Impact of Oral Health Training on Primary Health Care Workers in Gandaki Province of Nepal: A Pilot Study
Krishna Subedi, Umesh Parajuli, Prakash Raj Sharma, Ramesh Prasad Adhikari

TL;DR
A pilot study in Nepal found that oral health training significantly improved knowledge and practices among primary health care workers.
Contribution
The study demonstrates the effectiveness of targeted oral health training for primary health care workers in a specific regional context.
Findings
Oral health knowledge improved by 55.25% after the training (p < 0.001).
Use of interdental aids like dental floss increased from 35.29% to 86.36% post-training.
Abstract
This study was done to assess the impact of oral health training on primary health care (PHC) workers in Gandaki Province, Nepal. This quasi-experimental study was conducted among 24 PHC providers (auxiliary health workers [AHWs], and public health inspectors [PHIs]) attending the oral health training from 11 districts of Gandaki province. A non-randomized sampling technique was used. All participants present during the training session who provided written informed consent were included in the study. Dental experts provided training to the participants for 6 days, the last week of April 2025. The method of training uses a PowerPoint presentation, different tooth models and brushing models, diagnostic instruments, fluoride varnish, and videos. Oral health training was evaluated by assessing the improvements in oral health knowledge (OHK) and practice. There were 30 questions for…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
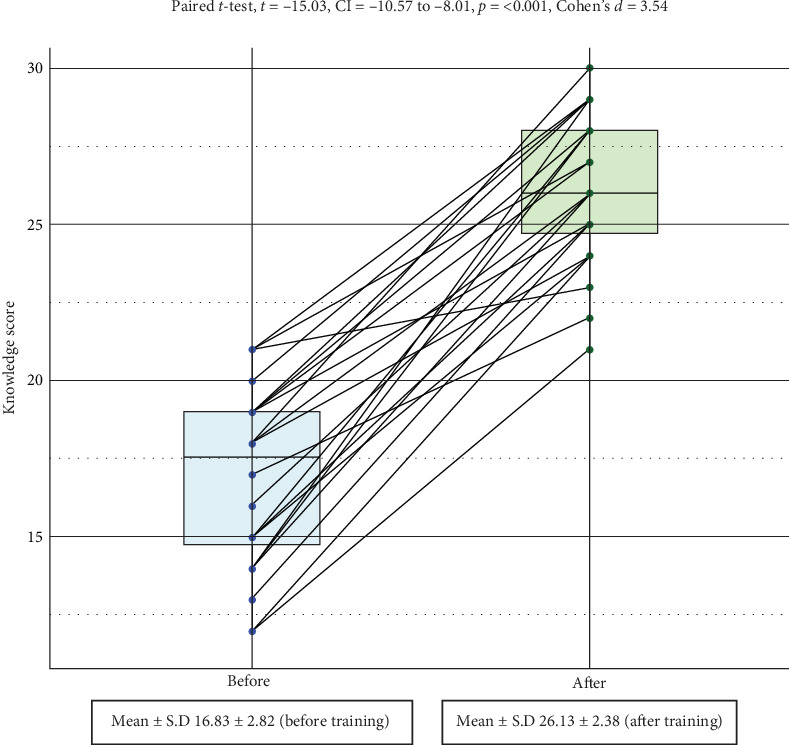 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDental Health and Care Utilization · Global Maternal and Child Health · Healthcare Systems and Reforms
1. Introduction
Oral diseases cover a spectrum of conditions, including dental caries, periodontal disease, tooth loss, oral cancer, oro–dental trauma, noma, and developmental disorders like cleft lip and palate. Oral diseases are among the most common noncommunicable diseases worldwide, with a disproportionate impact on vulnerable and disadvantaged populations [1]. Oral diseases are highly preventable [2], and oral health care should be integrated into primary healthcare services [3].
“Primary health care (PHC)” is the first level of contact where essential health care services are provided to an individual [4]. The World Health Organization (WHO) recommends achieving universal health coverage (UHC), and oral health services should be accessible and easily used by all people [5]. Oral health care should be integrated into PHC and ensure related financial protection and essential supplies in PHC [5]. Integration of essential oral health care into PHC and UHC is one of the six strategic objectives of the Global strategy on oral health [6].
Integrating oral health care into primary care is grounded in evidence showing the close connection between oral health and overall health. Coordinating care between these areas is vital for maintaining overall health. Primary care settings offer a valuable opportunity to address oral health by conducting risk assessments, screenings, and preventive measures, and providing guidance, counseling, and referrals to dental professionals [7]. Integrating oral health care into primary care can be achieved through interprofessional education, collaborative practice, closed-loop referral systems, partnerships between public and private sectors, and the inclusion of dental professionals within primary care teams [3].
The Nepalese Constitution recognizes health as a basic human right. Health posts are Nepal's first institutional contact point for basic health services [8]. They are particularly run by auxiliary health workers (AHWs; health assistants [HAs], community medical assistants, auxiliary nurse midwives) with other helping staff. There are no dentists in health posts. Therefore, it is necessary to provide oral health-related training to these staff unless dentists are recruited into the health posts. The success of the training should be evaluated before implementing it. To the best of the author's knowledge, no studies of this nature in Nepal have been published to date. Therefore, this study was done to assess the impact of oral health training on PHC workers in Gandaki Province, Nepal.
2. Methods
2.1. Study Design, Setting, and Eligibility Criteria for Participants
This was a quasi-experimental study conducted among PHC providers (AHWs and public health inspectors [PHIs]) attending the oral health training. A total of 24 healthcare workers from all districts of Gandaki Province participated in the study. In Gandaki Province, there were a total of 18 public health officers/health education administrative officers and 67 paramedics (also known as AHWs, which include nursing staff, lab staff, and pharmacy) and 81 nursing staff [9]. There are a total of 11 districts in the province. Three each from Baglung and Myagdi, and two each from the remaining districts of Gandaki province were selected. All the participants who were present during the training session and who had provided written informed consent were included. The training was provided by the Health Training Center, Pokhara, Nepal. All the expenses of the training were covered by the training center.
The Health Training Center of Gandaki Province sent invitation letters to all health offices across the province's districts, inviting health workers who were working at the local level to participate. Selection criteria included individuals working as permanent primary health workers (PHIs, HAs, senior community medical assistants, community medical assistants, or AHWs). They were instructed to choose three participants from both Baglung and Myagdi and two participants from each of the remaining districts in the Gandaki province. Participants were selected by their respective district health offices.
2.2. Ethical Approval and Consent
The study was conducted following the principles of the Declaration of Helsinki. Ethical approval for this study was obtained from the Institutional Review Committee of Gandaki Medical College (Reference Number: 37/080/081).
2.3. Interventions
Oral health training included topics like oral anatomy, specialization in dentistry, dental caries and its sequelae, teeth hypersensitivity, dentoalveolar abscess, space infection, fluoride, fluoride varnish and its application, gingivitis and periodontitis, brushing and flossing methods, common oral lesion, tobacco and oral cancer, systemic disease and trigeminal neuralgia, common pediatric problems, eruption disorder, traumatic problems, malocclusion, TMJ dislocation, role of diet on oral health. Various dental experts (recommended by the training center) provided training to the participants in the above-mentioned topics for 6 days, in the last week of April 2025. The method of training used a PowerPoint presentation, different tooth models and brushing models, diagnostic instruments (mouth mirror, explorer, a pair of tweezers), fluoride varnish, and videos.
2.4. Evaluation of Intervention
Oral health training was evaluated by assessing the improvements in oral health knowledge (OHK) and practice.
2.5. Overall OHK and Practice Assessment
There were a total of 30 questions for assessing OHK. There were eight questions for oral health practices. The questions were developed by the authors based on the topics to be covered during the training process, which are provided in Appendix A. Each of the 30 multiple-choice questions had a single correct answer. All questions had a binary outcome coded as one for correct and zero for incorrect. Every correct answer in baseline and after 6 days of training was scored as 1, and wrong answers were scored as zero. An overall composite score was then created by adding the individual scores on each question. The highest possible score for OHK was 30 for each individual.
The highest possible score for oral health practices was 7 (question for oral health practices number 5. How often do you change your toothbrush? was not provided a score, as it was only taken at the baseline and not considered in the post-training questionnaire. As the study evaluated the change in practice within 6 days, changing the toothbrush could not be done within this period). The mean score of knowledge was then calculated and then compared between baseline and after training. The percentage change was calculated by subtracting the pretest percentage from the posttest percentage (100 × [baseline mean score-after training score]/baseline score).
There were three questions regarding their previous training related to oral health, any oral health services provided in their workplace, and what services they were providing in their workplace. This questionnaire was filled out at the baseline only.
The questionnaire was filled out by the participants. The researcher checked for the completeness of the questionnaire before collecting the filled questionnaires.
2.6. Validation of the Study Tool
The content validity of the questionnaire was done with five experts, and the content validity index was found to be more than 0.90.
2.7. Masking
No masking was performed as health education was provided to all participants, and there was no control group.
2.8. Statistical Analysis
After completion of the study, data were entered in a Microsoft Excel Sheet version 2013 and analyzed using R 4.3.2 software. The level of significance was set at p < 0.05. The Shapiro–Wilk test was used to check the normality of the data, as the sample is less than 50. A descriptive analysis was performed to summarize the socio–demographic characteristics. Descriptive statistics, including the mean and standard deviations, were computed for OHK. Paired t-test was used to compare the baseline and at the end of training for knowledge and practice scores. The McNemar test was used to compare the percentage of correct responses of OHK before training and after training.
3. Results
All participants completed the study with a 100% response rate and no loss to follow-up. The data distribution was assessed for normality using the Shapiro–Wilk test. Before training, the OHK scores exhibited normal distribution (Shapiro–Wilk test, W = 0.942, p-value = 0.176, as did the OHK scores after training (Shapiro–Wilk test, W = 0.958, p-value = 0.402).
The participants' mean age was 32.04 ± 7.54 years, ranging from 21 to 44 years. Half of the participants were under 30 years old. Two-thirds of the participants were male. Approximately half of the participants had completed HA education. Half of the participants worked as AHWs. Slightly over half of the participants had more than 5 years of work experience (Table 1).
None of the participants had received any prior training related to dental and oral health. More than three-fifths of the participants were involved in providing dental and oral health-related services in their respective areas. Slightly less than half of the participants offered dental counseling and referrals for treatment (Table 2).
The mean OHK at the baseline was 16.83 ± 2.82. This increased by 55.25% to 26.13 ± 2.38 after training, a statistically significant difference (Figure 1).
Out of 30 questions, all participants provided the correct response to only one question, “What are the essential elements for tooth decay?” at baseline. The total responses to 14 questions (QN: 3, 5, 6, 7, 9, 11, 13, 19, 20, 21, 24, 28, 29, 30) showed statistically significant improvement after 6 days of training (Table 3).
Before the training, most participants had good oral hygiene practices. There was a slight improvement in these practices after the training. At baseline, 35.29% were using dental floss among those using interdental aids, while after training, this percentage increased to 86.36% (Table 4).
4. Discussion
4.1. OHK
This study demonstrated that oral health education effectively enhanced OHK among healthcare workers in Gandaki Province. The overall knowledge increased by 55.27%, from 16.88 ± 2.86 to 26.21 ± 2.44. No similar studies have been conducted. However, numerous studies have explored the impact of oral health training on nurses and other healthcare workers. A study conducted in India by Sandhya et al. [10] among primary healthcare workers at primary healthcare centers showed an overall increase in knowledge levels, with a mean difference of 12.56 ± 3.23, which aligns closely with our study findings. Similar results were observed in a study conducted by Bhagia et al. [11] in India.
A study done by Wu et al. [12] in China in 2020 showed that the mean knowledge was significantly improved from 6.58 ± 1.23 to 7.32 ± 0.70 among staff providing long-term care services. A study by Mohebbi et al. [13] in Iran on primary care physicians showed that oral health care knowledge was improved after intervention. Another study conducted in Nigeria by Oladayo et al. [14] among nurses and community health workers also demonstrated an increase in OHK after the training.
The findings from this study suggest that knowledge of oral health among primary healthcare workers can be improved through oral health education.
In rural areas where dental manpower is insufficient, preventive oral health education can be provided to healthcare workers. This enables them to share knowledge with those in need within their communities, aiding in the prevention of dental diseases to some extent.
4.2. Oral Health Practices
The majority of participants already had good oral hygiene practices before the training. The use of interdental aids increased from 70.83% to 91.67%. Before training, 35.29% of participants using interdental aids were using dental floss, which increased to 86.36% after training. Despite already having good oral hygiene practices before training, there was an improvement after training within a very short period of time. This improvement may be attributed to increased OHK. However, the long-term impact on oral hygiene practices should be evaluated.
5. Strengths and Limitations
Health workers from all districts of Gandaki province were included in the study, which enhances its representativeness. However, the use of convenience sampling limits the generalizability of the findings. Additionally, the study did not utilize a separate control group. Social desirability bias is also a potential concern. Furthermore, the study was also of shorter duration, and long-term knowledge retention and practice were not evaluated. Therefore, the results should be interpreted as an assessment of immediate recall rather than long-term retention.
6. Conclusions
The study concluded that oral health education effectively improves OHK and oral hygiene practices in the short term. However, a long-term evaluation of its impact is necessary. If proven effective in the long term, it should be fully implemented, providing oral health education to all healthcare providers in Gandaki Province.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1WHO Oral Health Overview 2024 accessed February 13, 2024, https://www.who.int/health-topics/oral-health#tab=tab_1
- 2WHO Oral Health Key Facts 2024 accessed February 13, 2024, https://www.who.int/news-room/fact-sheets/detail/oral-health
- 3Prasad M. Manjunath C. Murthy A. K. Sampath A. Jaiswal S. Mohapatra A. Integration of Oral Health Into Primary Health Care: A Systematic Review Journal of Family Medicine and Primary Care 201986 p. 183810.4103/jfmpc.jfmpc_286_19PMC 661818131334142 · doi ↗ · pubmed ↗
- 4Walley J. Lawn J. E. Tinker A. Primary Health Care: Making Alma-Ata a Reality The Lancet 200837296421001100710.1016/S 0140-6736(08)61409-92-s 2.0-5124909683618790322 · doi ↗ · pubmed ↗
- 5WHO Draft Global Oral Health Action Plan (2023–2030)2022 accessed February 13, 2024, WHO Discussion Paper, https://cdn.who.int/media/docs/default-source/ncds/mnd/eb 152-draft-global-oral-health-action-plan.pdf
- 6World Health Organization Document A 71/10 Add.1. Seventy-Fifth World Health Assembly. Provisional Agenda Item 14.1. Follow-up to the Political Declaration of the Third High-Level Meeting of the General Assembly on the Prevention and Control of Non-Communicable Disease. Annex 3. Draft Global Strategy on Oral Health 2022 https://apps.who.int/gb/ebwha/pdf_files/WHA 75/A 75_10Add 1-en.pdf
- 7Association of State and Territorial Dental Directors National Maternal and Child Oral Health Resource Center Policy Statement: Integrating Oral Health Care into Primary Care 2024 accessed August 14, 2024, https://www.astdd.org/docs/integrating-oral-health-care-into-primary-care.pdf
- 8Government of Nepal Ministry of Health and Population Nepal Health Facility Survey 2021 Final Report 2021 accessed February 13, 2024, https://www.dhsprogram.com/pubs/pdf/SPA 35/SPA 35.pdf