Right Femoral Pseudoaneurysm Versus Inguinal Abscess: Progressive Inguinal Mass Following Blunt Trauma
Emily Cushman, Danijela Lonco, James White, Rebecca Perry

TL;DR
A woman with a growing groin mass after trauma was initially thought to have a pseudoaneurysm but was found to have an abscess, highlighting the need for advanced imaging in such cases.
Contribution
The case emphasizes the limitations of ultrasonography in distinguishing abscesses from pseudoaneurysms and the value of CT angiography for accurate diagnosis.
Findings
Ultrasonography showed a vascularized mass but could not confirm a pseudoaneurysm.
CT angiography was necessary to guide surgical intervention for an abscess.
The patient's symptoms and imaging findings were initially inconclusive.
Abstract
When evaluating a patient with inguinal swelling following blunt trauma, maintaining a broad differential diagnosis is crucial, especially when laboratory and imaging findings do not correlate with the patient’s history. An important consideration is the choice of imaging modality to assess progressively worsening inguinal pain and swelling. A 21-year-old healthy female presented to the ED with a progressively enlarging mass in the right inguinal region following traumatic injury. She had undergone two prior evaluations by an OB-GYN, with recommendations for acetaminophen and NSAIDs, which provided no relief. The mass had increased in size relative to her discomfort, causing difficulty ambulating. On initial presentation, she was afebrile but tachycardic. Physical examination revealed significant right-sided vaginal edema extending throughout the inguinal region without overlying…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1 Figure 2
Figure 2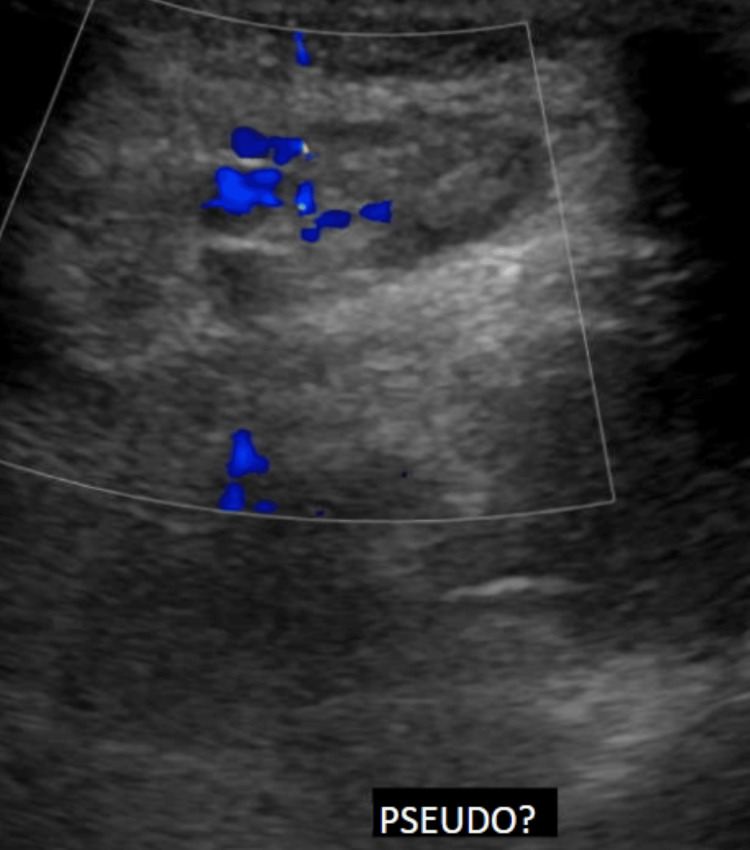 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVascular Procedures and Complications · Case Reports on Hematomas · Ultrasound in Clinical Applications
Introduction
Inguinal masses can have a multitude of causes, ranging from relatively benign conditions such as lipomas or cysts to more concerning etiologies like pseudoaneurysms, malignancy, or abscesses. Because of the wide spectrum of possible causes and presentations, appropriate evaluation and diagnostic imaging are essential [1]. Imaging that helps determine the likely origin of the mass is particularly important. Intrapelvic versus extrapelvic masses require distinct considerations for further evaluation and management [2]. CT imaging should be considered, given the difficulty in differentiating hematomas, pseudoaneurysms, and abscesses on ultrasound [3,4].
Pseudoaneurysms are uncommon in young individuals, with the most frequent causes being recent endovascular procedures; however, blunt trauma can also result in vascular injury. Here, we present a case of an abscess that mimicked the features of a pseudoaneurysm and was initially diagnosed as such on imaging following blunt trauma to the groin.
Case presentation
A 21-year-old previously healthy female presented to our ED with complaints of a progressively worsening mass in her right groin. She reported first noticing the mass after an incidental blunt trauma to the groin. She had previously been evaluated by her OB-GYN, who recommended acetaminophen and NSAIDs, which provided no relief. The increasing discomfort and eventual difficulty ambulating due to pain prompted her arrival in the ED. She had no prior history of a mass in the inguinal region.
On arrival, vital signs revealed tachycardia and fever. Physical examination demonstrated significant right-sided vaginal edema extending throughout the inguinal region without overlying integumentary changes, abrasion, laceration, or ecchymosis. A mass measuring approximately 3 × 4 cm was noted (Figure 1). The mass was nonpulsatile.
Physical exam findings in the EDRight inguinal fold mass with mild overlying erythema. No obvious signs of trauma.
Laboratory studies were obtained and were notable only for a leukocytosis of 18. Initial imaging included a CT of the pelvis, which demonstrated a right inguinal pseudoaneurysm of indeterminate origin with a surrounding hematoma measuring 4.3 × 3.7 cm (Figure 2).
CT pelvis, static imageFindings suggest a pseudoaneurysm with a surrounding hematoma. No obvious signs of localized fat stranding.
Vascular surgery was consulted, and the patient was admitted for further evaluation and management. A vascular ultrasound performed by the vascular surgeon revealed a vascularized region measuring 2.07 × 1.17 cm, with an inability to rule out a pseudoaneurysm (Figure 3). The patient was subsequently taken to the operating room for further intervention.
Vascular ultrasound of the right inguinal mass, static imageDoppler flow is noted within the mass. Imaging is indeterminate, and a pseudoaneurysm cannot be ruled out.
During incision and local exploration, an abscess was identified in the right inguinal region. The abscess was incised and drained, with purulent material noted. Cultures were obtained, and the area was thoroughly irrigated. Cultures grew Streptococcus pyogenes. The patient was started on appropriate intravenous antibiotics, later transitioned to oral antibiotics, and was eventually discharged home with outpatient follow-up.
Discussion
Inguinal masses can arise from a variety of pathologies, with emphasis on differentiating localized soft tissue masses or infections from deeper underlying pathology [1]. Typically, femoral pseudoaneurysms occur secondary to recent vascular access; however, they can also result from blunt trauma, as in this patient, and may progressively enlarge, potentially leading to rupture [5]. The primary focus in the ED is to establish the most likely diagnosis and determine appropriate next steps for treatment or management. An important aspect of this process is selecting the most appropriate diagnostic imaging or determining whether imaging is indicated at that time. The two most common imaging modalities obtained in the ED are CT and ultrasound, either point of care or formal.
When selecting imaging, the patient’s presentation, history, and physical examination findings must be considered. Suspected soft tissue masses are often initially evaluated via point-of-care ultrasound to assess for drainable fluid collections beneath the skin surface [6,7]. However, sonographic imaging can be misleading. Ultrasound may have difficulty differentiating a pseudoaneurysm from an abscess or hematoma due to similar anechoic to hypoechoic appearances, making clinical correlation essential [4].
In this case, the patient presented with a progressively enlarging inguinal mass, unresponsive to acetaminophen and ibuprofen, with mild overlying erythema. Ultrasound is a reasonable initial modality to rule out a simple abscess and minimize unnecessary radiation exposure; however, if Doppler flow is noted, further imaging with CT angiography should be considered. CT angiography provides detailed information regarding vascular involvement and other pathology [4], and it also facilitates treatment planning, whether medical management or surgical intervention. Despite its utility, imaging is not always conclusive, as demonstrated in this case.
For most abscesses, point-of-care ultrasound is appropriate for assessing the size of the fluid collection prior to incision and drainage. Clinical symptoms and laboratory findings can also aid in diagnosis, as pyogenic inguinal abscesses may present with fever and leukocytosis [2]. However, for suspected inguinal abscesses, ultrasound alone is insufficient. CT should be performed to determine whether the abscess is intrapelvic or extrapelvic and to evaluate for communication or tract formation [1,2]. Determining the abscess origin helps guide appropriate antibiotic therapy; intrapelvic abscesses require coverage for anaerobic organisms [2]. Doppler ultrasound may help identify blood flow, but it can be inconclusive, as seen in this case, and its accuracy depends on the operator’s skill and probe positioning.
Not all patient presentations have histories that clearly align with the final diagnosis. In this case, the patient presented after blunt trauma to the groin with worsening symptoms suggestive of possible hematoma expansion or vascular injury. Leukocytosis and fever may have been attributable to a stress response from trauma as well as inflammation from a developing infection or abscess [2]. Ultimately, the patient required surgical intervention, either for vascular repair or incision and drainage of an abscess.
Conclusions
Due to the complexity of the pelvic region and the wide range of potential pathologies, CT is the optimal diagnostic imaging modality for evaluating inguinal masses, particularly in patients with concerning presentations. Point-of-care ultrasound can be useful for initial differentiation of solid versus cystic or fluid-filled masses but should not serve as the definitive diagnostic tool for concerning inguinal masses.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1The inguinal canal: anatomy and imaging features of common and uncommon masses Radiographics Bhosale PR Patnana M Viswanathan C Szklaruk J 8198352820081848048610.1148/rg.283075110 · doi ↗ · pubmed ↗
- 2The role of cross sectional imaging in the management of acute pyogenic inguinal abscess - extrapelvic versus intrapelvic origin BMC Infect Dis Hsu WH Lee CY Lai LJ Huang TY Peng KT 1551320132353745510.1186/1471-2334-13-155PMC 3639101 · doi ↗ · pubmed ↗
- 3Femoral artery pseudoaneurysm Stat Pearls [Internet] Tulla K Kowalski A Qaja E Treasure Island (FL)Stat Pearls Publishing 2025 https://pubmed.ncbi.nlm.nih.gov/29630262/29630262 · pubmed ↗
- 4Groin abnormalities: ultrasonographic and clinical findings Ultrasonography Yang DM Kim HC Kim SW Won KY 1661773920203178690510.14366/usg.19041 PMC 7065985 · doi ↗ · pubmed ↗
- 5Do not underestimate the femoral pseudoaneurysm Vasa Stolt M Braun-Dullaeus R Herold J 1771854720182943961110.1024/0301-1526/a 000691 · doi ↗ · pubmed ↗
- 6Imaging of pseudoaneurysms: key diagnostic findings, causes and complications Radiologia (Engl Ed) Moreno Real D de Araújo Martins-Romêo D 2022136720254018781210.1016/j.rxeng.2024.07.002 · doi ↗ · pubmed ↗
- 7Ultrasonography in the emergency department Crit Care Whitson MR Mayo PH 2272020162752388510.1186/s 13054-016-1399-x PMC 4983783 · doi ↗ · pubmed ↗