Real-World Effectiveness of Cisplatin, 5-Fluorouracil, and Pembrolizumab Combination Therapy for Unresectable or Recurrent Esophageal Cancer
Yu Ueta, Masanobu Nakajima, Masaki Yoshimatsu, Takahiro Ochiai, Shuhei Takise, Junki Fujita, Masatoshi Nakagawa, Shinji Morita, Kazuyuki Kojima

TL;DR
This study shows that reducing the dose of chemotherapy in combination with pembrolizumab for esophageal cancer does not harm effectiveness and reduces side effects.
Contribution
The study demonstrates that dose reduction of chemotherapy in combination with pembrolizumab is safe and effective in real-world clinical settings.
Findings
Dose reduction did not compromise treatment effectiveness with overall response and disease control rates of 55.6% and 81.5%.
Grade ≥ 3 adverse events occurred in 16.7% of patients, with fewer events in the dose-reduction group.
Median overall survival was 18.6 months and progression-free survival was 6.5 months, with no significant differences based on dose reduction.
Abstract
Esophageal cancer is one of the most aggressive cancers worldwide, and many patients are diagnosed at an advanced stage where surgery is not possible. A combination of cisplatin, 5-fluorouracil, and pembrolizumab has recently become a standard first-line treatment for unresectable or recurrent esophageal cancer, but many patients in real-world practice are elderly or have impaired renal function, which makes full-dose chemotherapy difficult to tolerate. In this study, we evaluated the outcomes of patients treated with this combination therapy at our institution, with particular attention to those who started treatment with reduced doses. We found that dose reduction did not compromise the effectiveness of treatment and was associated with fewer severe side effects, allowing patients to continue therapy for longer periods. These findings suggest that careful dose adjustment may help…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
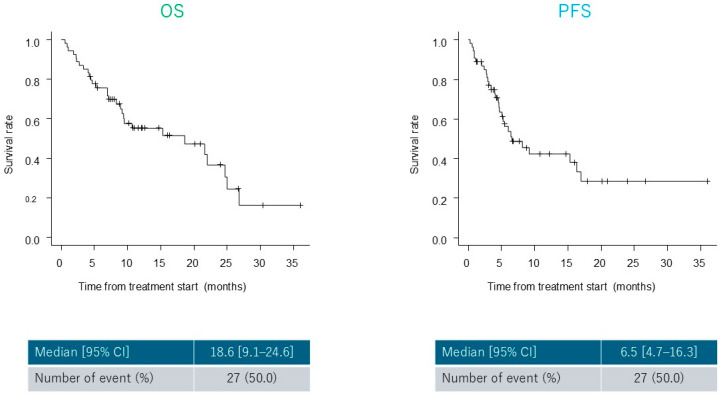 Figure 1
Figure 1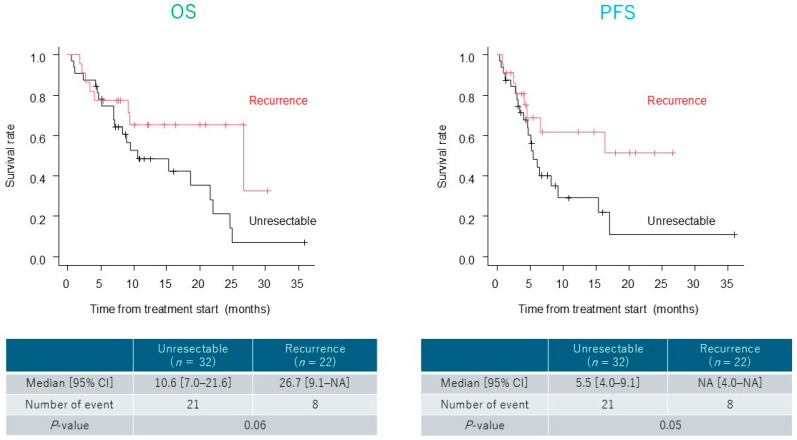 Figure 2
Figure 2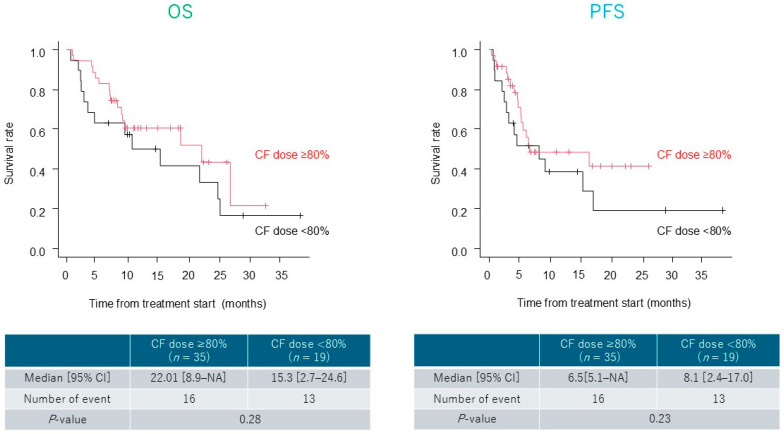 Figure 3
Figure 3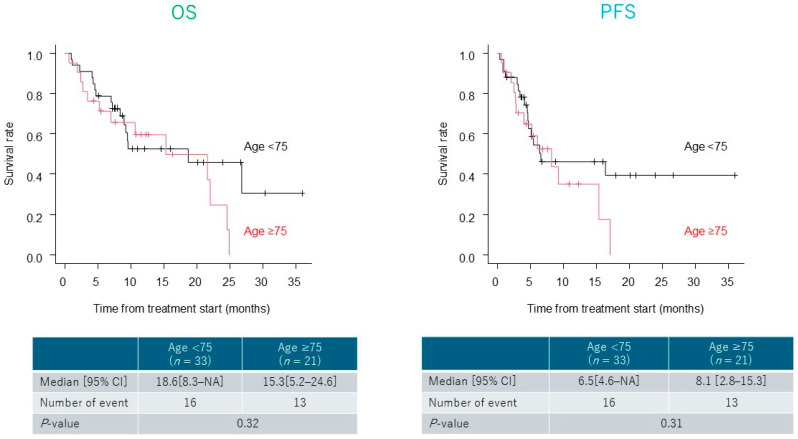 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEsophageal Cancer Research and Treatment · Cancer Immunotherapy and Biomarkers · Gastric Cancer Management and Outcomes
1. Introduction
Esophageal cancer is one of the most lethal gastrointestinal malignancies worldwide. The GLOBOCAN 2022 data indicated approximately 511,054 new cases and 445,391 deaths, making it the seventh leading cause of cancer-related mortality [1]. In Japan, approximately 24,000 new cases of esophageal cancer are reported annually, and this number is projected to increase further [2]. Patients tend to be diagnosed at advanced stages (III or IV), which significantly limits the possibility of curative treatment [3]. Cisplatin and 5-fluorouracil (CF) therapy has been the standard first-line treatment for unresectable or recurrent esophageal cancer, with reported response rates of approximately 30% and median overall survival (OS) ranging from 6.6 to 9.5 months [4,5,6,7,8,9]. Immune checkpoint inhibitors (ICIs) are now internationally recognized as a new standard of care in various malignancies including esophageal cancer owing to their superior efficacy [10,11,12,13]. The KEYNOTE-590 trial compared cisplatin, 5-fluorouracil (CF), and pembrolizumab (Pem) (CF plus Pem) with CF plus placebo. The addition of Pem significantly prolongs OS and progression-free survival (PFS), establishing CF plus Pem therapy as the global standard [13]. However, in clinical practice, CF regimens often require dose reduction in patients with advanced age, renal dysfunction, or poor performance status. Despite their common occurrence, the effects of these modifications on the treatment outcomes have not been sufficiently studied. This is particularly relevant in real-world settings where patients are often older and present with multiple comorbidities. This retrospective study aimed to evaluate the effect of dose modifications based on age and renal function on the efficacy and safety of combined CF and Pem therapy. We focused on the OS, PFS, response rates, and adverse events in patients with unresectable or recurrent esophageal cancer.
2. Materials and Methods
2.1. Study Design and Patients
In our institution, the treatment strategy is determined according to disease stage and resectability. For patients with Stage IVA disease, surgery aiming for R0 resection is performed when resection is feasible, such as in T4a cases with invasion to the lung or pleura. For unresectable disease, including T4b cases with invasion to the aorta, trachea, or bronchi, definitive chemoradiotherapy (CRT) is indicated. In patients with extensive lymph node metastases (N3), systemic therapy with ICI plus chemotherapy is administered. For Stage IVB disease, the principle of treatment is systemic therapy, with ICI plus chemotherapy being the standard approach. In addition, palliative treatments are considered when appropriate; for example, in cases of dysphagia, palliative radiotherapy (RT) or esophageal stent placement may be employed. For recurrent disease, when local therapy is feasible, chemotherapy is combined with surgery or radiotherapy, whereas when local therapy is not feasible, systemic therapy with ICI plus chemotherapy is selected.
This retrospective observational study was conducted at a single institution. We included patients with unresectable or recurrent esophageal cancer who received CF plus Pem therapy between February 2022 and February 2025. Patients with incomplete clinical data and those with a short observation period were excluded from this study. Patients with comorbidities who were able to continue treatment were included. The inclusion criteria were (i) histologically confirmed unresectable or recurrent esophageal cancer, and (ii) availability of sufficient clinical and follow-up data. The exclusion criteria were as follows: (i) patients with incomplete or missing clinical data, and (ii) patients with a short observation period.
This study was conducted in accordance with the principles of the Declaration of Helsinki and was approved by the Medical Ethics Committee of Dokkyo Medical University (approval number: R-96-1J). Written informed consent for treatment was obtained from all patients. For the use of clinical data, the requirement for additional individual consent was waived owing to the retrospective design, with an opt-out option available on the institutional website.
2.2. Data Collection Items
Clinical data were extracted from electronic medical records and imaging studies. Variables included age, sex, Eastern Cooperative Oncology Group performance status (PS), combined positive score (CPS) of programmed death-ligand 1 (PD-L1), estimated glomerular filtration rate (eGFR), and comorbidities. Tumor characteristics, including location, histological type, macroscopic appearance, clinical stage, and metastasis, were classified according to the Union for International Cancer Control (UICC) tumor, node, and metastasis (TNM) classification (8th edition). For patients with recurrence (n = 22), the T, N, M, and stage classifications refer to the clinical stage before the initial therapy, not at the time of recurrence.
The treatment-related data included the number of cycles, initial CF dose (percentage of the standard dose), reasons for dose reduction, and post-treatment course. Treatment response was assessed using the Response Evaluation Criteria in Solid Tumors (RECIST 1.1): complete response (CR), partial response (PR), stable disease (SD), or progressive disease (PD). Esophagogastroduodenoscopic (EGD) findings were reviewed. Safety was evaluated according to the Common Terminology Criteria for Adverse Events (CTCAE, version 5.0), including the incidence and grade of immune-related adverse events (irAEs).
2.3. Treatment Protocol
The standard regimen consisted of cisplatin (80 mg/m^2^ on day 1), 5-fluorouracil (800 mg/m^2^ on days 1–5), and Pem (200 mg/body on day 1), repeated every three weeks. Dose reductions of CF were considered in patients with impaired renal function, advanced age, or poor performance status. Specifically, in cases with creatinine clearance (Ccr) < 60 mL/min or eGFR < 60 mL/min/1.73 m², the initial dose was generally reduced to ≤80%. For patients with Ccr < 50 mL/min, the dose was further adjusted to 50–70%, and in those with a solitary kidney or severe renal impairment, the dose was reduced to approximately 50%. In elderly patients (≥75 years), the initial dose was reduced to 80–90% when the PS was 0–1, and to 50–70% in those with PS ≥ 2 or significant comorbidities. In patients with poor PS (≥2), the initial dose was usually reduced to 50–70% to minimize the risk of adverse events. In practice, the reduced-dose cohort consisted of two groups: 50% and 70%. Additional dose modifications were made on an individual basis, taking into account comorbid conditions (e.g., cardiac disease, sequelae of cerebrovascular disorders) or prior treatment-related toxicities. However, the Pem dosage was not reduced. If adverse events persisted, the treatment interval was extended to four weeks. The treatment was continued until disease progression or unacceptable toxicity was observed. The tumor response was assessed every 8 weeks in the first year and every 12 weeks thereafter.
2.4. Evaluation Criteria
The efficacy was assessed using the overall response rate (ORR [CR + PR]) and disease control rate (DCR [CR + PR + SD]). OS and PFS were measured from treatment initiation to death and cancer progression, respectively. Additionally, we evaluated the frequency and severity of treatment-related adverse events according to CTCAE version 5.0. Associations between initial dose intensity and outcomes were also examined.
2.5. Statistical Analyess
All analyses were performed using the Easy R software (EZR, version 1.55). Continuous variables are expressed as medians (range), and categorical variables are expressed as proportions. Chi-squared or Fisher’s exact tests were used for categorical comparisons. OS and PFS were estimated using the Kaplan–Meier method and compared using the log-rank test. Statistical significance was set at p < 0.05.
3. Results
3.1. Characteristics of the Patients
A total of 54 patients with unresectable or recurrent esophageal cancer who received CF plus Pem therapy between February 2022 and February 2025 were enrolled in this study. Their median age was 72.5 years (range, 44–91 years), and 40 patients (74.1%) were male. Overall, 75.9% of patients had PS of 0–1. CPS was examined in 23 patients: CPS ≥ 10 in 16 cases (69.6%), CPS < 10 in 7 cases (30.4%), and not assessed in 31 cases. Renal dysfunction, defined as eGFR < 60 mL/min/1.73 m^2^, was present in 15 patients (27.8%). In addition, 26 patients (48.1%) had creatinine clearance (Ccr) < 60 mL/min, including 15 patients (27.8%) with Ccr < 50 mL/min (Table 1). The most frequent tumor location was the middle thoracic esophagus; 53 patients had squamous cell carcinoma. The most common metastatic sites were the extra-regional lymph nodes, followed by the lungs and the liver.
3.2. Dose Intensity of Cisplatin and 5-Fluorouracil and Modification of the Treatment Interval
The initial CF dose was 100% in 24 patients (44.4%), 90% in 2 (3.7%), 80% in 9 (16.7%), and <80% in 19 (35.2%). Dose reduction was performed in patients with renal dysfunction (n = 24), advanced age (n = 14), or poor PS (n = 13). The treatment interval was extended to 4 weeks in 32 patients (59.3%) based on adverse events or PS during the first cycle, or if adverse events persisted thereafter (Table 2).
3.3. Treatment Outcomes
The ORR was 55.6%, including five cases of CR and 25 cases of PR. The DCR was 81.5%. In the lower dose group (initial CF dose < 80%), the ORR was 63.2% (CR, 2 cases; PR, 10 cases) and the DCR was 89.4%, with no significant difference compared to the non-reduction group. In older patients (aged ≥75 years), the ORR was 61.9% (CR, 3 cases; PR, 10 cases) and the DCR was 90.5% (Table 3). In the CPS ≥10 group, 2 patients achieved CR, 6 patients achieved PR, 5 patients achieved SD, and 3 patients achieved PD. In the CPS < 10 group, 1 patient achieved CR, 3 patients achieved PR, 1 patient achieved SD, and 2 patients achieved PD. There was no statistically significant difference (p = 0.857). Regarding the non-assessment group, there were 2 cases of CR, 16 cases of PR, 8 cases of SD, and 5 cases of PD. In the 50% dose group, 1 patient achieved CR, 7 patients achieved PR, 2 patients achieved SD, 2 patients achieved PD. In the 70% dose group, 1 patient achieved CR, 1 patient achieved PR, 1 patient achieved SD. There was no statistically significant difference (p = 0.446). Thus, although there was a wide range of reductions in the dose of chemotherapy, no significant differences were observed in the therapeutic effect.
The median OS and PFS were 18.6 (range, 9.1–24.6 months) and 6.5 months (range, 4.7–16.3 months), respectively (Figure 1). Although not statistically significant, patients with recurrent disease showed a trend toward longer OS and PFS than those with unresectable disease (OS, p = 0.06; PFS, p = 0.05) (Figure 2). In the lower dose group (initial CF dose < 80%), the median OS and PFS were 15.3 (range, 2.7–24.6 months) and 8.1 months (range, 2.4–17.0 months), respectively. No significant differences in OS or PFS were observed between groups (OS, p = 0.28; PFS, p = 0.23) (Figure 3).
Survival analysis based on age (≥75 vs. <75 years) showed no significant differences in OS or PFS (OS, p = 0.32; PFS, p = 0.31) (Figure 4). Similarly, no significant differences in OS or PFS were observed between patients treated at the 3- and 4-week intervals.
3.4. Safety
Adverse events of grade 3 or higher were observed in 10 patients (18.5%). The most frequent adverse event was neutropenia (six cases), while immune-related adverse events included interstitial pneumonitis (one case) and autoimmune encephalitis (one case) (Table 4). Adverse events were compared between the ≥80% dose group (n = 35) and the <80% dose group (n = 19) (Table 5). Although some adverse events were observed only in the <80% dose group, no statistically significant differences were detected between the two groups (all p-value > 0.05).
In our study, hyponatremia occurred during the first cycle and was managed with intravenous supplementation; however, subsequent decline in performance status led to discontinuation of chemotherapy. Hypocalcemia and hypomagnesemia developed during the second cycle, both managed with intravenous supplementation, after which treatment was continued with dose reduction. Adrenal insufficiency was observed in one patient during the second cycle, requiring oral steroid therapy, with chemotherapy continuation. Two additional cases occurred during the fifth cycle: one was managed with oral steroids and treatment continued, while the other required steroid pulse therapy followed by oral steroids, resulting in treatment discontinuation. Hypothyroidism occurred in two patients (during the first and fifth cycles, respectively), both requiring initiation of oral medication. Autoimmune encephalitis developed in one patient during the fifth cycle, necessitating steroid pulse therapy and subsequent discontinuation of chemotherapy. Interstitial pneumonitis developed during the sixth cycle and was managed with steroid pulse therapy, also leading to discontinuation of chemotherapy. The incidence of grade 3 or higher adverse events was lower in the lower dose group than in the higher dose group, with only two cases reported.
4. Discussion
The advent of ICIs has substantially changed the treatment paradigm for advanced esophageal cancer. The KEYNOTE-590 trial demonstrated that CF plus Pem therapy significantly improved OS and PFS compared with CF plus placebo, particularly in patients with high PD-L1 expression [13]. However, this trial included patients with relatively favorable clinical profiles—such as younger age, preserved renal function, and good PS—raising concerns about the generalizability of its findings among older or comorbid populations, especially considering the nephrotoxicity of cisplatin-based regimens [14,15,16].
In this study, we retrospectively analyzed the real-world clinical outcomes of CF plus Pem therapy for unresectable or recurrent esophageal cancer. A notable feature of this analysis was the inclusion of patients who underwent initial dose reduction owing to advanced age, renal dysfunction, or poor PS. This study provides meaningful insights into the practical feasibility, effectiveness, and safety of this regimen in routine clinical practice. In our study, approximately 40% of patients were aged ≥75 years and approximately 45% had impaired renal function (eGFR < 60 mL/min/1.73 m^2^ or Ccr < 60 mL/min). Only 44.4% of patients received the full initial CF dose; the remainder underwent dose reduction primarily because of renal dysfunction or advanced age. Importantly, the ORR and DCR were comparable between the dose reduction and non-reduction groups 63.2% vs. 51.4% for ORR and 89.5% vs. 77.1% for DCR), with no significant differences (ORR: p = 0.57; DCR, p = 0.47). These results suggest that individualized dose adjustments, such as initial dose reduction based on age, renal function, and PS, may help preserve therapeutic efficacy, while potentially reducing the risk of treatment discontinuation due to toxicity, particularly in vulnerable populations [9,15]. The median OS and PFS were 18.6 (range, 9.1–24.6 months) and 6.5 months (range, 4.7–16.3 months), respectively. When stratified by disease status, patients with recurrent disease demonstrated a trend toward longer OS and PFS than those with initially unresectable disease, although the differences were not significant (OS, p = 0.06; PFS, p = 0.05). These nonsignificant trends may be attributed to the limited statistical power owing to the small sample size of this retrospective study. These differences may become more pronounced and reach statistical significance in larger cohorts. In the lower dose group (initial CF dose < 80%), the median OS and PFS were 15.3 (range, 2.7–24.6 months) and 8.1 months (range, 2.4–17.0 months), respectively, with no significant difference in OS or PFS (OS, p = 0.28; PFS, p = 0.23) compared to higher dose group. Notably, the median OS in the lower dose group was comparable with that reported in the KEYNOTE-590 trial (Pem plus chemotherapy median OS, 12.4 months in the overall population) [13]. This suggests that clinically meaningful survival benefits may be maintained in real-world settings even with an initial dose reduction. In older patients, a comprehensive assessment is essential because of age-related decline in organ function, comorbidities, and nutritional status. Aggressive treatment based solely on chronological age is often withheld; however, recent studies have suggested that personalized treatment based on tumor characteristics can yield favorable outcomes in older adults [16,17,18,19,20,21]. Our previous study reported good outcomes in patients aged ≥80 years who underwent dose-adjusted definitive chemoradiotherapy [22]. The present findings reinforce this notion, indicating that appropriate dose modifications can lead to satisfactory outcomes even in older patients. Furthermore, the incidence of grade ≥3 adverse events was relatively low (18.5%). Major adverse events included neutropenia, interstitial pneumonia, and irAEs, all of which were manageable with appropriate interventions. The lower incidence of irAEs in older patients may be due to immunosenescence, which reduces the immune reactivity. Some studies have suggested that irAEs may be less frequent in this population [23,24,25,26,27], supporting the rationale for administering Pem without dose reduction. Although this study included patients with advanced disease and distant metastases, some achieved CR or sustained SD, suggesting that the durable antitumor effects of immunotherapy may extend to metastatic lesions. Previous reports have shown better response rates in patients with lung or regional lymph node metastases, possibly because of the characteristics of the tumor microenvironment (TME) [28,29,30]. ICIs are thought to modify the TME, enhance immune cell infiltration, and improve tumor recognition, potentially leading to synergistic effects when combined with chemotherapy. These mechanisms may contribute to improved metastatic control and pave the way for conversion surgery, ultimately leading to improved survival.
Nonetheless, this study had some limitations that must be acknowledged. First, the retrospective, single-center nature of this study may have introduced selection and information biases. Second, the relatively small sample size limited the statistical power of multivariate and subgroup analyses. Thirdly, the relatively short follow-up period may have resulted in immature survival data. Future multicenter prospective studies are required to validate these findings and clarify the role of CF plus Pem therapy in real-world clinical settings.
5. Conclusions
Despite the limitations of this retrospective single-institution study, our findings provide important real-world evidence regarding the use of CF plus pembrolizumab for unresectable or recurrent esophageal cancer. The overall response rate was 55.6%, with a disease control rate of 81.5%, and the median progression-free and overall survival were 6.5 and 18.6 months, respectively. Notably, dose reduction of cisplatin and 5-fluorouracil, often required in elderly patients or those with renal dysfunction, did not compromise treatment efficacy, and the incidence of grade ≥3 adverse events was lower in the reduced-dose group. These results suggest that CF plus pembrolizumab can be safely and effectively administered across diverse clinical backgrounds, including older patients and those with impaired renal function. Given the aging global population, the implementation of flexible, patient-tailored treatment strategies is essential. This study highlights the feasibility of dose-adjusted CF plus pembrolizumab as a practical treatment option and provides valuable evidence to guide future optimization and personalization of therapy for patients with unresectable or recurrent esophageal cancer.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ferlay J. Ervik M. Lam F. Laversanne M. Colombet M. Mery L. Piñeros M. Znaor A. Soerjomataram I. Bray F. Global cancer observatory Cancer Today International Agency for Research on Cancer Lyon, France 2022 Available online: https://gco.iarc.who.int/today(accessed on 30 August 2025)
- 2National Cancer Institute Japan. Cancer Information Service: Cancer Statistics Available online: https://ganjoho.jp/reg_stat/statistics/stat/summary.html(accessed on 30 August 2025)
- 3Guo D. Jin J. Li D. He Y. Lin Y. Analysis of the incidence and mortality trends of esophageal cancer in cancer registry areas of China and Japan Int. J. Cancer 20241551376138610.1002/ijc.3500338771567 · doi ↗ · pubmed ↗
- 4Kato H. Nakajima M. Treatments for esophageal cancer: A review Gen. Thorac. Cardiovasc. Surg.20136133033510.1007/s 11748-013-0246-023568356 · doi ↗ · pubmed ↗
- 5Bleiberg H. Conroy T. Paillot B. Lacave A.J. Blijham G. Jacob J.H. Bedenne L. Namer M. De Besi P. Gay F. Randomised phase II study of cisplatin and 5-fluorouracil (5-FU) versus cisplatin alone in advanced squamous cell oesophageal cancer Eur. J. Cancer 1997331216122010.1016/S 0959-8049(97)00088-99301445 · doi ↗ · pubmed ↗
- 6Iizuka T. Kakegawa T. Ide H. Ando N. Watanabe H. Tanaka O. Takagi I. Isono K. Ishida K. Arimori M. Phase II evaluation of cisplatin and 5-fluorouracil in advanced squamous cell carcinoma of the esophagus: A Japanese Esophageal Oncology Group Trial Jpn. J. Clin. Oncol.1992221721761518165 · pubmed ↗
- 7Hayashi K. Ando N. Watanabe H. Ide H. Nagai K. Aoyama N. Takiyama W. Ishida K. Isono K. Makuuchi H. Phase II evaluation of protracted infusion of cisplatin and 5-fluorouracil in advanced squamous cell carcinoma of the esophagus: A Japan Esophageal Oncology Group (JEOG) Trial (JCOG 9407)Jpn. J. Clin. Oncol.20013141942310.1093/jjco/hye 09011689594 · doi ↗ · pubmed ↗
- 8Lorenzen S. Schuster T. Porschen R. Al-Batran S.E. Hofheinz R. Thuss-Patience P. Moehler M. Grabowski P. Arnold D. Greten T. Cetuximab plus cisplatin-5-fluorouracil versus cisplatin-5-fluorouracil alone in first-line metastatic squamous cell carcinoma of the esophagus: A randomized phase II study of the Arbeitsgemeinschaft Internistische Onkologie Ann. Oncol.2009201667167310.1093/annonc/mdp 06919549707 · doi ↗ · pubmed ↗