Cardiac Angiosarcoma: A Diagnostic and Therapeutic Challenge
Kang Ying Tan, Yi‐Chang Liu

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
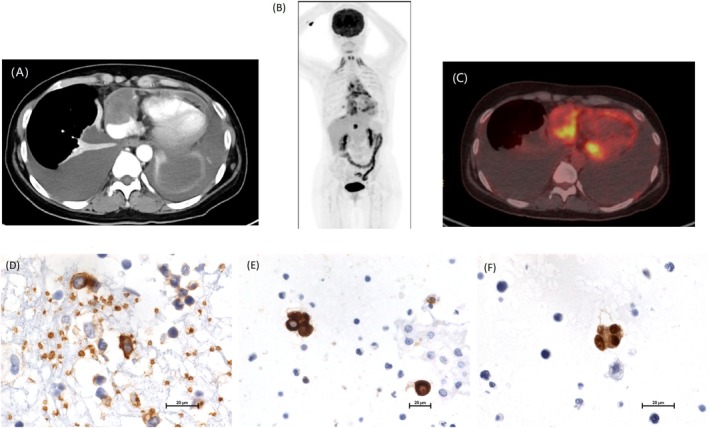 FIGURE 1
FIGURE 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac tumors and thrombi · Vascular Tumors and Angiosarcomas · Vascular Malformations and Hemangiomas
Dear Editor,
1
Primary cardiac angiosarcoma is a rare and highly aggressive neoplasm, accounting for less than 0.1% of all cardiac tumors. Due to the difficulty of approaching it, timely diagnosis and management are challenging. Here we report a case of primary cardiac angiosarcoma; the diagnosis was impressed after a series of investigations.
A 42‐year‐old woman presented with progressive dyspnea for 4 months. Initial investigations revealed pericardial and pleural effusions. Laboratory testing showed elevated anti‐Ro antibodies and positive anti‐connective tissue disease (CTD) serologies, raising suspicion for autoimmune disease‐related effusions. Empirical treatment with corticosteroids and leflunomide was initiated; however, no clinical improvement was observed. Repeat thoracentesis revealed atypical cells, and subsequent computed tomography (CT) imaging identified a mass involving the right atrium and pericardium (Figure 1A). Positron emission tomography‐computed tomography (PET‐CT) demonstrated fluorodeoxyglucose (FDG) uptake in the cardiac sinus and mediastinal lymph nodes (Figure 1B,C). Due to the patient's poor performance status and signs of advanced heart failure, cardiac biopsy was not feasible. Further cytologic analysis of pleural fluid supported the diagnosis of angiosarcoma, with immunohistochemistry positive for cytokeratin (CK), CD31, and ERG (Figure 1D–F).
Computed tomography (CT) showed a tumor involving the right pericardium and right atrium (A). Positron emission tomography (PET) scan showed cardiac sinus infiltration and fluorodeoxyglucose (FDG) uptake in mediastinal lymph nodes (B and C). Pleural Fluid cytology immuohistochemical stains showed CK(+) (D), CD31(+) (E) and ERG(+) (F).
The patient received chemotherapy with doxorubicin and ifosfamide, but severe pancytopenia complicated by pneumonia and septic shock developed later. The treatment was then switched to cabozantinib and nivolumab; however, no tumor shrinkage was observed, with worsening effusions. A final attempt with gemcitabine and docetaxel was interrupted by respiratory failure, and the patient passed away 8 months after the initial symptom onset.
This case underscores the diagnostic challenge posed by cardiac angiosarcomas, especially in the context of overlapping autoimmune features. While imaging and cytology aid in diagnosis, tissue confirmation remains critical. Currently, no established link between autoimmune disease and cardiac angiosarcoma exists; only sparse pieces of literature focusing on autoimmune phenomena associated with sarcoma are reported [1, 2, 3].
Therapeutic options for unresectable cardiac angiosarcoma are quite limited. Although immunotherapy like cabozantinib and nivolumab combination has shown promise in other angiosarcoma subtypes [4], our patient did not benefit. Tumor location and subtype may influence response, with cardiac sarcomas possibly demonstrating lower immunogenicity [5].
In conclusion, this case highlights the need for early diagnostic interventions in unexplained recurrent pericardial effusion and emphasizes the urgency for developing effective targeted and immunotherapeutic treatments for cardiac angiosarcoma.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1J. Wen , H. Ouyang , R. Yang , et al., “Malignancy Dominated With Rheumatic Manifestations: A Retrospective Single‐Center Analysis,” Scientific Reports 8, no. 1 (2018): 1786.29379092 10.1038/s 41598-018-20167-w PMC 5789019 · doi ↗ · pubmed ↗
- 2N. Ung , C. Gunasingam , K. Cai , et al., “Cardiac Sarcoma Presenting as Paraneoplastic Arthritis and Clubbing: A Case Report and Literature Review,” BMC Rheumatology 7, no. 1 (2023): 30.37715284 10.1186/s 41927-023-00350-x PMC 10503070 · doi ↗ · pubmed ↗
- 3A. Vlagea , S. Falagan , G. Gutierrez‐Gutierrez , et al., “Antinuclear Antibodies and Cancer: A Literature Review,” Critical Reviews in Oncology/Hematology 127 (2018): 42–49.29891110 10.1016/j.critrevonc.2018.05.002 · doi ↗ · pubmed ↗
- 4J. E. Grilley‐Olson , J. B. Allred , S. Schuetze , et al., “A Multicenter Phase II Study of Cabozantinib + Nivolumab for Patients (Pts) With Advanced Angiosarcoma (AS) Previously Treated With a Taxane (Alliance A 091902),” Journal of Clinical Oncology 41 (2023): 11503.
- 5A. H. Nassar , E. El‐Am , R. Denu , et al., “Clinical Outcomes Among Immunotherapy‐Treated Patients With Primary Cardiac Soft Tissue Sarcomas: A Multicenter Retrospective Study,” JACC Cardio Oncology 6, no. 1 (2024): 71–79.38510282 10.1016/j.jaccao.2023.11.007PMC 10950431 · doi ↗ · pubmed ↗