Case Report: Transient monocular vision loss with isolated paracentral acute middle maculopathy on optical coherence tomography: beware of giant cell arteritis!
George Alencastro Landim, Etienne Bénard-Séguin, Nancy J. Newman, Valérie Biousse

TL;DR
An 80-year-old woman with transient vision loss and a specific OCT finding was diagnosed with giant cell arteritis, highlighting the importance of early detection.
Contribution
This case highlights PAMM on OCT as a rare, early indicator of GCA without typical ocular signs.
Findings
PAMM on OCT was the only ocular sign of GCA in a patient with transient vision loss.
The patient had no permanent vision loss or ischemia on retinal angiography.
Immediate treatment with steroids prevented further complications.
Abstract
We describe a case of transient monocular vision loss (TMVL) and paracentral acute middle maculopathy (PAMM) on optical coherence tomography (OCT) as the only ocular presentation of biopsy-proven GCA. An 80-year-old woman presented 4 days after an episode of TMVL in the right eye, which lasted for 2 hours and spontaneously resolved. She also had jaw claudication for 1 month. Visual acuity was 20/20 in both eyes, with no relative afferent pupillary defect. Funduscopic examination was normal. Humphrey visual fields (HVF 24-2) were full in both eyes. Spectral domain OCT of the right eye demonstrated a focal lesion with increased hyperreflectivity at the level of the inner nuclear layer, consistent with PAMM. Fluorescein angiography and indocyanine angiography were normal. She was immediately treated with intravenous steroids for presumed giant cell arteritis (GCA), confirmed subsequently…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
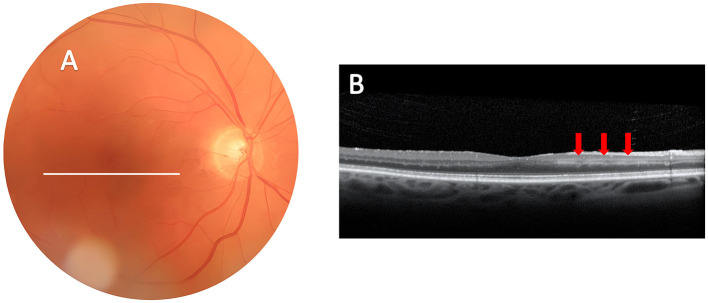 Figure 1
Figure 1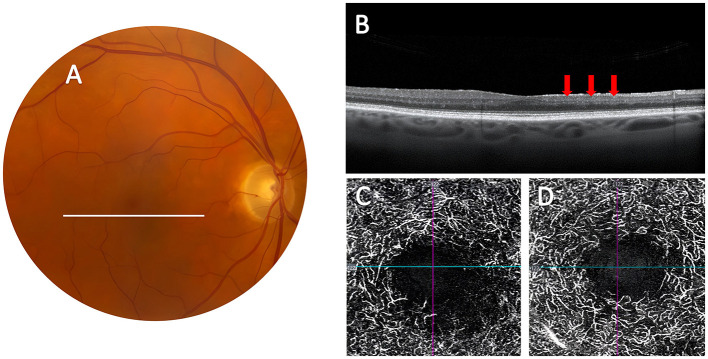 Figure 2
Figure 2|
|
|
|
|
|
|
|
|
|---|---|---|---|---|---|---|---|
| Christenbury et al. ( | M/82 | Yes; Multiple for 2 days | Yes | Negative | ESR ↑ CRP ↑ | Count fingers | Normal |
| Kasimov et al. ( | F/73 | Yes; Multiple for 10 days | Yes | Positive | ESR ↑ CRP ↑ | Count fingers | Cotton wool spots, AION, cilioretinal artery occlusion |
| Pellegrini et al. ( | F/72 | Yes; 3 days prior | Yes | Positive | ESR ↑ CRP ↑ | 20/25 with paracentral scotoma | Retinal whitening |
|
|
|
|
|
|
|
| |
| Pichi et al. ( | F/67 | No | Yes | Positive | NA | 20/150 | Cilioretinal artery occlusion |
| F/67 | No | Yes | Positive | NA | 20/200 | Cilioretinal artery occlusion | |
| Ahuja et al. ( | F/75 | No | No | Positive | Normal | 20/80 | Cotton wool spots |
| M/58 | No | No | Positive | ESR ↑ | NA | AION | |
| Narala et al. ( | M/86 | No | No | Positive | ESR ↑ CRP ↑ | 20/60 | Cotton wool spots and retinal whitening |
| Broyles et al. ( | F/75 | No | No | Positive | ESR ↑ CRP ↑ | 20/30 with paracentral scotoma | Cotton wool spots |
| Sodhi et al. ( | F/75 | No | No | Positive | ESR ↑ CRP ↑ | 20/20 with paracentral scotoma | Subtle retinal whitening |
| Pellegrini et al. ( | M/63 | No | No | Positive | ESR ↑ CRP ↑ | 20/25 with paracentral scotomas at presentation, but no light perception 3 weeks later | Isolated PAMM at presentation AION 3 weeks later |
| Mairot et al. ( | 5M/11F; Mean age 81.6 | NA | NA | 3/3 positive; 10 MRI positive | NA | Mean of 20/400 (range 20/20 to light perception) | 6 patients isolated PAMM 10 patients AION or CRAO |
| Mairot et al. ( | F/85 | NA | NA | Positive | CRP ↑ | worse than 20/2,000 | AION |
| F/66 | NA | NA | Positive | CRP ↑ | worse than 20/2,000 | AION | |
| F/69 | NA | NA | Positive | CRP ↑ | 20/300 | AION | |
| F/68 | NA | NA | Positive | CRP ↑ | 20/2,000 | AION | |
| Klefter et al. ( | 5F/3M; Mean age 74.5 | NA | NA | Positive TAB or PET | NA | NA | AION |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsRetinal and Optic Conditions · Ocular Diseases and Behçet’s Syndrome · Vasculitis and related conditions
Introduction
The most dreaded complication of giant cell arteritis (GCA) is permanent vision loss, most often from anterior ischemic optic neuropathy (AION), not infrequently preceded by episodes of transient monocular vision loss (TMVL) (1). Prompt treatment of GCA patients with TMVL with high-dose intravenous steroids is the only way to prevent permanent vision loss and second eye involvement (1). The presence of systemic symptoms suggestive of GCA and findings of elevated erythrocyte sedimentation rate (ESR), C-reactive protein (CRP) and thrombocytosis are very useful for the diagnosis, but they are not always present, making the decision whether to immediately treat patients with vision complaints with steroids often challenging (1). Recent reports of paracentral acute middle maculopathy (PAMM) on macular optical coherence tomography (OCT) in GCA patients suggest that this OCT finding may be helpful in the early diagnosis of GCA, especially in patients with AION (2–5). PAMM is an OCT finding defined by the presence of a hyperreflective band at the level of the inner nuclear layer (INL) of the retina that indicates focal retinal infarction caused by globally impaired perfusion through the retinal capillary system (6–8). Lesions can be caused by various local retinal vascular diseases and systemic disorders, and the presence of PAMM in a patient with transient vision loss suggests a definite vascular mechanism (7, 8). Most cases of GCA and PAMM reported in the literature have had permanent vision loss and other funduscopic findings, including cotton wool spots, retinal whitening, extensive retinal ischemia from central retinal artery occlusion (CRAO), cilioretinal artery occlusion or AION (2, 3, 5, 8–15) (Table 1). We describe a case of TMVL and PAMM as the only ocular presentation of biopsy-proven GCA.
Case report
An 80-year-old white woman presented to our emergency department (ED) 4 days after an episode of a gray band in the central vision of the right eye that lasted for 2 hours and spontaneously resolved. Medical history was remarkable for polymyalgia rheumatica (PMR) diagnosed 18 months prior, treated with oral prednisone that was discontinued 2 months prior to presentation, and jaw claudication for 1 month. In the ED, the patient had non-mydriatic ocular fundus imaging, including color photographs and OCT of the optic nerve and macula (10). Remote review of these imaging studies showed no obvious retinal or optic nerve abnormalities and no retinal emboli. However, the macular OCT suggested a focal retinal area of hyper-reflectivity in the right macula. The patient was seen immediately by Neuro-ophthalmology where visual acuity was 20/20 in both eyes, color vision was normal and there was no relative afferent pupillary defect. 24-2 SITA-Fast Humphrey visual fields (HVF) were full in both eyes. Funduscopic examination and repeat color fundus photography were normal with no evidence of retinal ischemia. Repeat OCT of the right eye confirmed focal areas of increased hyperreflectivity at the level of the INL, nasal to the macula, consistent with PAMM (Figure 1). Fluorescein angiography (FA) and indocyanine angiography (ICG) were normal, with no choroidal hypoperfusion. ESR was normal at 20 (reference < 30 mm/h) and CRP was mildly elevated at 27 (reference < 10 mg/L). She was admitted to the hospital with high suspicion for TMVL from GCA, and was immediately started on intravenous methyl prednisolone 250 mg, 4 times per day. A right temporal artery biopsy (TAB) performed 1 day after admission demonstrated giant cells in the wall of the artery and around the inner elastic lamina, confirming the diagnosis of GCA. She was discharged 4 days later on oral prednisone and her vision remained normal in both eyes. She was last seen at 36-week follow-up at which time she was taking oral prednisone 5 mg daily and tocilizumab 162 mg injection weekly. She did not have any visual symptoms and repeat 24-2 HVF was normal. Repeat OCT showed an area of atrophy where PAMM was previously noted, correlating with abnormal vasculature on OCT-angiography (OCT-A) (Figure 2).
Demonstration of paracentral acute middle maculopathy on ocular imaging obtained four days after transient monocular vision loss in the right eye. (A) Color fundus photograph of the right eye is normal. White line corresponds to the scan area of the SD-OCT. (B) SD-OCT of the macula shows hyperreflective focal lesions at the level of the inner nuclear layer (red arrows), consistent with ischemia of the deeper vascular complex of the inner retina as seen with PAMM.
Evolution of paracentral acute middle maculopathy on ocular imaging obtained 36 weeks after presentation. (A) Color fundus photograph of the right eye remained normal. (B) SD-OCT of the macula shows evolution of the lesion with thinning at the level of the inner nuclear layer (red arrows). (C) OCT-A of the DCP with attenuation of the capillaries in the inferonasal parafoveal area the right eye. (D) OCT-A with normal parafoveal capillaries of the DCP in the left eye.
Discussion
Our patient's unique presentation of TMVL from GCA with normal visual function and normal funduscopic appearance, but with findings of PAMM on macular OCT 4 days after TMVL, highlights the usefulness of performing a macular OCT acutely in patients with TMVL. Our patient was found to have PAMM on non-mydriatic OCT obtained in our ED (17, 18), which prompted immediate evaluation in our clinic and rapid diagnosis of presumed GCA. She received intravenous steroids rapidly after arriving in the ED, and her visual function remained normal. Although PAMM may be seen in patients with non-arteritic TMVL (19), non-arteritic reperfused CRAO (7, 19) or even central retinal vein occlusions (CRVO) (20), its presence should always suggest the possibility of GCA in patients aged 50 years and older (13–16).
The number of reported cases of PAMM in GCA remains low (Table 1), but this number likely largely underestimates the true prevalence of PAMM in GCA. PAMM is only seen on retinal OCT, and many GCA patients, especially those presenting with vision loss from optic neuropathy or those with isolated TMVL, do not have systematic macular OCT performed acutely. Most reported patients with PAMM and GCA have had permanent vision loss and obvious funduscopic abnormalities suggesting retinal ischemia, such as cotton wool spots, areas of retinal whitening, CRAO or optic disc edema from AION, and were seen in eye clinics where OCT is routinely used. Our patient's ocular fundus was normal, as were retinal FA and ICG, as similarly reported by Sodhi et al. in one patient with PAMM and GCA (15).
PAMM is one of the newer retinal OCT findings that have emerged with the advent of high-resolution spectral domain OCT and OCT-A which provide exquisite images of the retinal layers and retinal vessel changes at various depths (18, 21–24). PAMM is described on OCT as a hyper-reflective band at the level of the retinal INL, eventually leading to permanent thinning of the INL as shown in Figures 1, 2 (7, 8, 22). The INL is located in a region of the retina where oxygen is supplied by both the choroidal and retinal circulations, hence considered a watershed region most susceptible to early ischemia (7, 8, 22–28). The macula's oxygen demand, especially in the inner retinal segments and at the photoreceptor level, is higher than in any other retinal region. Although the choroidal vasculature in the macula is increased to fill this metabolic demand, oxygen diffusion from the choroid to the retina is limited by retinal thickness, which is greatest in the parafoveal region (7, 8, 25), and is often compromised in vasculitic disorders such as GCA (23). PAMM results from focal ischemia of the intermediate and deep capillary plexi, which are responsible for the blood supply to the middle retina which includes the INL (7, 8). This area can be visualized with OCT-A which demonstrates reduced superficial and deep capillary plexi in PAMM (28). We did not perform OCT-A acutely in our patient. However, when seen in follow-up 36 weeks later, OCT-A showed lower capillary density and attenuated deep capillary plexus in the eye with PAMM compared to the fellow eye (Figure 2).
PAMM has been linked to various retinal vascular ischemic disorders, underscoring the critical role of vascular dysfunction in its pathogenesis (7, 8). The literature is mostly based on case reports and small case series, which have reported PAMM in association with CRAO, branch retinal artery occlusions (BRAO), CRVO, Purtscher retinopathy, sickle cell disease, hypercoagulable states, and systemic vasculitic disorders, either auto-immune or post-infectious (7, 8, 26).
PAMM is an important finding in patients with TMVL or those with mild visual symptoms, as selective infarction of the retinal INL may precede devastating subsequent vision loss from severe retinal or optic nerve ischemia (4, 20). Pellegrini et al. reported a 63-year-old man with mild vision loss in one eye who was found to have PAMM as the only finding at initial presentation (16). The diagnosis of GCA was not made at that initial visit and the patient returned 3 weeks later with severe vision loss and pallid optic disc edema in the contralateral eye, consistent with AION from GCA. Among the cases with PAMM and GCA reported in detail in the literature (Table 1), only 3 patients (11–13). other than our case were documented to have experienced TMVL prior to presentation, including only one other patient treated early enough to prevent severe vision loss (13). A recent study suggested that the presence of PAMM in a patient with AION may be a strong argument for GCA, especially in the absence of subretinal fluid tracking from the swollen optic disc toward the macula (5).
Conclusion
PAMM is a relatively new OCT finding associated with acute retinal ischemia, the significance of which needs to be fully understood before specific recommendations can be made. Our case and other recent reports confirm that PAMM is secondary to focal acute retinal ischemia and may precede more severe retinal ischemia and vision loss. Although most reported patients with GCA and PAMM had other obvious funduscopic findings of ischemia and already had severe vision loss at the time of presentation, the diagnosis of PAMM in a patient with TMVL and normal funduscopic examination should prompt urgent evaluation in order to potentially prevent permanent vision loss from a disorder such as GCA. Similarly, systematic urgent OCT of the macula in patients with TMVL and those with AION may help identify the subgroup of patients at risk for bilateral severe retinal ischemia from GCA. OCT and OCTA are routinely used in eye clinics and are widely available, but may not be systematically performed in patients with isolated TMVL (18). Although very few EDs are equipped with OCTs, the growing interest in non-mydriatic ocular imaging in EDs including with OCT, with remote interpretation by ophthalmologists (17, 18, 29, 30), could greatly improve the evaluation of acute TMVL patients in emergency settings.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Baig I Pascoe A Kini A Lee A. Giant cell arteritis: early diagnosis is key. Eye Brain. (2019) 11:1–12. 10.2147/EB.S 17038830697092 PMC 6340646 · doi ↗ · pubmed ↗
- 2Mairot K Gascon P Stolowy N Comet A Attia R Beylerian M. Paracentral acute middle maculopathy as a specific sign of arteritic anterior ischemic optic neuropathy. Am J Ophthalmol. 2023; 1:248:1-7. 10.1016/j.ajo.2022.09.01936228776 · doi ↗ · pubmed ↗
- 3Broyles H Chacko J Chancellor J Lo Russo F Phillips P Mashayekhi A. Paracentral acute middle maculopathy as the initial presentation of giant cell arteritis. J Neuroophthalmol. (2021) 41:157–9. 10.1097/WNO.000000000000122233770010 · doi ↗ · pubmed ↗
- 4Bousquet E Santina A Abraham N Daily MJ Sarraf D. Detection of paracentral acute middle maculopathy can prevent blindness and death. Retina. (2023) 43:1827–32. 10.1097/IAE.000000000000393937748460 · doi ↗ · pubmed ↗
- 5Klefter ON Hansen MS Lykkebirk L Subhi Y Brittain JM Jensen MR. Combining paracentral acute middle maculopathy and peripapillary fluid as biomarkers in anterior ischemic optic neuropathy. Am J Ophthalmol. (2024) 271:329–36. 10.1016/j.ajo.2024.12.00139645178 · doi ↗ · pubmed ↗
- 6Scharf J Freund KB Sadda S Sarraf D. Paracentral acute middle maculopathy and the organization of the retinal capillary plexuses. Prog Retin Eye Res. (2021) 81:100884. 10.1016/j.preteyeres.2020.10088432783959 · doi ↗ · pubmed ↗
- 7Fumi D Ruggeri F Fasciolo D Antonello E Burtini G Abdolrahimzadeh S. Paracentral acute middle maculopathy (PAMM) in ocular vascular diseases-what we know and future perspectives. Vision (Basel). (2025) 9:19. 10.3390/vision 901001940137931 PMC 11946784 · doi ↗ · pubmed ↗
- 8Pichi F Fragiotta S Freund KB Au A Lembo A Nucci P. Cilioretinal artery hypoperfusion and its association with paracentral acute middle maculopathy. Br J Ophthalmol. (2019) 103:1137–45. 10.1136/bjophthalmol-2018-31277430257961 · doi ↗ · pubmed ↗