The Diagnostic Pitfalls and Clinical Challenges of Unilateral Facial Paralysis in Acute Demyelinating Disorders: A Case Report and Literature Review
Thamer S. Alhowaish, Hossam Ali Alqahtani, Moustafa S. Alhamadh, Ali Alanazi

TL;DR
This case report highlights the diagnostic challenges of Guillain–Barré syndrome when it presents with unilateral facial paralysis, which can resemble Bell's palsy.
Contribution
The paper presents a rare case of GBS with unilateral facial palsy and emphasizes the importance of considering GBS in atypical cranial neuropathy presentations.
Findings
Unilateral facial palsy can be an atypical presentation of Guillain–Barré syndrome.
Early diagnosis of GBS is crucial and can be supported by cerebrospinal fluid analysis and electrodiagnostic studies.
Treatment with intravenous immunoglobulin led to significant clinical improvement in the reported case.
Abstract
Guillain–Barré syndrome (GBS) is an acute immune-mediated polyradiculoneuropathy typically presenting with progressive limb weakness and areflexia, while bilateral facial nerve involvement is a well-recognized feature. However, unilateral facial palsy is exceedingly rare and can closely mimic Bell's palsy, complicating early diagnosis. We report the case of a previously healthy 32-year-old man whose illness began with subtle bilateral fingertip numbness ascending to his elbows, followed by the acute onset of right-sided facial weakness, perioral numbness, slurred speech, and inability to close his right eye. These symptoms developed shortly after an upper respiratory tract infection and were soon accompanied by toe numbness and gait unsteadiness. Examination revealed isolated right lower motor neuron facial palsy and a rapid progression from diminished to absent deep tendon reflexes,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
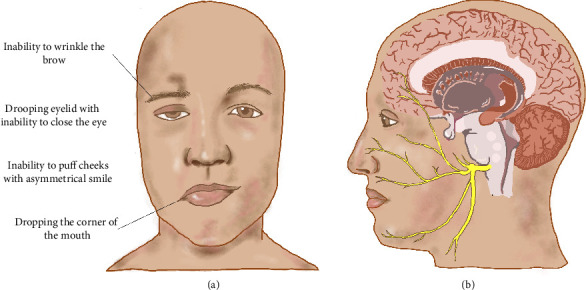 Figure 1
Figure 1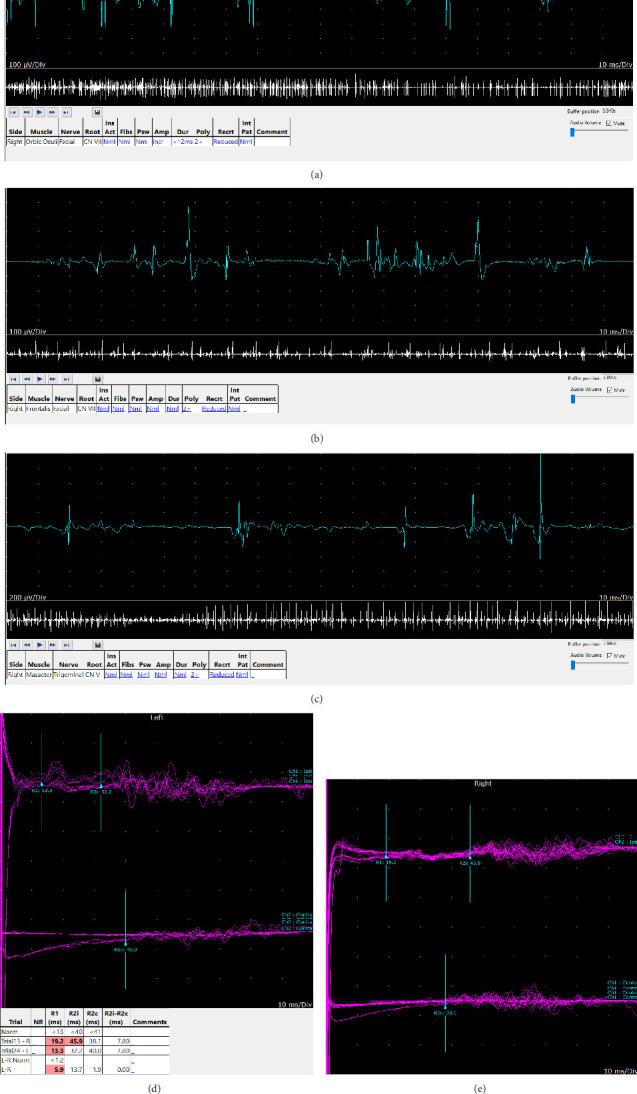 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPeripheral Neuropathies and Disorders · Facial Nerve Paralysis Treatment and Research · Infectious Diseases and Tuberculosis
1. Introduction
Guillain–Barré syndrome (GBS) is an acute demyelinating disorder that presents in the classic form of muscle weakness and absent reflexes [1]. A rare variant of GBS includes facial paresthesia and bilateral facial weakness. Because of these atypical manifestations, it is occasionally challenging to diagnose GBS when it presents with this rare variant [2–4]. In general, bilateral facial nerve palsy is rare, with an incidence of only 1 per 5,000,000 population, and only 20% of the cases are idiopathic [5]. A study of 43 patients with bilateral facial nerve palsy found that 10 cases were attributed to Bell's palsy, and five were due to GBS [6]. This variant of GBS typically manifests by numbness in the limbs, followed by bilateral facial nerve palsy. Interestingly, in rare cases, GBS also presents with unilateral facial weakness that is difficult to distinguish from Bell's palsy [2–4, 7]. The pathology of unilateral facial palsy in GBS involves immune-mediated nerve damage, leading to demyelination or axonal injury of the facial nerve. While facial involvement in GBS is typically bilateral, an asymmetric immune response can result in unilateral facial palsy due to localized inflammation [8, 9].
Here, we report a case of a rare variant of GBS with unilateral facial weakness and paresthesia.
2. Case Report
2.1. History of Presenting Illness
A 32-year-old male, not known to have a previous medical history, presented to the emergency department complaining of right-sided facial weakness with perioral numbness for two days. The symptoms started with numbness in the fingertips bilaterally that progressed to the elbows. One week later, he developed slurred speech, facial deviation on the right side, and an inability to close the right eye (Figure 1). Three days later, he developed numbness in his toes associated with unsteadiness. The symptoms were persistent since their onset and had never occurred before. The patient had upper respiratory tract infection (URTI) symptoms 10 days prior to the onset of his neurological symptoms. He denied any earache, hearing difficulty, tinnitus, recent trauma to the head or neck, or weakness in other parts of the body. There was no history of skin rash, tick bite in the past, promiscuous sexual behavior, or use of any herbal supplements.
2.2. Clinical Examination
The patient remained hemodynamically stable with normal vital signs. Neurological assessment revealed intact cranial nerves except for right lower motor neuron-type facial weakness (e.g., ipsilateral forehead involvement). Motor examination demonstrated normal tone and strength in all limbs without muscle atrophy. Deep tendon reflexes were globally diminished at admission, progressing to areflexia (brachioradialis, biceps, triceps, patellar, and Achilles tendons) by day 6. Plantar responses were flexor bilaterally. Sensory testing showed intact light touch, pinprick, vibration, and proprioception in all extremities. Cerebellar function including finger-to-nose, heel-to-shin, and rapid alternating movements was normal without dysmetria or intention tremor.
2.3. Investigation
Basic laboratory tests were unremarkable except for polycythemia; chest radiographs were normal. Magnetic resonance imaging (MRI) of the brain with gadolinium administration revealed smooth enhancement in the right internal auditory canal and the right geniculate ganglion. Examination of the cerebrospinal fluid (CSF) showed high protein 0.61 g/L (normal range 0.15–0.40 g/L) and a normal range of white blood cells (WBCs) (Table 1). A nerve conduction study (NCS) and blink reflex were performed 2 weeks after the onset of his symptoms which showed a picture of right carpal tunnel syndrome but otherwise unremarkable findings.
To rule out other possible causes of his neurological symptoms, further tests were performed. Cytologic examination of the CSF revealed a few lymphocytes with no malignant cells. Vitamin B12 level was normal. Antibodies to human immunodeficiency virus (HIV), Epstein–Barr virus (EBV), Cytomegalovirus (CMV), and EBV early antigen were negative. Blood and CSF cultures were negative. A stool culture was not performed. Analysis of anti-glycolipid antibodies was negative (Table 2).
2.4. Management and Outcome
On the 5th day of admission, he was started on intravenous immunoglobulin (IVIG), 0.4 g/kg/day, for five days along with occupational and physical therapy.
The patient was discharged with a diagnosis of atypical GBS. At the 2-week follow-up in the clinic, the facial weakness improved significantly. However, the patient complained of perioral numbness and bilateral upper limbs, up to the elbow, and feet numbness. Also, he had decreased pinprick sensation on the right side over the mandibular nerve distribution, and he remained areflexic all over the body.
Three months later, at follow-up, NCS, electromyography (EMG), and blink reflex were performed (Table 3). NCS showed a picture of right median neuropathy, consistent with the previous test. Blink reflexes showed features consistent with right facial neuropathy. Needle EMG of muscles innervated by the facial and trigeminal nerves (frontalis, orbicularis oculi, and masseter) bilaterally demonstrated mild denervation changes as well as chronic neurogenic changes (Table 4 and Figure 2).
The patient underwent multiple follow-up evaluations in the neurology clinic, with the most recent visit occurring 22 months postdischarge. At that time, he had returned fully to his neurological baseline, with complete resolution of facial asymmetry. His only complaint was intermittent tingling sensations in the left arm, which were not associated with any objective neurological deficits. A comprehensive neurological examination was unremarkable, and deep tendon reflexes were symmetrically preserved as 2+ throughout.
3. Discussion
In this article, we shared our experience in diagnosing and managing a variant of GBS. Initially, our patient came with unilateral facial weakness and paresthesia following an URTI, because of which he was diagnosed as a case of unilateral Bell's palsy. However, he developed areflexia throughout the body, for which he underwent lumbar puncture and neurophysiological studies (NCS, EMG, and blink reflexes) that showed albumin-cytological dissociation and evidence of facial and trigeminal neuropathy, respectively. The diagnosis of variant GBS with unilateral facial nerve palsy was made based on the clinical examination, CSF analysis, and neurophysiological studies. Treatment of GBS includes supportive measures and disease-modifying therapies such as IVIG or plasma exchange [2]. Our patient responded well to IVIG and had a significant neurological improvement on follow-up visits. While facial weakness can emerge following the resolution of Miller Fisher syndrome (MFS), our patient had no history of diplopia, and the clinical examination showed neither ophthalmoparesis nor ataxia, making the diagnosis of MFS unlikely [9–11].
GBS is classically recognized as a postinfectious polyneuropathy that typically presents with acute lower limb weakness [12]. While this hallmark presentation is well documented, cranial nerve involvement particularly of the facial nerve is also not uncommon feature [7]. When facial involvement occurs, it is characteristically bilateral and often accompanied by distal limb paresthesia or weakness [13]. Interestingly, isolated facial diplegia represents a rare GBS variant, and cases presenting with unilateral facial weakness are exceedingly uncommon, with only a few cases described so far [2, 8] (Table 5). In some reported cases, the weakness started unilaterally and progressed to bilateral facial involvement. However, in our case, it started as and continued to be unilateral while the neurophysiological studies showed evidence of bilateral facial involvement. GBS typically presents with symmetrical neurological deficits; some may question why, in rare cases, facial palsy appears unilaterally such as on the right side rather than the left. While the precise reason remains unclear, several anatomical, immunological, and physiological factors may contribute to this paradoxical presentation. The proposed mechanism involves asymmetric integrity of the blood-nerve barrier (BNB); a more intact BNB on the clinically unaffected side may restrict the infiltration of pathogenic antibodies (e.g., anti-ganglioside antibodies such as GM1) and inflammatory cells, thereby preventing overt clinical symptoms. In contrast, a compromised BNB on the affected side may allow immune-mediated demyelination or axonal injury. Neurophysiological studies often reveal bilateral abnormalities, suggesting subclinical involvement even on the asymptomatic side [8, 9]. Additionally, uneven antigen exposure from prior infections might lead to antibodies targeting specific nerve segments unilaterally, influenced by variations in ganglioside distribution or localized nerve injury [26]. Furthermore, the facial nerve's anatomical pathway through the narrow fallopian canal makes it particularly susceptible to inflammation-induced compression (Figure 1). Asymmetric edema within this confined space may precipitate unilateral facial palsy despite underlying bilateral nerve involvement [8, 26]. These factors collectively illustrate how GBS can present with unilateral facial weakness, highlighting the importance of thorough diagnostic evaluation including NCSs and CSF analysis to ensure accurate diagnosis, particularly in atypical presentations.
The cranial nerves' involvement and enhancement on MRI can be observed in GBS. This was noted in our case as well as in Sharma's case report and Zuccoli's study [16, 27]. Facial nerve enhancement on MRI is observed in both GBS and Bell's palsy but differs in pattern and clinical context. In GBS, enhancement is often bilateral and may involve multiple cranial nerves, reflecting diffuse demyelination and BNB disruption [28]. In contrast, Bell's palsy typically shows unilateral enhancement, most commonly in the labyrinthine segment of the facial nerve, due to localized viral neuritis [29]. While MRI findings may overlap, diffuse or bilateral enhancement supports a diagnosis of GBS, whereas isolated, unilateral enhancement favors Bell's palsy. Thus, clinical correlation remains essential for accurate differentiation.
Deep tendon reflexes are generally absent or diminished. Rare cases without hypo/areflexia have been described, mostly in the acute motor axon neuropathy variant of GBS [6, 30, 31]. In our patient, the reflexes of the upper and lower limbs were absent. A history of infection within four weeks before the onset of neurologic symptoms is found in many patients, and most of them have evidence of demyelination in their limbs on NCS [7, 13]. In the early stages of GBS, neurophysiological assessments such as NCSs may yield negative or inconclusive results. This diagnostic limitation arises from different pathophysiological factors. First, during the initial ≤ 7 days of the disease, the autoimmune response predominantly targets proximal nerve roots and nodes of Ranvier, leading to inflammatory edema and reversible conduction block rather than overt demyelination or axonal injury. Consequently, key electrophysiological parameters such as motor and sensory conduction velocities and compound muscle action potential amplitudes often remain within normal limits until more permanent structural damage, like Wallerian degeneration, emerges typically after 1-2 weeks. Second, early lesions in GBS frequently involve proximal nerve segments, such as spinal roots, which are not readily evaluated by conventional distal-focused NCS techniques. As a result, early diagnostic sensitivity is reduced, underscoring the importance of clinical judgment and potential adjunctive testing in the early phase of GBS [32–34]. The guidance outlined in the paper “Diagnosis and Management of Guillain–Barré Syndrome in Ten Steps” underscores the diagnostic challenges in early GBS. It emphasizes that both CSF analysis and electrophysiological studies may produce normal or inconclusive results in the initial stages of the disease, thereby necessitating serial testing to capture evolving pathological changes. The paper also highlights the need for heightened clinical awareness of atypical presentations, which may not conform to classic GBS features at onset. Importantly, it reinforces current treatment guidelines by prioritizing IVIG or plasma exchange as first-line therapies, while advising against the use of corticosteroids due to their lack of efficacy and potential to adversely affect recovery [35].
The use of corticosteroids in the treatment of GBS has been a controversial subject and remains a fertile ground of ongoing research. Historically, corticosteroids have been used to reduce inflammation, impede disease progression, and potentially expedite recovery of GBS. However, recent evidence suggests that their efficacy might be limited, and in some cases, they might exacerbate the disease instead [36, 37]. To clarify, randomized controlled trials evaluating the efficacy of corticosteroids in the treatment of GBS revealed no significant benefit; instead, these trials showed that the use of oral corticosteroids worsened GBS outcomes [35, 38]. Because of that, contemporary treatment guidelines for GBS generally recommend against the routine use of corticosteroids [10]. In our case, corticosteroid therapy was initially withheld due to significant diagnostic uncertainty. The patient's presentation, characterized by isolated facial nerve involvement with preserved reflexes and no evidence of limb weakness, ascending paralysis, or autonomic dysfunction, was more suggestive of Bell's palsy or another focal cranial neuropathy than Guillain–Barré syndrome. However, atypical features such as perioral and distal limb paresthesias raised concerns for an alternative diagnosis, warranting caution with corticosteroid use. While steroids are used in Bell's palsy, they are not indicated in GBS. Therefore, corticosteroid administration was deferred due to clinical ambiguity and to allow for further diagnostic evaluation. Ultimately, the evolution of symmetrical areflexia by day six confirmed the diagnosis of GBS. Reflex changes, a hallmark of GBS, often emerge after the onset of motor symptoms, reinforcing the importance of clinical vigilance. Following this diagnostic clarification, GBS-specific treatment was initiated using IVIG. IVIG was selected in this case over plasma exchange due to its similar efficacy, simpler administration, better safety profile, and greater accessibility [35, 39, 40].
GBS with unilateral facial nerve involvement can mimic Bell's palsy, leading physicians to mistakenly administer corticosteroids, which may exacerbate GBS symptoms. Our case, in addition to five published reports, exemplifies the previous scenario, in which Bell's palsy was initially presumed. These five cases initially received corticosteroids for suspected Bell's palsy as shown in Table 5. Distinguishing between Bell's palsy and facial nerve palsy as part of GBS can pose a diagnostic challenge. Bell's palsy presents with an acute onset of one-sided facial nerve palsy, reaching its peak severity in less than 3 days and insidiously resolving over weeks [11]. It often follows a viral infection, particularly herpes simplex virus type 1 and varicella-zoster virus [41]. On the other hand, facial nerve involvement in GBS typically manifests bilaterally, either simultaneously with or preceding the onset of ascending paralysis and paresthesia. This manifestation occurs 1-2 weeks after URTI or gastroenteritis, reaching its peak severity in 2–4 weeks and insidiously subsiding over months to years [42]. In the absence of limb weakness, the presence of high protein levels in the CSF and antiganglioside antibodies helps to distinguish facial nerve involvement in GBS from Bell's palsy [43].
Table 5 summarizes the reported cases of GBS with unilateral facial nerve involvement. We found a total of 23 GBS cases with unilateral facial nerve involvement. The mean age was 33.3 ± 22.9 years (the mean age among adult cases was 44.7 and that among pediatric cases was 7 years), with almost equal gender distribution (12 females and 11 males). Most of the affected patients were healthy with no comorbidities. The majority of the cases were triggered or presumed to be triggered by a respiratory infection or gastroenteritis. More than half (56.5%; n = 13) of the reported cases had evidence of bulbar palsy in addition to facial nerve involvement. More than 90% of the cases had diminished or absent deep tendon reflexes. Among the cases where CSF examination was performed, more than two-thirds (68.4%, n = 13) demonstrated albuminocytologic dissociation, defined as elevated CSF protein (> 45 mg/dL) with a total cell count of ≤ 10/mm^3^ [44], and two patients (10.5%) had high protein and slightly elevated WBCs (> 10 and < 20/mm). MRI was negative in almost all cases. IVIG was given for almost three-quarters (73.9%; n = 17) of the patients, and some patients received adjunctive therapies such as antiviral therapy. Almost all cases reported a good response to treatment with almost complete recovery; the exception is a 66-year-old female, who was admitted for COVID-19 infection and developed GBS with facial nerve involvement. This patient deteriorated and was admitted to the intensive care unit for respiratory support with multiorgan failure, deep vein thrombosis, and superimposed bacterial infection despite early IVIG and antiviral therapy. Corticosteroids were administered to 5 patients, mainly for presumed Bell's palsy. These patients later received IVIG, and all made a full recovery or had mild residual weakness at the follow-up visit. Our case shares several key features with the 23 previously reported cases of GBS presenting with unilateral facial nerve involvement. Similar to the majority of those cases, our patient was a previously healthy young adult who developed symptoms shortly after an URTI, reinforcing the role of postinfectious immune response as a trigger. The clinical course in our patient also included diminished-to-absent deep tendon reflexes and albuminocytologic dissociation on CSF analysis findings consistent with over 90% and two-thirds of the previously reported cases, respectively. IVIG, which was the most commonly used treatment among the reviewed cases, also resulted in a favorable outcome in our patient. However, our case is distinct in its initial presentation with right facial palsy with perioral numbness, rapidly evolving into broader areflexia without motor weakness, features that added diagnostic complexity. Unlike most prior cases, where bulbar involvement was common (56.5%), our patient did not exhibit bulbar dysfunction. These similarities and differences underscore the heterogeneity of GBS presentations and highlight the need for heightened clinical suspicion in atypical cranial neuropathies.
The disease typically reaches its nadir by 2 weeks in most cases and in 4 weeks in nearly all, after which recovery begins first proximally then distally over weeks or months [13]. Despite a good clinical recovery, many patients exhibit residual weakness and loss of motor units, which likely contributes to the persistent fatigue common in GBS. Early diagnosis and a multidisciplinary rehabilitation program are crucial for improving outcomes. Preclinical studies show that early physical exercise, including active exercise and electrical stimulation, promotes axonal regeneration, prevents maladaptive responses, and upregulates genes linked to neuronal plasticity in both the spinal cord and skeletal muscle. For example, a 12-week study by Chiaramonte et al. demonstrated that bicycle exercise training in GBS patients with severe fatigue was well tolerated and led to marked reductions in fatigue, along with improvements in physical fitness, functional outcomes, and quality of life [45, 46].
This case presents a compelling and educational contribution to medical literature, particularly in the field of neurology, for several key reasons. First, it underscores the critical importance of maintaining a high clinical suspicion for GBS, especially when encountering patients with acute onset unilateral facial weakness, an atypical but possible presentation, particularly when preceded by an infectious illness. Often misattributed to more common conditions such as Bell's palsy, such presentations highlight the necessity of clinicians being familiar with the atypical variants of GBS. Early recognition in these cases allows for prompt and appropriate investigation and treatment, which can significantly impact patient outcomes. Our patient's marked improvement with medical therapy not only reinforces the value of accurate diagnosis but also emphasizes the potential to avoid unnecessary tests and delays in care. Unilateral facial palsy as an initial manifestation of GBS remains rare, as most cases traditionally involve bilateral facial weakness, making this case notable. By drawing attention to this uncommon variant, we aim to broaden the clinical perspective and encourage heightened diagnostic vigilance. This report contributes meaningfully to neurology by bridging a crucial gap in the understanding of GBS presentations, refining diagnostic approaches, and reinforcing the importance of evidence-based management in improving patient outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Lewis R. Arcila-Londono X. Guillain-Barré Syndrome Seminars in Neurology 2012320317918610.1055/s-0032-13291962-s 2.0-8486824494723117942 · doi ↗ · pubmed ↗
- 2Nishiguchi S. Branch J. Tsuchiya T. Ito R. Kawada J. Guillain-Barré Syndrome: A Variant Consisting of Facial Diplegia and Paresthesia With Left Facial Hemiplegia Associated With Antibodies to Galactocerebroside and Phosphatidic Acid American Journal of Case Reports 2017181048105210.12659/ajcr.9049252-s 2.0-8503084500928966341 PMC 5633102 · doi ↗ · pubmed ↗
- 3Mori M. Kuwabara S. Fukutake T. Yuki N. Hattori T. A Variant of Guillain-Barré Syndrome With Prominent Bilateral Peripheral Facial Nerve Palsy: Facial Diplegia and Paresthesias Rinsho Shinkeigaku 2004441174074415471093 · pubmed ↗
- 4Susuki K. Koga M. Hirata K. Isogai E. Yuki N. A Guillain-Barré Syndrome Variant With Prominent Facial Diplegia Journal of Neurology 2009256111899190510.1007/s 00415-009-5254-82-s 2.0-7344914842519633904 · doi ↗ · pubmed ↗
- 5Kumar P. Charaniya R. Bahl A. Ghosh A. Dixit J. Facial Diplegia With Paresthesia: An Uncommon Variant of Guillain–Barré Syndrome Journal of Clinical and Diagnostic Research 2016107 OD 01OD 0210.7860/jcdr/2016/19464.8128 PMC 502019727630886 · doi ↗ · pubmed ↗
- 6Sardar S. Sasi S. Menik Arachchige S. Zahid M. Melikyan G. Isolated Facial Diplegia: A Rare Presentation of Guillain-Barré Syndrome Clinical Case Reports 202197 p. e 447310.1002/ccr 3.4473 PMC 829908634322247 · doi ↗ · pubmed ↗
- 7Ropper A. H. Further Regional Variants of Acute Immune Polyneuropathy Archives of Neurology 199451767167510.1001/archneur.1994.005401900510142-s 2.0-00282274078018039 · doi ↗ · pubmed ↗
- 8Verma R. Chaudhari T. S. Giri P. Unilateral Facial Palsy in Guillain-Barre Syndrome (GBS): A Rare Occurrence BMJ Case Reports 20122012 p. bcr 201200707710.1136/bcr-2012-0070772-s 2.0-84872165746 PMC 454430923087283 · doi ↗ · pubmed ↗