,37,43,45], integrating quantitative metrics with qualitative analysis. For instance, Nagpal et al. [22] combined pre/post surveys with thematic analysis of trainee feedback, while Sullivan et al. [31] supplemented quantitative ratings with family member interviews to capture communication preferences. Analysis of quantitative outcomes demonstrated confidence in communication as the predominant measured theme (16/26 studies) [20,21,22,23,24,26,27,28,30,31,33,34,38,40,43,44], primarily assessed via Likert-scale surveys. Communication and behavioral skill measurements represented the second most common outcome [20,21,22,23,27,28,30,32,33,34,37,40,43,44,45], utilizing OSCEs or checklists.
Interprofessional collaboration outcomes were present in six studies [20,21,23,37,39,44].
(ii)Qualitative evaluations and outcomes
Qualitative analysis was conducted in nine studies [22,23,24,25,29,31,37,43,45]. Qualitative evaluation tools were employed to assess various aspects of the interventions, spanning from feedback on used frameworks to interprofessional dialog. The most frequently used method was written feedback (e.g., open-ended survey responses or comments) [22,23,24,29,31,43]. Debrief sessions were the second most common tool [22,29,43,45], followed by thematic analysis of qualitative [23,25,29,37]. Less frequently used methods included semi-structured interviews with participants or family members [31] and focus groups [37].
4. Discussion
Of the 1017 titles screened, we included 26 articles. We discuss some specific findings that emerged from our data, which we believe can guide HPs in designing effective interventions.
A notable observation was the predominance of the North American studies, while no studies were conducted in Europe. The identified training programs appeared to minimize cultural differences; however, training on FMs should be proposed based on cultural specificity, because the goals of care, the values and desires of patients, and the communication of bad news can take on different meanings depending on the culture of belonging. By integrating cultural competence into training curricula, HPs can enhance their capacity to deliver relational support to the family system that respects the unique cultural background of patients, promoting more patient-centered healthcare practices, as suggested by other studies [47,48,49].
The analysis revealed that communication skills training dominated the literature [20,21,22,23,24,25,26,27,28,30,31,33,34,37,38,40,43,44,45]. These studies prioritized competencies such as delivering difficult prognoses, facilitating FMs, and navigating end-of-life discussions. Data suggested that communication on bad news cannot be improvised because the FMs are also a tool for supporting patients and families, not just for giving technical information. Inadequate communication could have negative effects, resulting in psychological distress due to unmet needs, lack of decision-making, and mistrust of HPs [9]. According to the family systems approach, each family member is interdependent on the others to cope with the disease. The different coping strategies of the family system depend on the life cycle stage they are going through: young couples without children; families with small children or teenagers; families with adult children; families with elderly parents. It is therefore essential for HPs to assess the family system they will support [50]. Few of the analyzed studies reported specific training on recognizing family dynamics. Evaluating these topics helps HPs offer personalized care, intercepting families with dysfunctional communication styles so they can work preventively to activate the specialists [15,51]. For example, Kissane et al. proposed a focus on assessing aspects of family-level functioning (e.g., communication, conflict, cohesiveness) that may have been changed by cancer [9]. In general, families with a major sense of coherence, a construct referring to individual family members’ capacity to make sense of the illness and develop a coherent and meaningful narrative about its implications, report less psycho-social distress. Future training on FMs should also consider the most important information about the type of family.
According to clinical practice guidelines [52], FMs should be conducted by a multiprofessional team, including a physician and a nurse or another key figure involved in patient/family care. However, our review reveals that few educational interventions have been designed for teams (physicians and nurses) [21,23,37,39,44]. A smaller but significant subset (n = 5/26) focused on interprofessional training, emphasizing collaborative communication across disciplines. These studies highlighted role clarity and shared decision-making as critical outcomes.
Moreover, among the reviewed studies, the oncology setting was not utilized for FM’s educational interventions. Oncology fellows and radiation oncology residents [26,44] participated in standardized training programs such as Oncotalk and VitalTalk, conducted in specialized communication simulation centers. However, oncologists were not involved in team-based training (physician–nurse) or workplace-integrated learning. Moreover, only three studies [38,40,44] occurred in dedicated palliative care units. These findings suggest training settings remain narrowly focused on acute, institution-bound contexts rather than the diverse environments where palliative communication occurs.
Methodological heterogeneity was evident in sample sizes, training durations, and evaluation frameworks. While quantitative measures predominated, the integration of qualitative data [22,23,24,25,29,31,37,43,45] in select studies enriched interpretations of training acceptability and experiential outcomes. The widespread adoption of simulation-based training underscores its perceived utility in communication education, though variability in assessment rigor suggests the need for standardized evaluation protocols. The limited use of longitudinal follow-up [22,33,35,38,43] highlights opportunities to strengthen causal inferences and assess long-term training impacts in future research.
5. Strengths and Limitations
The limitations of this scoping review should be acknowledged. First, our study was restricted to peer-reviewed articles published in English, Italian, and Spanish, potentially excluding relevant studies in other languages. Only peer-reviewed studies were included. Second, literature via other sources, such as clinical trial registers or pre-print databases, was not searched, so educational interventions described in gray literature may have been missed. Lastly, we observed a scarcity of longitudinal studies, which hinders the ability to assess the long-term impact of FMs’ training on HPs’ practices. Future research should address these gaps by incorporating more diverse cultural contexts and conducting follow-up evaluations to better understand the enduring effects of such training.
6. Implication
We suggest that FMs’ training should be organized in a multidisciplinary approach, using active learning methodologies, such as simulation-based training and role-playing. Moreover, training should consider not only medical students but also the HPs involved in the assistance routine. Finally, a longitudinal evaluation is desirable.
7. Conclusions
We implemented a systematic scoping review to provide a comprehensive overview of FMs’ training programs designed for hospital HPs, and to acquire skills for conducting and/or participating in FMs. The present scoping review defined the extent and pinpointed gaps in training opportunities. This preliminary work is often essential to establish the probably active components of complex educational interventions, the objective of our future study.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Mc Darby M. Mroz E. Walsh L.E. Malling C. Chilov M. Rosa W.E. Kastrinos A. Mc Connell K.M. Parker P.A. Communication Interventions Targeting Both Patients and Clinicians in Oncology: A Systematic Review of Randomized Controlled Trials Psychooncol.202534 e 7010810.1002/pon.70108 PMC 1211844740011205 · doi ↗ · pubmed ↗
- 2Bos-van den Hoek D.W. Visser L.N.C. Brown R.F. Smets E.M.A. Henselmans I. Communication Skills Training for Healthcare Professionals in Oncology over the Past Decade: A Systematic Review of Reviews Curr. Opin. Support. Palliat. Care 201913334510.1097/SPC.000000000000040930562180 · doi ↗ · pubmed ↗
- 3Tanzi S. De Panfilis L. Costantini M. Artioli G. Alquati S. Di Leo S. Development and Preliminary Evaluation of a Communication Skills Training Programme for Hospital Physicians by a Specialized Palliative Care Service: The “Teach to Talk” Programme BMC Med. Educ.20202036310.1186/s 12909-020-02275-233059642 PMC 7560022 · doi ↗ · pubmed ↗
- 4Boyle D.K. Miller P.A. Forbes-Thompson S.A. Communication and End-of-Life Care in the Intensive Care Unit: Patient, Family, and Clinician Outcomes Crit. Care Nurs. Q.20052830231610.1097/00002727-200510000-0000216239819 · doi ↗ · pubmed ↗
- 5Moneymaker K. The Family Conference J. Palliat. Med.2005815710.1089/jpm.2005.8.15715662189 · doi ↗ · pubmed ↗
- 6Powazki R.D. Walsh D. The Family Conference in Palliative Medicine: A Practical Approach Am. J. Hosp. Palliat. Care 20143167868410.1177/104990911349944424031079 · doi ↗ · pubmed ↗
- 7Fineberg I.C. Kawashima M. Asch S.M. Communication with Families Facing Life-Threatening Illness: A Research-Based Model for Family Conferences J. Palliat. Med.20111442142710.1089/jpm.2010.043621385083 · doi ↗ · pubmed ↗
- 8Schuler T.A. Zaider T.I. Li Y. Hichenberg S. Masterson M. Kissane D.W. Typology of Perceived Family Functioning in an American Sample of Patients with Advanced Cancer J. Pain. Symptom Manag.20144828128810.1016/j.jpainsymman.2013.09.013PMC 517744824766739 · doi ↗ · pubmed ↗