Atypical Manifestation of Giardiasis: Exocrine Pancreatic Insufficiency in a Young Adult
Julio E Sanchez Gonzalez, Aymara Fernandez de la Vara

TL;DR
A young adult with chronic diarrhea was found to have giardiasis causing exocrine pancreatic insufficiency, highlighting the need for broader diagnostic approaches.
Contribution
This case highlights a rare but treatable link between giardiasis and exocrine pancreatic insufficiency in adults.
Findings
Giardia lamblia can cause reversible exocrine pancreatic insufficiency in adults without intrinsic pancreatic disease.
Multiplex PCR stool testing improves detection of Giardia compared to standard antigen testing.
Pancreatic enzyme replacement and tinidazole treatment resolved symptoms in this case.
Abstract
Diagnosing the underlying cause of chronic diarrhea in adults can be complex, especially when routine evaluations yield no clear etiology. Although Giardia lamblia is a common pathogen, its role in triggering secondary complications such as exocrine pancreatic insufficiency (EPI) is rarely recognized. Increased awareness of this association is crucial as newer diagnostic tools become more accessible in outpatient settings. We report a case of a 22-year-old male with five months of persistent watery diarrhea and abdominal discomfort following a course of clindamycin. Initial laboratory and stool studies were unrevealing, but fecal elastase-1 levels were severely reduced, consistent with EPI. The patient showed partial improvement with pancreatic enzyme replacement and cholestyramine. A multiplex polymerase chain reaction (PCR) stool panel later identified Giardia lamblia, and treatment…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
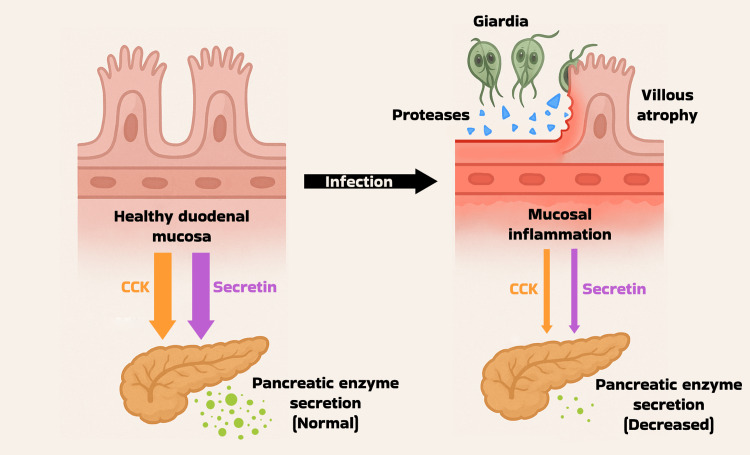 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsParasitic Infections and Diagnostics · Amoebic Infections and Treatments · Gastrointestinal disorders and treatments
Introduction
Persistent diarrhea in young, otherwise healthy adults is a common but often diagnostically challenging complaint [1]. While infectious causes are frequently implicated, standard testing may fail to reveal an etiology, particularly in cases of chronic or relapsing symptoms [1]. Giardiasis, caused by the protozoan Giardia lamblia, is a leading parasitic cause of diarrheal illness worldwide, yet its chronic manifestations and extraintestinal complications, including reactive arthritis and urticaria, remain poorly recognized [2]. Emerging literature suggests a potential association between prolonged Giardia infection and reversible exocrine pancreatic insufficiency (EPI), a relationship that may be overlooked when diagnostic focus remains limited to either gastrointestinal pathogens or pancreatic disease alone [3]. Recognizing this interplay is essential for timely diagnosis and appropriate management, especially as multiplex molecular diagnostics and noninvasive pancreatic testing become more widely available in primary care and outpatient settings [4]. This report illustrates how integrating these tools can improve diagnostic accuracy and clinical outcomes in patients with unexplained, treatment-refractory diarrhea.
Case presentation
A 22-year-old male with no significant past medical history presented to an outpatient primary care clinic with persistent diarrhea and abdominal pain for five months. Shortly before symptom onset, he was treated with a course of clindamycin for a piercing site infection. The patient reported that his usual bowel habits consisted of one to two daily movements, but the frequency had increased to up to six per day. He described his stools as being yellow to brown in color, with a liquid consistency. The patient also noted experiencing dull, diffuse, non-radiating abdominal pain, increased flatulence, and a strong urge to defecate within thirty minutes after meals, without any specific food triggers. In an attempt to alleviate his symptoms, the patient began using probiotics and eliminated acidic and spicy foods from his diet; however, these measures provided no relief. He denied any other significant dietary modifications in the past year, recent international travel, known food or medication allergies, or other exposure risks such as caring for children or eating at new restaurants. He had no past surgical history and was not taking any medications, vitamins, or herbal supplements. The patient also denied experiencing hematochezia, melena, bloating, nausea, vomiting, fever, chills, or any changes in weight since the onset of diarrhea.
On initial evaluation, the patient’s vital signs were temperature 36.6°C, heart rate 65 beats/minute, respiratory rate 16 breaths/minute, blood pressure 117/62 mmHg, oxygen saturation 97% on room air, and body mass index of 22.9. The physical exam showed a well-appearing, cooperative young male in no acute distress, with no signs of dehydration. The abdomen was soft, non-tender, and non-distended, with no guarding, rebound tenderness, or palpable masses. Bowel sounds were normoactive in all four quadrants, and there was no hepatosplenomegaly. The remainder of the physical exam was unremarkable. Initial laboratory studies, including complete blood count, comprehensive metabolic panel, thyroid function tests, iron studies, amylase, and lipase, were all within normal limits. Additionally, infectious and gastrointestinal workups revealed negative results for fecal leukocyte stain, fecal calprotectin, Clostridioides difficile toxin B, Giardia lamblia antigen, Helicobacter pylori antigen, ova and parasites, and HIV. Over the following week, the patient continued to experience persistent watery diarrhea without associated weight loss. Further tests were conducted to evaluate alternative etiologies. Serum tissue transglutaminase immunoglobulin A (IgA) and total IgA levels were both within normal limits, thereby reducing the likelihood of celiac disease. However, fecal pancreatic elastase-1 was severely decreased at <15 mcg/g (normal: >200 mcg/g). Micronutrient evaluation was performed, which showed that levels of vitamins A, E, and K were within normal limits. In contrast, vitamin B12 was decreased at 178 pg/mL (reference range: 200-900 pg/mL), and 25-hydroxyvitamin D was also reduced at 26 ng/mL (reference range: 30-100 ng/mL); therefore, supplementation was initiated.
Subsequently, the patient was evaluated by an outpatient gastroenterologist. Repeat fecal pancreatic elastase-1 testing confirmed persistently decreased levels at 48.3 mcg/g (normal: >200 mcg/g), consistent with severe pancreatic insufficiency. Treatment was initiated with pancrelipase at a dose of 40,000-126,000 units, administered as two capsules with each meal, along with cholestyramine 4 g once daily. Two weeks later, the patient reported a marked improvement in stool consistency and a decreased frequency of bowel movements; however, intermittent diffuse abdominal pain persisted. A CT scan of the abdomen and pelvis with and without contrast revealed no acute intra-abdominopelvic pathology. A Quality Diagnostics (QDx) Complete Stool Pathogen Panel (14-target multiplex polymerase chain reaction (PCR) assay) was ordered to investigate potential infectious causes and was positive for Giardia lamblia. The patient was prescribed tinidazole 500 mg, four tablets as a single dose, for treatment of giardiasis. At the outpatient primary care follow-up visit one week later, the patient reported complete resolution of diarrhea and overall improvement in gastrointestinal comfort, including a reduction in abdominal cramping and bloating. The patient was advised to continue monitoring symptoms and follow up as needed, with a plan for ongoing management of pancreatic enzyme replacement therapy. However, several weeks later, the patient experienced a recurrence of altered bowel habits, although less severe than prior to treatment. A colonoscopy was performed and found to be unremarkable. At the time of reporting, the gastroenterologist was planning to repeat fecal elastase testing to further evaluate the persistence of EPI following eradication of Giardia.
Discussion
This case describes a rare presentation of EPI in an otherwise healthy adult following a confirmed Giardia lamblia infection. Giardia lamblia is the causative agent of giardiasis, one of the most common intestinal protozoan infections worldwide. In high-income nations, the prevalence of the condition is around 2-7%, while in low- and middle-income countries, it can reach as high as 20-30% [2]. Transmission occurs via the fecal-oral route, frequently through contaminated water sources, food, or close interpersonal contact, particularly in daycare settings with suboptimal hygiene [2]. Clinically, giardiasis spans a broad spectrum: some develop acute symptoms such as watery diarrhea, abdominal cramps, bloating, and excessive flatulence, while others exhibit chronic manifestations, including steatorrhea, weight loss, fatigue, and micronutrient deficiencies [5]. Children are especially vulnerable; chronic infections are often asymptomatic but can result in long-term effects such as growth stunting and cognitive delays [5].
Although Giardia lamblia primarily colonizes the proximal small intestine, persistent infection can profoundly disrupt the intestinal environment well beyond mechanical injury. Giardia trophozoites secrete proteases such as giardipain-1 that degrade tight junctions, leading to villous atrophy, increased epithelial apoptosis, and chronic duodenal inflammation [6]. These histological changes, including shortening of brush-border microvilli, crypt hyperplasia, and increased intraepithelial lymphocytic infiltration, undermine mucosal integrity, compromise brush-border enzyme activity, and impair nutrient absorption [7]. Importantly, epithelial injury reduces the release of key enteroendocrine hormones, such as cholecystokinin (CCK) and secretin, which are secreted by I-cells and S-cells in the duodenal mucosa [8]. These hormones are critical for stimulating pancreatic exocrine function; thus, their suppression can result in transient EPI in the absence of intrinsic pancreatic pathology. Figure 1 illustrates the proposed mechanism by which Giardia lamblia disrupts enteroendocrine signaling and contributes to EPI. Observational data in patients with celiac disease further support this mechanism, demonstrating that duodenal injury is associated with reduced pancreatic enzyme output, which improves following mucosal recovery [9]. Additionally, chronic inflammation may provoke ductal edema and intermittently obstruct ampullary outflow, further impeding enzyme delivery [10]. While the precise pathophysiological mechanisms underlying Giardia-associated pancreatic dysfunction remain incompletely understood, emerging reports suggest this is not an isolated phenomenon. In line with our findings, a 2021 case report documented reversible pancreatic insufficiency secondary to chronic giardiasis, emphasizing the need to consider extra-pancreatic etiologies in patients with unexplained EPI [3].
Mechanism of enteroendocrine disruption in chronic giardiasisCCK: cholecystokininImage Credit: Julio Sanchez Gonzalez
Stool microscopy and antigen assays remain first-line testing tools for Giardia, but intermittent cyst excretion limits their sensitivity. Studies indicate that cumulative sensitivity rises only after obtaining multiple separate stool samples [11]. In contrast, molecular methods like multiplex PCR panels, such as the QDx Complete 14-target assay, have demonstrated significantly higher sensitivity and specificity compared to single antigen tests and microscopy [12]. In our patient's case, conventional tests were repeatedly negative; only the PCR panel identified Giardia, enabling prompt treatment. Therefore, clinicians should consider advanced molecular diagnostics when conventional testing fails but clinical suspicion remains, particularly in protracted cases. This case highlights the importance of a broad differential when diarrhea continues despite treatment and supports early evaluation of pancreatic function when malabsorptive symptoms persist.
Metronidazole and tinidazole are considered first-line therapy against Giardia, with tinidazole favored in many protocols due to its single-dose convenience and comparable efficacy [13]. In this case, a single dose of tinidazole led to symptom resolution, aligning with current treatment success benchmarks. For EPI, fecal elastase measurement is a non-invasive diagnostic marker; levels below 200 mcg/g indicate insufficiency, with values under 100 mcg/g signifying severe deficiency. Pancrelipase replacement successfully restores digestive function, improving stool consistency and nutrient absorption. Additionally, bile acid sequestrants such as cholestyramine may be prescribed to manage bile acid diarrhea, a secondary mechanism frequently observed in intestinal mucosal injury, in which unabsorbed bile acids can trigger water and electrolyte secretion, leading to diarrhea [14]. In our patient, the combination of antimicrobial therapy, pancreatic enzyme replacement therapy, and cholestyramine resulted in rapid clinical improvement.
This case demonstrates the importance of a comprehensive approach to persistent diarrhea. Early evaluation of pancreatic function, such as fecal elastase testing, should be considered in patients with prolonged malabsorptive symptoms to promptly identify EPI. When initial stool studies are unrevealing, molecular diagnostics like multiplex PCR panels offer superior sensitivity and can detect overlooked infections, as demonstrated here. Effective treatment may require a multifaceted strategy addressing not only the underlying infection but also enzyme insufficiency and bile acid-induced diarrhea. Nutritional surveillance, particularly for fat-soluble vitamins, is essential to prevent long-term complications. Finally, the detection of EPI should trigger consideration of infectious or inflammatory gastrointestinal causes, not solely pancreatic imaging or endocrinology referrals. Broadening the diagnostic lens in this way can improve outcomes and avoid unnecessary delays in care.
Conclusions
This case highlights an uncommon but clinically significant link between chronic giardiasis and secondary EPI. For clinicians, it reinforces the importance of maintaining a broad differential when evaluating persistent diarrhea, especially when symptoms are refractory to initial treatments. Incorporating early pancreatic function testing and advanced stool diagnostics, such as multiplex PCR panels, can lead to timely diagnosis and targeted therapy. Recognizing these overlapping mechanisms enables a more comprehensive, efficient approach to care that can reduce diagnostic delays, prevent nutritional deficiencies, and improve patient outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Persistent diarrhea: a clinical review JAMA Du Pont HL 2712272331520162735724110.1001/jama.2016.7833 · doi ↗ · pubmed ↗
- 2A scoping review of risk factors and transmission routes associated with human giardiasis outbreaks in high-income settings Curr Res Parasitol Vector Borne Dis Krumrie S Capewell P Smith-Palmer A Mellor D Weir W Alexander CL 100084220223658987710.1016/j.crpvbd.2022.100084 PMC 9795371 · doi ↗ · pubmed ↗
- 3Chronic giardiasis: a rare cause of exocrine pancreatic insufficiency BMJ Case Rep Pophali P Veyseh M Fraij O Hapangama S 014202110.1136/bcr-2021-242129 PMC 810867733962931 · doi ↗ · pubmed ↗
- 4Utility and recommendations for the use of multiplex molecular gastrointestinal pathogen panels J Appl Lab Med Hata DJ Powell EA Starolis MW 11481159820233710250010.1093/jalm/jfad 009 · doi ↗ · pubmed ↗
- 5Prevalence and clinical manifestations of Giardia intestinalis and other intestinal parasites in children and adults in Algeria Am J Trop Med Hyg Belkessa S Ait-Salem E Laatamna A 91091610420213353477110.4269/ajtmh.20-0187 PMC 7941827 · doi ↗ · pubmed ↗
- 6Giardipain-1, a protease secreted by Giardia duodenalis trophozoites, causes junctional, barrier and apoptotic damage in epithelial cell monolayers Int J Parasitol Ortega-Pierres G Argüello-García R Laredo-Cisneros MS 6216394820182957198110.1016/j.ijpara.2018.01.006 · doi ↗ · pubmed ↗
- 7Interactions of Giardia sp. with the intestinal barrier: epithelium, mucus, and microbiota Tissue Barriers Allain T Amat CB Motta JP Manko A Buret AG 05201710.1080/21688370.2016.1274354 PMC 536299828452685 · doi ↗ · pubmed ↗
- 8Identification of enteroendocrine regulators by real-time single-cell differentiation mapping Cell Gehart H van Es JH Hamer K 1158117317620193071286910.1016/j.cell.2018.12.029 · doi ↗ · pubmed ↗