Comparing the Effectiveness of Group Discussion and SMS-Based Education on Nutritional Status, Physical Activity, and Blood Cholesterol Levels in Women with Elevated Cholesterol: A Randomized Controlled Trial
Hossein Ashtarian, Neda Yavari, Behrooz Hamzeh, Afshin Almasi

TL;DR
This study compared group discussions and SMS messages to improve nutrition, activity, and cholesterol in women with high cholesterol, finding both effective but group discussions better for nutrition.
Contribution
Demonstrates that group discussions and SMS-based education are equally effective for physical activity and cholesterol, but group discussions improve nutritional status more.
Findings
Both interventions significantly improved nutritional status and physical activity compared to the control group.
Group discussions led to better nutritional status scores than SMS-based education.
No significant difference was found between SMS and discussion groups in physical activity and cholesterol levels.
Abstract
Given the significant contribution of dyslipidemia to cardiovascular disease (CVD) risk in women, effective educational interventions targeting lifestyle modifications are crucial for disease prevention and management. The present study was conducted with the aim of comparing the effectiveness of group discussion and short message service (SMS)-based education in improving nutrition, physical activity, and cholesterol levels in women with high blood cholesterol. A randomized trial was conducted with 165 women aged 30 - 59, recruited from two urban health centers in Kermanshah, Iran. The study included participants with borderline high cholesterol levels (200 - 239 mg/dL) who were randomly assigned to one of three groups (n = 55 each): An SMS-based education group receiving text messages on nutrition and physical activity, a group discussion intervention with facilitated sessions on…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
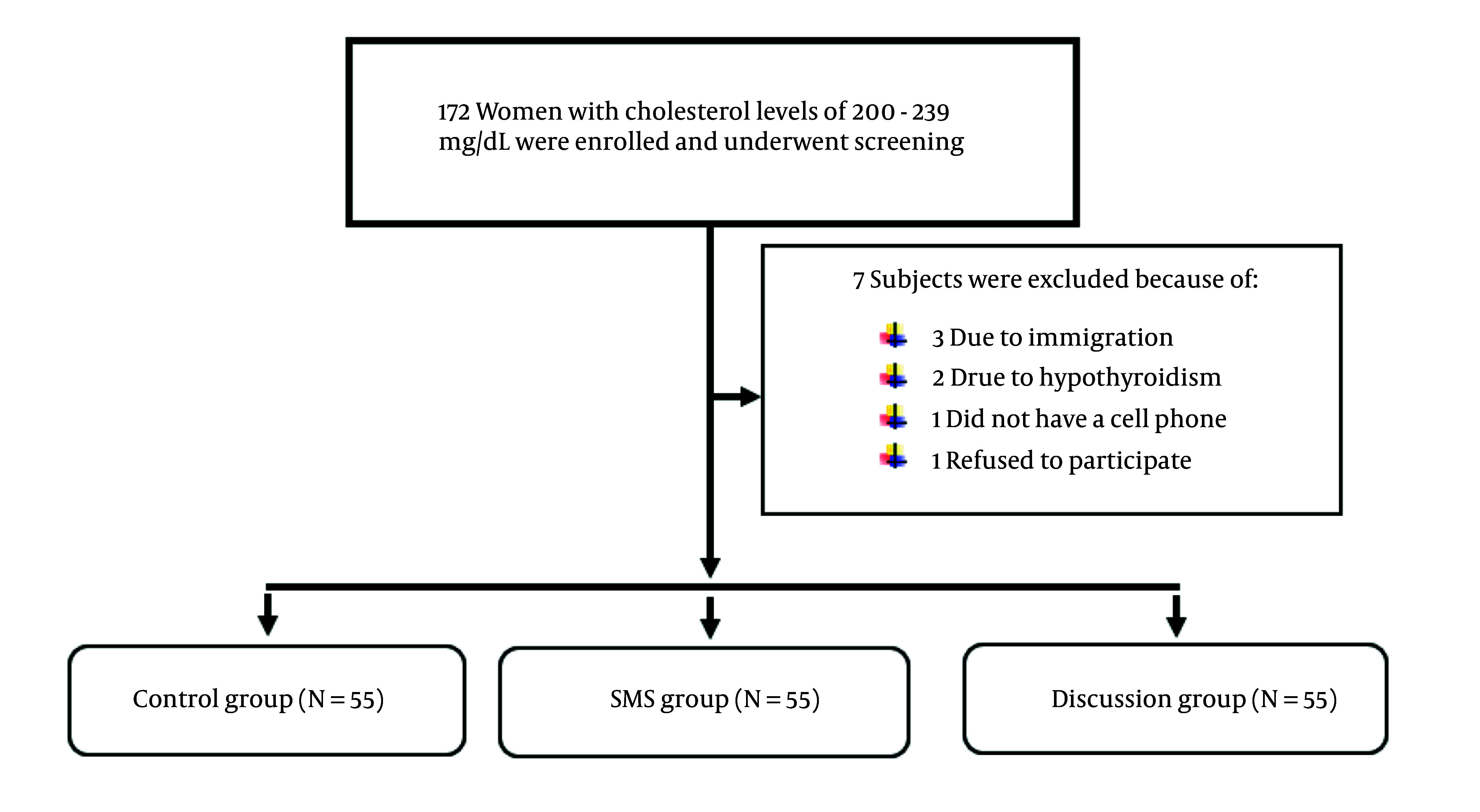 Figure 1
Figure 1| Variables | Control Group | SMS Group | Group Discussion | Total | P-Value |
|---|---|---|---|---|---|
|
| 0.969 | ||||
| 20 - 24.9 | 8 (14.5) | 8 (14.5) | 9 (16.4) | 25 (15.2) | |
| 25 - 29.9 | 28 (50.9) | 26 (47.3) | 24 (43.6) | 78 (47.3) | |
| ≥ 30 | 19 (34.5) | 21 (38.2) | 22 (40) | 62 (37.6) | |
|
| 1 | ||||
| 30 - 39 | 14 (25.5) | 15 (27.3) | 15 (27.3) | 44 (26.7) | |
| 40 - 49 | 16 (29.1) | 16 (29.1) | 16 (29.1) | 48 (29.1) | |
| 50 - 59 | 25 (45.5) | 24 (43.6) | 24 (43.6) | 73 (44.2) | |
|
| 0.813 | ||||
| Elementary | 24 (43.6) | 25 (45.5) | 22 (40) | 71 (43) | |
| Junior high school | 15 (27.3) | 12 (21.8) | 18 (32.7) | 45 (27.3) | |
| Secondary school | 1 (1.8) | 3 (5.5) | 3 (5.5) | 7 (4.2) | |
| Diploma | 15 (27.3) | 15 (27.3) | 12 (21.8) | 42 (25.5) |
| Variables | Groups | |||
|---|---|---|---|---|
| Control (N = 55) | SMS (N = 55) | Group Discussion (N = 55) | Total (N = 165) | |
|
| ||||
| Before | 6.27 ± 1.11 (6) | 5.94 ± 1.26 (6) | 5.72 ± 1.28 (6) | 5.98 ± 1.23 (6) |
| After | 6.12 ± 1.1 (6) | 7.52 ± 1.19 (7) | 8.49 ± 1.05 (9) | 7.38 ± 1.48 (7) |
|
| ||||
| Before | 299 ± 191 (279) | 278 ± 204 (279) | 198 ± 222 (9) | 258 ± 210 (297) |
| After | 275 ± 153 (279) | 339 ± 138 (279) | 306 ± 153 (279) | 307 ± 150 (279) |
|
| ||||
| Before | 216 ± 12 (215) | 215 ± 14 (213) | 217 ± 15 (216) | 216 ± 13 (215) |
| After | 218 ± 12 (218) | 205 ± 14 (201) | 203 ± 14 (200) | 209 ± 15 (206) |
| Variables | Groups | P-Value | ||
|---|---|---|---|---|
| Control | SMS | Group Discussion | ||
|
| ||||
| Before | 299 ± 191 | 278 ± 204 | 198 ± 222 | 0.02 |
| After | 275 ± 153 | 339 ± 138 | 306 ± 153 | 0.097 |
| P-value | 0.041 | < 0.001 | < 0.001 | < 0.05 |
| Difference | -24 ± 90 | 61 ± 121 | 108 ± 141 | |
|
| ||||
| Before | 6.27 ± 1.13 | 5.94 ± 1.26 | 5.72 ± 1.23 | 0.101 |
| After | 6.12 ± 1.10 | 7.52 ± 1.19 | 8.49 ± 1.05 | < 0.001 |
| P-value | 0.262 | < 0.001 | < 0.001 | < 0.001 |
| Difference | -0.14 ± 1.06 | 1.58 ± 0.87 | 2.76 ± 1.07 | |
|
| ||||
| Before | 216 ± 12 | 215 ± 14 | 217 ± 15 | 0. 861 |
| After | 218 ± 12 | 205 ± 14 | 203 ± 14 | < 0.001 |
| P-value | 0.307 | < 0.001 | < 0.001 | < 0.001 |
| Difference | 2 ± 9 | -10 ± 4 | -14 ± 6 | |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMobile Health and mHealth Applications · Physical Activity and Health · Obesity, Physical Activity, Diet
1. Background
Cardiovascular diseases (CVDs) are a primary cause of worldwide morbidity and mortality, and elevated cholesterol levels are recognized as a significant modifiable risk factor in women. Borderline high cholesterol, defined as levels between 200 and 239 mg/dL, presents a critical juncture for intervention to prevent progression to more severe hyperlipidemia and subsequent cardiovascular events (1, 2). Lifestyle modifications, such as dietary adjustments and increased physical activity, constitute the cornerstone of cholesterol management and CVD risk reduction (3). However, effectively translating this knowledge into sustained behavior change, especially among women, remains a significant public health challenge (4, 5).
Traditional health education approaches, such as face-to-face counseling, have demonstrated some limited efficacy in promoting lifestyle changes. In a meta-analysis study examining the effect of behavioral counseling on 15 randomized controlled trials, the results showed that these programs reduced LDL but had no significant effect on HDL and total cholesterol (6). Evidence suggests that different educational intervention methods should be considered to provide appropriate information tailored to the health needs of women with hypercholesterolemia rather than a single educational method that applies to all individuals (7).
2. Objectives
The group discussion method, in particular, offers a valuable platform for peer learning, shared experience, and social support, which can be instrumental in fostering motivation and adherence to new behaviors. However, these approaches can be limited by logistical constraints, including scheduling difficulties, geographical accessibility, and the requirement for participants to travel to designated locations. Moreover, the group setting may not be ideal for all individuals, with some women feeling hesitant to discuss personal health information in a public forum.
On the other hand, the advent of mobile technology has opened new avenues for delivering health interventions, offering the potential to overcome some of the limitations of traditional methods. Mobile interventions, particularly those utilizing text messaging, provide a convenient, cost-effective, and scalable approach to health education and behavior change support. This study seeks to rigorously compare the effectiveness of two distinct intervention modalities — group discussion and short message service (SMS) — in promoting positive changes in diet, physical activity levels, and total cholesterol among women with borderline high cholesterol.
3. Methods
3.1. Study Design and Population
This three-group experimental study (two interventions, one control) investigated middle-aged women (30 - 59) with borderline high cholesterol (200 - 239 mg/dL) at two Kermanshah urban health centers during September 2019. Based on prior research and considering the average changes in cholesterol levels in the three study groups — group 1 (SMS intervention): 22.2 ± 10.89, group 2 (group discussion): 19.2 ± 13.65, and group 3 (control): 16.4 ± 15.4 — with a statistical power of 80% and a confidence level of 95%, the minimum required sample size was calculated to be 55 participants per group using PASS 11 software (8).
The study attempted to mitigate the influence of confounding variables (age, BMI, and literacy) by creating combined variable categories for adjustment across the various groups. The minimization method was employed for random assignment. The two urban health centers with the greatest population reach were used as the source for sample recruitment. Potential participants were identified from the Integrated Health System (SIB), comprising individuals who had undergone fasting blood sugar (FBS) and cholesterol tests for cardiovascular risk assessment. From the initial pool of 172 individuals contacted, 165 participants were ultimately selected for the study after a thorough review of the inclusion and exclusion criteria. Participants were randomly assigned to one of three groups using permuted block randomization [block sizes of (e.g. 6, 9)], with allocation concealment ensured by sealed, opaque envelopes (Figure 1).
Flowchart of screening, randomization, and intervention
To participate in this study, individuals had to be between 30 and 59 years old, own a mobile phone, and be able to read text messages. Participants also needed to have borderline high cholesterol levels, specifically between 200 and 239 mg/dL. Individuals were excluded if they had a history of heart disease, diabetes, high blood pressure, hypothyroidism, or were currently taking cholesterol-lowering medication.
3.2. Data Collection and Questionnaire
A demographic questionnaire was used to collect data on age, height, weight, BMI, education level, mobile phone ownership, underlying disease status, and medication use. Dietary habits were assessed via the Dietary Habits Assessment Questionnaire. This 11-item questionnaire assessed participants’ consumption of dairy products, type of oil used, and intake of vegetables, fruits, and legumes with dichotomous (e.g. yes/no) response options. The validity and reliability of this questionnaire have been confirmed (9).
The short form of the International Physical Activity Questionnaire (IPAQ) contains 7 questions about physical activity in the past seven days. Physical activities were categorized into three levels of intensity: Vigorous, moderate, and light in this study. These categories were determined based on the sum of each activity over a 7-day period. Activities with a sum exceeding 3000 units were classified as vigorous, those ranging from 600 to 3000 units were classified as moderate, and those below 600 units were classified as light. The units are based on the metabolic equivalent (MET) values assigned to different activities in the IPAQ, multiplied by the duration and frequency of the activities. The IPAQ is also a valid questionnaire and its validity and reliability have been confirmed in Iran (10).
Cholesterol levels were measured using the Sinova D280 autoanalyzer (Sinova Medical Device Co., Ltd., China), which is a reliable and accurate instrument that is widely used in clinical laboratories. To ensure the accuracy and precision of the results, blood samples (2 to 3 cc) were taken from the participants after 12 hours of fasting and analyzed under the same laboratory conditions.
After the educational objectives were defined, the educational content for the three sessions was developed. To ensure content validity, the materials were reviewed by three university professors and two nutrition specialists. Based on their feedback, necessary revisions were made to the content. In the SMS intervention group, participants received three text messages per week, delivered between 6:00 - 6:30 pm every week, with the goal of increasing awareness, providing reminders, and offering encouragement. The content of these messages was limited to 160 characters and focused on topics related to hyperlipidemia, diet, and physical activity. To ensure engagement, participants were instructed to send a confirmation reply (e.g. a specific code) upon receiving each message. Messages were derived from American Heart Association (AHA) guidelines and Iranian Ministry of Health protocols, covering hyperlipidemia awareness (e.g. "Limit saturated fats to reduce cholesterol"), nutrition tips (e.g. "Use olive oil instead of animal fats"), and physical activity prompts (e.g. "Aim for 30 min of daily walking").
Participants in the group discussion were assigned to three groups, each containing 15 - 20 individuals. These groups met bi-weekly at 10 am for three educational sessions lasting 45 - 60 minutes. Pamphlets covering the material of each educational session were provided to participants. Following the distribution of the pamphlets, the researcher gave a short presentation summarizing the key information and then facilitated a discussion among the participants. Attendance was recorded for each session, with an average participation rate of around 95%. Sessions followed an interactive, participant-centered approach, including group discussions on personal challenges in managing cholesterol and motivational techniques (e.g. weekly goal-setting).
These three sessions provided a comprehensive overview of blood lipids, covering key aspects from understanding the different types of lipids and their roles in the body to practical strategies for managing them through diet and exercise. The first session introduced dyslipidemia, the various types of fats, their impact on cardiovascular health, and the importance of a balanced diet as represented by the food pyramid. The second session delved into the specifics of nutrition for individuals with high blood lipids, outlining foods to include and avoid, and explaining how elevated lipid levels affect the heart and blood vessels, increasing the risk of CVDs. Finally, the third session emphasized the crucial role of physical activity in managing blood lipids, detailing how regular exercise can lower levels and improve cardiovascular health, while also providing guidance on choosing appropriate types, intensity, and duration of physical activity. In this study, following data collection, the control group was given an educational booklet comprising the instructed content.
3.3. Ethical Considerations
The present study was approved by the Ethics Committee of Kermanshah University of Medical Sciences (IR.KUMS.REC.1397.576). All relevant ethical considerations were observed. The trial was registered at the Iranian Registry of Clinical Trials (IRCT20130812014333N114).
3.4. Data Analysis
The data were entered into SPSS version 16, and descriptive and analytical analyses were performed. After checking the normality of the data, the Kruskal-Wallis, chi-square, and Wilcoxon tests were used, and the significance level was considered to be less than 5%.
4. Results
In the present study, 165 women aged 30 - 59 with cholesterol levels of 200 - 239 mg/dL participated. Descriptive information, including BMI, age, and education level in all three groups, is given in detail in Table 1.
The results of the chi-square test showed that there was no significant difference between the three study groups in terms of BMI (P = 0.969), age (P > 0.05), and education level (P = 0.813). Given the non-normal distribution of pre-intervention nutritional status and cholesterol levels across the three groups, the Kruskal-Wallis test was employed for comparative analysis. The three groups exhibited no statistically significant differences in either nutritional status (P = 0.101) or cholesterol levels (P = 0.861) before the commencement of the intervention. Since baseline physical activity levels differed significantly among the three groups (Kruskal-Wallis test, P = 0.02) and were non-normally distributed, absolute changes in physical activity were calculated to assess the intervention’s effect. The results of the Kruskal-Wallis test showed that this difference between the three groups was significant (P < 0.05). Pairwise comparisons revealed that changes in physical activity scores, assessed by energy expenditure, were significantly greater in both the SMS (P = 0.002) and group discussion (P < 0.001) interventions compared to the control group. However, no significant difference in physical activity was observed between the SMS and group discussion interventions (P = 0.24) (Table 2).
The data presented in Table 3 indicate that both group discussions and SMS interventions yielded statistically significant improvements in physical activity levels relative to the control group (P < 0.001). While nutritional status showed greater enhancement through group discussions (P < 0.001), cholesterol reduction was equally effective across both intervention modalities, with no significant difference between them.
5. Discussion
This study compared the effects of group discussion and SMS interventions on nutritional status, physical activity, and blood cholesterol levels in women with high cholesterol. The results showed that both educational approaches led to significant improvements, suggesting their value in post-screening health programs. These findings are particularly noteworthy because group discussions demonstrated more effectiveness than SMS in improving dietary habits, likely due to their interactive nature, which allows for experience-sharing and immediate feedback (11). Further research is needed to explore the underlying mechanisms through which group discussions lead to greater improvements in nutritional status.
The findings of the present study align with prior research demonstrating the effectiveness of different educational approaches in improving health outcomes. For instance, a comparative study on diabetes self-care revealed that both group-based education and mobile-based education were equally effective, with no significant difference between the two methods (12). While group discussions showed advantages in dietary improvements, the role of SMS-based interventions deserves particular attention, given their scalability and documented efficacy in health promotion. Multiple studies have shown that regular text messaging significantly improves both nutritional practices and physical activity levels among various populations, from hypertensive patients to women visiting health centers, with measurable differences between intervention and control groups (13-17).
Emerging evidence suggests that mobile-delivered education can achieve superior outcomes for certain health behaviors. For instance, one study found that mobile phone-delivered education significantly improved both dietary compliance and overall treatment adherence among hemodialysis patients, whereas face-to-face education, while improving general treatment adherence, showed no significant effect on dietary restrictions specifically (17). However, while studies highlight the potential advantages of mobile-based education, several limitations warrant consideration. Although the use of SMS is recognized as an educational method, its limitations underscore the necessity of leveraging additional mobile phone functionalities, such as interactive games or specialized applications, to enhance the effectiveness and engagement of the educational process.
A comprehensive systematic review and meta-analysis investigated the impact of utilizing mobile applications, both with and without game-based elements, to assess their effectiveness and outcomes. Findings from 36 research studies demonstrated that mobile applications incorporating game-like elements were effective in promoting higher levels of physical activity and contributing to weight loss (18). However, it is important to note that some studies have also shown that digital interventions, including these gamified apps, tend to be more beneficial for men than for women, highlighting potential gender-based differences in engagement and outcomes (19). In contrast, the results of the current study revealed that SMS-based interventions were effective in reducing blood cholesterol levels among women, suggesting that simpler, non-gamified digital approaches may be more suitable for certain demographics.
The present study documented a statistically significant reduction in cholesterol levels following the group discussion and mobile-based educational interventions. A potential reason for the observed reduction in cholesterol levels among women in this study may be attributed to the simultaneous increase in physical activity resulting from the educational content provided during the course of the intervention. Numerous studies have demonstrated the positive impact of increased physical activity on reducing blood cholesterol levels, which is consistent with the findings of the current study (20, 21).
Notably, while the observed 10 - 13 mg/dL reduction in total cholesterol among participants appears modest, its clinical significance becomes evident when considering longitudinal epidemiological evidence. For instance, data from the Framingham study indicate that even a 10 mg/dL decrease in cholesterol is associated with a 2% reduction in CVD risk (22). Furthermore, non-pharmacological interventions typically lower cholesterol by 5 - 20 mg/dL (23). These results demonstrate that even moderate improvements in cardiovascular risk factors can generate significant population-level health benefits when implemented widely. This evidence highlights the preventive medicine value of non-pharmacological approaches to cholesterol management.
Despite efforts to control for confounding variables through rigorous inclusion/exclusion criteria (e.g. age range, health status) and randomization across three study groups, several limitations persist. First, unmeasured confounders such as genetic predispositions, dietary habits outside the intervention, and participants’ adherence to SMS instructions may have influenced outcomes. Second, factors beyond the researcher’s control — including environmental stressors, access to healthcare, or concurrent medications — could not be fully mitigated. While randomization helped balance known and unknown confounders across groups, residual confounding may remain. Future studies could address these limitations by collecting detailed baseline covariates or employing stratified randomization.
5.1. Conclusions
The findings of this study highlight the critical role of targeted education in empowering women with high cholesterol to adopt healthier lifestyle practices. The results showed that both educational intervention methods improved nutritional status, physical activity, and reduced cholesterol levels, but this effectiveness was more evident in the group discussion training method, which could be due to various reasons. Therefore, both training methods can be used alone or in combination with the two methods in middle-aged women with high cholesterol. The group discussion training method can lead to better learning in these people due to the creation of active learning, and also the use of short messages as a low-cost and immediate method can be used alongside the group discussion method as a reminder method.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Peters SA Singhateh Y Mackay D Huxley RR Woodward M Total cholesterol as a risk factor for coronary heart disease and stroke in women compared with men: A systematic review and meta-analysis.Atherosclerosis.20162481233110.1016/j.atherosclerosis.2016.03.01627016614 · doi ↗ · pubmed ↗
- 2Wenger NK Female-friendly focus: 2019 ACC/AHA Guideline on the Primary Prevention of Cardiovascular Disease.Clin Cardiol.2019428706910.1002/clc.2321831211428 PMC 6671777 · doi ↗ · pubmed ↗
- 3Katz DL Karlsen MC Chung M Shams-White MM Green LW Fielding Jet al.Hierarchies of evidence applied to lifestyle Medicine (HEALM): introduction of a strength-of-evidence approach based on a methodological systematic review.BMC Med Res Methodol.201919117810.1186/s 12874-019-0811-z 31429718 PMC 6701153 · doi ↗ · pubmed ↗
- 4Martemucci G Khalil M Di Luca A Abdallah HD'Alessandro AG Comprehensive Strategies for Metabolic Syndrome: How Nutrition, Dietary Polyphenols, Physical Activity, and Lifestyle Modifications Address Diabesity, Cardiovascular Diseases, and Neurodegenerative Conditions.Metabolites.202414632710.3390/metabo 1406032738921462 PMC 11206163 · doi ↗ · pubmed ↗
- 5Giles LA Hyperlipidemia Prevention and Management Utilizing Lifestyle Changes.J Midwifery Womens Health.2024693361910.1111/jmwh.1363738678434 · doi ↗ · pubmed ↗
- 6Albert SL Massar RE Correa L Kwok L Joshi S Shah Set al.Change in cardiometabolic risk factors in a pilot safety-net plant-based lifestyle medicine program.Front Nutr.202310115581710.3389/fnut.2023.115581737153909 PMC 10157493 · doi ↗ · pubmed ↗
- 7Seo M Jun EY Oh H Development and effectiveness of a mobile-based autonomy support program for the prevention of metabolic syndrome in middle-aged women.Front Public Health.202412133498810.3389/fpubh.2024.133498838384883 PMC 10879428 · doi ↗ · pubmed ↗
- 8Jafari M Pasdar Y Rezaei M Mahdizadeh H Ashtarian H[The effect of nutrition education using blogs, group-collaborative blogs and short messaging on lipids profiles and glucose in patients with type II diabetes]. Med J Mashhad Univ Med Sci.20135652616