Mode of delivery among pregnant people with obesity undergoing labor induction in the late preterm period
Daniella Rogerson, Minhazur Sarker, Alice Sutton, E. Nicole Teal, Cynthia Gyamfi-Bannerman

TL;DR
Pregnant people with obesity are more likely to have cesarean delivery during late preterm labor induction, but most still deliver vaginally.
Contribution
This study is the first to examine cesarean delivery rates during late preterm induction of labor specifically among people with obesity.
Findings
Participants with obesity had higher cesarean delivery rates compared to nonobese participants.
Adjusted odds of cesarean delivery increased with higher BMI classes.
Despite higher cesarean rates, most obese participants still delivered vaginally.
Abstract
Pregnant people with obesity are more likely than those without obesity to undergo induction of labor and to require unplanned cesarean delivery during induction at term. Whether they are more likely to undergo unplanned cesarean delivery during preterm induction of labor is unknown. This study examines the induction of labor success among people with obesity undergoing indicated late preterm induction of labor. This is a secondary analysis of a multicenter, randomized trial of betamethasone versus placebo among pregnancies at risk for late preterm delivery, defined as delivery between 34 weeks and 0 days and 36 weeks and 6 days between 2010 and 2015. This study included pregnant people with live singleton nonanomalous gestations at high risk for late preterm delivery before 36 weeks and 6 days. This secondary analysis included all participants who underwent a medically indicated…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
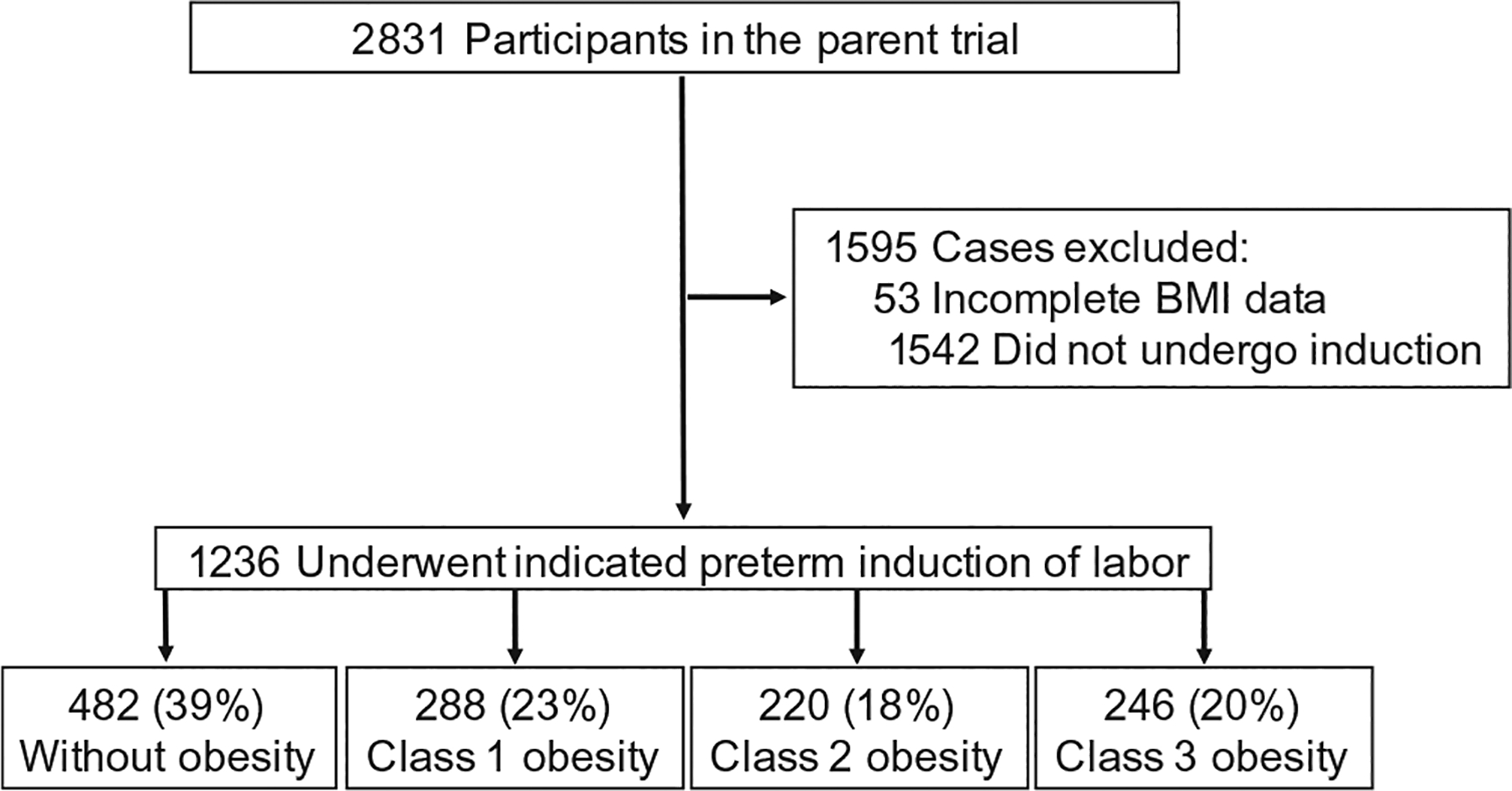 Figure 1
Figure 1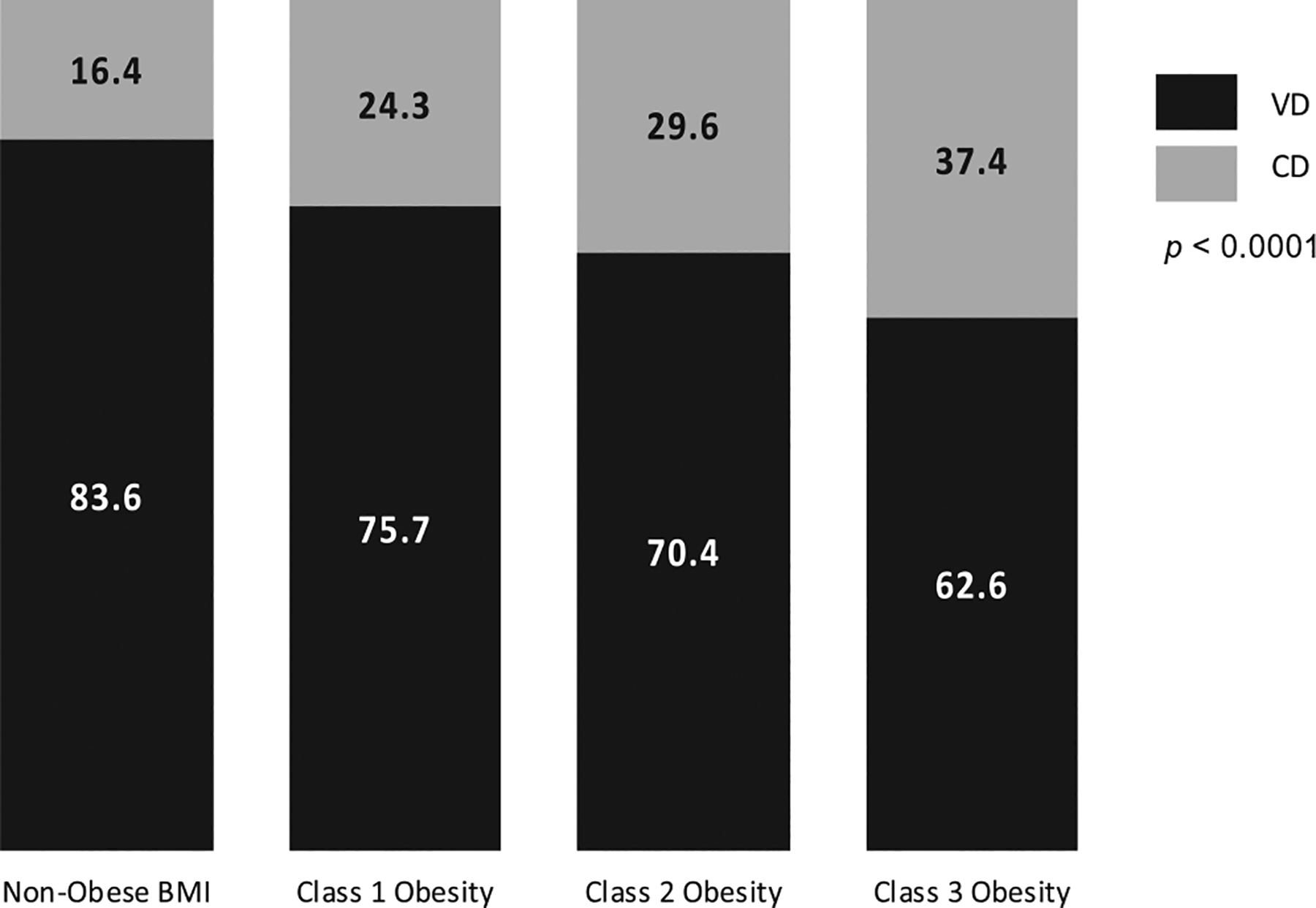 Figure 2
Figure 2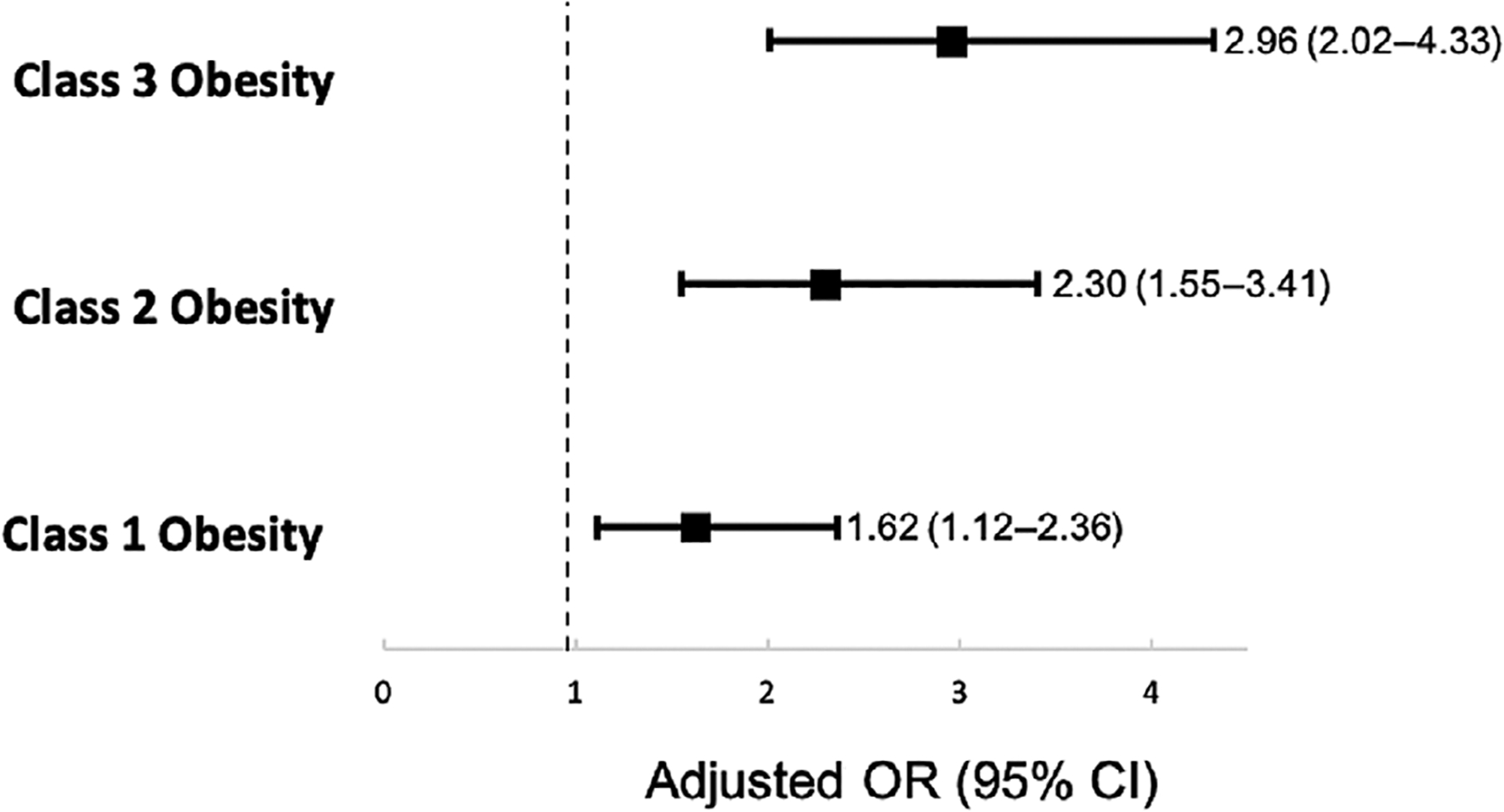 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPregnancy-related medical research · Maternal and Perinatal Health Interventions · Gestational Diabetes Research and Management
INTRODUCTION
1 |
The prevalence of obesity (class 1 obesity—body mass index [BMI] 30–34.9, class 2 obesity—BMI 35–39.9, and class 3 obesity—BMI ≥ 40) among reproductive-aged people in the United States is 31%, and half of these people are class 2 or 3 obese [1]. Pregnant people with obesity are at increased risk for a number of pregnancy complications, including gestational diabetes mellitus (GDM), gestational hypertension (HTN), preeclampsia, large for gestational age newborns, stillbirth, and postpartum hemorrhage [1, 2]. People with obesity are also more likely to be recommended induction of labor (IOL) due to medical comorbidities [3, 4]. One study found that the rate of IOL increases with obesity class, with 30.4% for class 1, 32.5% for class 2, and 34% for class 3 and above compared to 28% among people without obesity [5].
People with obesity have been shown to have prolonged latent and active phases in labor compared to those without obesity, and are at increased risk of cesarean delivery, including during IOL [1, 6–11]. Even when implementing standardized failed IOL criteria, studies have shown an increased risk of cesarean among people with obesity [5, 10]. Notably, prior studies have focused only on term pregnancies; data examining mode of delivery after preterm IOL, when delivery is almost always indicated and necessary, are sparse.
Whether people with obesity undergoing medically indicated late preterm IOL are at higher risk of cesarean than their counterparts without obesity is unknown. This study evaluates cesarean rates for patients undergoing medically indicated preterm IOL stratified by BMI category. We hypothesized that during late preterm medically indicated IOL, participants with obesity will have higher cesarean delivery rates than those without obesity.
MATERIALS AND METHODS
2 |
This is a secondary analysis of a multicenter, randomized trial of betamethasone versus placebo among pregnancies at risk for late preterm delivery, defined as delivery between 34 weeks and 0 days and 36 weeks and 6 days [12]. The parent trial, Antenatal Betamethasone for Women at Risk for Late Preterm Delivery (ALPS), was conducted at 17 university-based clinical centers within the Maternal–Fetal Medicine Units Network of the Eunice Kennedy Shriver National Institute of Child Health and Human Development between 2010 and 2015. The parent trial included pregnant people with live, singleton, nonanomalous gestations at high risk for late preterm delivery due to labor or need for medically indicated delivery [12]. In the parent study, participants were included if an IOL was expected to start by 36 weeks 5 days, and among the exclusion criteria were unclear dating, having pregestational diabetes, or an expected delivery within 12 h.
For this secondary analysis, we included all participants in the parent trial who underwent a medically indicated preterm IOL. We excluded patients who underwent planned cesarean, had spontaneous labor, had a BMI <18.5 at their most recent measured weight prior to delivery, or had incomplete BMI data. We compared cesarean delivery rates among participants undergoing preterm IOL stratified by BMI class: no obesity (BMI 18.5–29.9), class 1 obesity (BMI 30–34.9), class 2 obesity (BMI 35–39.9), and class 3 obesity (BMI ≥ 40). BMI was calculated using the last measured weight prior to delivery. The primary outcome was cesarean birth. The indications for IOL and cesarean delivery were reviewed; one or multiple indications for both induction and cesarean were listed for each case.
Chi-square was used for categorical data reported as frequencies and percentages; ANOVA or Wilcoxon was used for continuous variables reported as means with standard deviation (SD) or median with interquartile range (IQR), as appropriate. We fit multivariable regression models to determine the strength of association after adjusting for confounders identified in the literature and statistically significant baseline differences, including nulliparity, maternal age, chronic HTN (cHTN), GDM, and treatment group. A p value of less than 0.05 or a 95% confidence interval (CI) not crossing 1.0 was considered statistically significant. All statistical analyses were performed on SAS statistical software (Version 9.4).
The parent trial research protocol was approved by the Institutional Review Board of each clinical trial site. All patients in the parent trial provided voluntary written informed consent prior to study participation. Given the de-identified data, this secondary analysis was deemed exempt and did not require separate oversight from our Institution Review Board.
RESULTS
3 |
Among the 2831 participants in the parent trial, 1236 participants underwent medically indicated late preterm IOL, with 482 (39%) without obesity, 288 (23%) with class 1 obesity, 220 (18%) with class 2 obesity, and 246 (20%) with class 3 obesity (Figure 1). Baseline demographics for the cohort are presented in Table 1. Multiple indications for induction were cited for each case, most commonly including preeclampsia and/or hypertension (688), premature rupture of membranes (254), fetal growth restriction (114), oligohydramnios (101), and nonreassuring fetal status (70). Other indications included cholestasis (40), other maternal disease (34), abruption (20), GDM (10), history of fetal demise/other serious pregnancy complication (7), chorioamnionitis (2), and other causes not described in the parent trial (44). The median gestational age at delivery for each group was 36 weeks (IQR 35, 37) and was statistically similar. Participants with class 1–3 obesity were more likely to be Black (20% with no obesity; 27%, 29%, and 37% with class 1–3 obesity, respectively), have cHTN (6% with no obesity; 13%, 21%, and 33% with class 1–3 obesity, respectively), or GDM (6% with no obesity; 13%, 18%, and 21% class 1–3 obesity, respectively) than their counterparts without obesity (all p < 0.0001). There were no differences in maternal age, insurance type, nulliparity, ethnicity, or tobacco use between groups. Neonates of participants with class 3 and class 4 obesity weighed more than the neonates of their normal weight counterparts (p < 0.0001). The incidence of low 5-min APGAR scores (defined as 5-min APGAR < 7) was not different between the groups (0.230).
Overall, 930 (75%) participants achieved a vaginal birth, while 306 (25%) participants underwent cesarean delivery. Among the obese participants, the overall vaginal delivery rate was 69.9% (527/754). In a univariable analysis, as BMI class increased, participants were more likely to undergo unplanned cesarean delivery, 79 (16.4%) with no obesity, 70 (24.3%) with class 1, 65 (29.6%) class 2, and 92 (37.4%) class 3 obesity (p < 0.0001). However, the majority of participants in each group had a vaginal birth, 83.6% among the no obesity group, 75.7 % among class 1 obesity, 70.4% among class 2 obesity, and 62.6% among class 3 obesity (Figure 2). Although multiple indications for cesarean were listed for each participant, the most common indications included nonreassuring fetal status (154, 50%) and labor dystocia (149, 49%). Other indications included preeclampsia and/or hypertension (59), malpresentation (15), chorioamnionitis (6), abruption (5), cord prolapse (4), other (2), prior cesarean (2), other maternal disease (1), and elective (1).
In a multivariable analysis adjusting for nulliparity, advanced maternal age, cHTN, GDM, and treatment group and using participants with no obesity as the reference, participants with class 1–3 obesity were more likely to undergo unplanned cesarean delivery (class 1, aOR 1.62, 95% CI 1.12–2.36; class 2, aOR 2.30, 95% CI 1.55–3.41; and class 3, aOR 2.96, 95% CI 2.02–4.33, Figure 3).
DISCUSSION
4 |
Our study found that pregnant people with obesity undergoing medically indicated late preterm IOL are at increased risk for unplanned cesarean with increasing BMI category compared to people without obesity, even after adjusting for confounders such as GDM, cHTN, and parity. Cesareans were largely performed for nonreassuring fetal status, highlighting fetal intolerance, and labor dystocia, highlighting parturition differences in people with obesity. However, the majority of participants (69.9%, 527/754) with obesity achieved a vaginal birth regardless of their BMI class, suggesting that when delivery is indicated, a vaginal trial of labor can be offered in the appropriate clinical context.
Our findings of increased cesareans among people with obesity undergoing preterm IOL are consistent with the existing literature for term IOL, where a similar association between BMI class and cesarean is appreciated [5, 11]. One large population-based cohort study of singleton pregnancies found that rates of failed IOL and subsequent cesarean increased with BMI from 13% in people without obesity to 20.2%, 24.2%, and 29% in class 1–3 obesity, respectively [5]. A systematic review found increased odds of cesarean with increasing BMI; this review largely included studies that examined only patients at term as well as a few small studies that included both preterm and term births [11]. Our findings add to the literature by highlighting that this increased risk of failed IOL persists in the late preterm period, even though birth weights are smaller relative to term neonates.
Given that the majority of participants achieved a vaginal birth, IOL can be offered as the primary recommendation for patients with obesity who require late preterm delivery. Planned cesarean has not been shown to improve obstetrical outcomes in people with obesity, and the risk of cesarean may persist for pregnant patients with obesity after expectant management, as obesity is a risk factor for cesarean during spontaneous labor as well [13–15]. Though the majority of participants with obesity delivered vaginally, the increased risk of cesarean was notable. Cesarean delivery is associated with increased rates of hemorrhage, transfusion, venous thromboembolism, placental abnormalities in future pregnancies, and overall morbidity [9]. These risks associated with cesarean highlight the importance of optimizing preconception weight and weight gain during pregnancy.
Given the association between maternal obesity and labor dystocia noted in our cohort and at term, a number of studies have examined IOL techniques for people with obesity to identify whether there are benefits to any specific method. No benefits to any one agent, and no specific recommendations for IOL regimens in people with obesity, are currently available [16–18]. Given that 49% of the cesareans in our cohort occurred due to labor dystocia, and a breadth of literature notes prolonged labor curves for people with obesity [7, 8], further studies examining the optimal approach to IOL, and criteria for failure, in people with obesity are needed. Patients may also benefit from being counseled that obesity is a modifiable risk factor for risk of cesarean at the preconception visit.
Limitations for this study include that granular data on failed induction versus labor dystocia were not available, multiple indications were listed for cesareans, and we are unable to comment on some pertinent parameters related to induction, including the starting Bishop score, whether patients were undergoing trial of labor after cesarean, and the specific methods used for IOL. However, the fact that the parent trial allowed pragmatic management at the discretion of the provider makes the findings more generalizable. Other strengths included that, as an analysis from a prospective randomized controlled trial, the data are robust. The large cohort of participants received care at geographically diverse academic medical centers, also increasing the generalizability of our findings. Finally, we used data on maternal BMI at the time of delivery instead of prepregnancy BMI, as this is more pertinent to counseling at the time of delivery.
CONCLUSIONS
5 |
While obesity and obesity class were associated with higher rates of cesarean compared with pregnant individuals without obesity, the majority (69.9%, 527/754) of pregnant people with obesity undergoing late preterm IOL delivered vaginally, and thus obesity should not necessarily deter providers from offering IOL when there are no obstetric contraindications. Given increasing rates of obesity among people of reproductive age, further studies are needed to understand differences in labor and induction physiology among pregnant people with obesity.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Poston L, Caleyachetty R, Cnattingius S, Corvalán C, Uauy R, Herring S, and Gillman MW, 2016. “Preconceptional and Maternal Obesity: Epidemiology and Health Consequences.” The Lancet Diabetes & Endocrinology 4(12): 1025–36.27743975 10.1016/S 2213-8587(16)30217-0 · doi ↗ · pubmed ↗
- 2Vats H, Saxena R, Sachdeva MP, Walia GK, and Gupta V. 2021. “Impact of Maternal Pre-pregnancy Body Mass Index on Maternal, Fetal and Neonatal Adverse Outcomes in the World-wide Populations: A Systematic Review and Meta-analysis.” Obesity Research & Clinical Practice 15(6): 536–45.34782256 10.1016/j.orcp.2021.10.005 · doi ↗ · pubmed ↗
- 3Usha Kiran TS, Hemmadi S, Bethel J, and Evans J. 2005. “Outcome of Pregnancy in a Woman With an Increased Body Mass Index.” BJOG: An International Journal of Obstetrics and Gynaecology 112(6): 768–72.15924535 10.1111/j.1471-0528.2004.00546.x · doi ↗ · pubmed ↗
- 4Sebire NJ, Jolly M, Harris JP, Wadsworth J, Joffe M, Beard RW, Regan L, and Robinson S, 2001. “Maternal Obesity and Pregnancy Outcome: A Study of 287,213 Pregnancies in London.” International Journal of Obesity and Related Metabolic Disorders 25(8): 1175–82.11477502 10.1038/sj.ijo.0801670 · doi ↗ · pubmed ↗
- 5Wolfe KB, Rossi RA, and Warshak CR. 2011. “The Effect of Maternal Obesity on the Rate of Failed Induction of Labor.” American Journal of Obstetrics and Gynecology 205(2): 128.e 1–e 7.
- 6Norman SM, Tuuli MG, Odibo AO, Caughey AB, Roehl KA, and Cahill AG. 2012. “The Effects of Obesity on the First Stage of Labor.” Obstetrics and Gynecology 120(1): 130–5.22914401 10.1097/AOG.0b 013e 318259589 c PMC 4494673 · doi ↗ · pubmed ↗
- 7Cohen WR and Friedman EA. 2023. “The Latent Phase of Labor.” American Journal of Obstetrics and Gynecology 228(5S): S 1017–S 24.36973092 10.1016/j.ajog.2022.04.029 · doi ↗ · pubmed ↗
- 8Frolova AI, Raghuraman N, Stout MJ, Tuuli MG, Macones GA, and Cahill AG. 2021. “Obesity, Second Stage Duration, and Labor Outcomes in Nulliparous Women.” American Journal of Perinatology 38(4): 342–9.31563134 10.1055/s-0039-1697586 PMC 8081034 · doi ↗ · pubmed ↗