Cardiorespiratory Arrest in the Postoperative Period of Cardiovascular Surgery: What Changes?
Hélio Penna Guimarães, Isadora Salvador Rocco, Walter José Gomes, Solange Guizilini

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
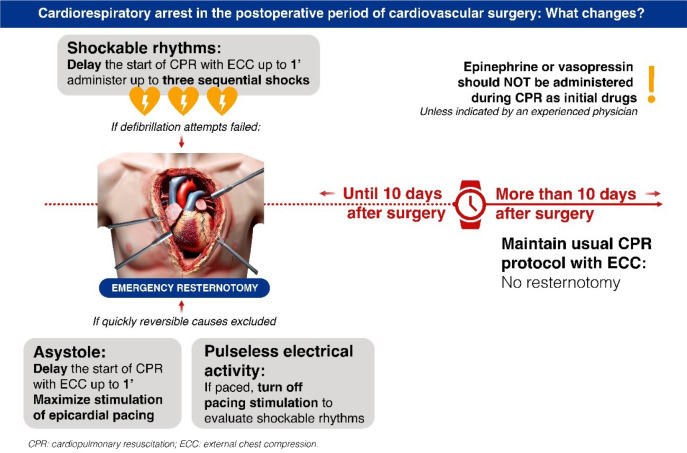 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac, Anesthesia and Surgical Outcomes · Cardiac Arrest and Resuscitation · Airway Management and Intubation Techniques
The occurrence of cardiorespiratory arrest (CRA) in cardiac surgery units is an uncommon but extremely severe event, involving various factors that can directly impact the recovery of spontaneous circulation and the post-CRA prognosis. Therefore, it demands specific approaches and effective protocols for its management.
Most CRAs after cardiac surgery have a reversible cause, such as hypovolemia or cardiac tamponade. In 60 - 70% of these cases, conventional cardiopulmonary resuscitation (CPR) is not effective, necessitating a resternotomy within five minutes of the arrest onset^[1,2]^. It is worth noting that this CRA often occurs in a highly monitored environment, facilitating immediate recognition and rapid and safe intervention by intensivist physicians and cardiovascular surgeons trained to perform advanced life support maneuvers^[1-3]^.
Among the most common causes of CRA after cardiac surgery, hypovolemia is prevalent despite a total body fluid increase of up to 30% after cardiopulmonary bypass (CPB). The depletion of intravascular volume is associated with capillary leakage, hemodilution, redistribution, and polyuria. Hemorrhage may be related to blood dyscrasia or surgical causes, including residual effects of heparin, platelet dysfunction (in number and activity), coagulation factor deficiencies, and extensive fibrinolysis, as well as bleeding from sternal wires and anastomotic or side branches of graft sites.
Low cardiac output may occur due to decreased ventricular function after CPB, myocardial edema, metabolic dysfunction, ischemia, reperfusion injury, and hypocalcemia, returning to baseline values within 24 to 72 hours. Right ventricular failure accounts for approximately 20% of low cardiac output states in the postoperative period. Graft and valve dysfunctions are serious complications, often masked in the immediate postoperative period by temporary epicardial pacing. Although the incidence of early graft dysfunction is low (3%), it can be fatal depending on the presentation, as well as valve dysfunction^[2,3]^. Cardiac tamponade can be challenging to diagnose because the "classic" signs may be challenging to unveil (e.g., in hypovolemic and beta-blocked patients with left ventricular dysfunction)^[3]^.
It is crucial to recognize that postoperative CRA not only challenges the healthcare team in terms of immediate response but also emphasizes the importance of preventive strategies and early interventions during the perioperative period. Essentially, differences between CRA post-cardiac surgery and CRA that typically manifest in other clinical conditions should be considered.
A meta-analysis^[3]^ of 23 studies on CPR not associated with cardiac surgery showed that the incidence of pericardial injury after external chest compression (ECC) is 8.9%, the rate of sternal fracture is 15%, and the rate of rib fracture is 32%. Additionally, cases of myocardial lacerations, cardiac chamber ruptures, prosthetic valve dehiscence, vascular dissection, papillary muscle rupture, and 10% of conduction system injuries have been reported.
In this context, the Society of Thoracic Surgeons (STS)^[4]^, following the methodologies of the American College of Cardiology Foundation/American Heart Association (AHA), proposed recommendations for the management of CRA in the postoperative period of cardiovascular surgery, aiming to optimize care for patients experiencing such an adverse outcome. These recommendations address the need to distinguish between patients with less and more than 10 postoperative days to follow specific protocols, highlighting the importance of individualized care. This differentiation recognizes the potential variations in physiology and clinical conditions of patients at different postoperative stages, which may influence the most appropriate therapeutic strategies.
Thus, some of the recommended modifications to the traditional AHA algorithm should be applied in cases of CRA after cardiac surgery. These modifications include the recommendation for emergency resternotomy as a possible intervention of the resuscitation protocol up to 10 days after surgery; beyond 10 days postoperatively, the traditional protocol should be followed^[5]^.
The evidence supporting the performance of an initial cycle of ECC before defibrillation or the immediate implementation of epicardial pacing is unclear, as potential unnecessary harm should be considered^[6,7]^. The use of drugs in CRA after cardiac surgery does not provide conclusive evidence of benefit or harm. For example, epinephrine may cause severe hypertension and bleeding in patients who recover spontaneous circulation^[7,8]^.
Extracorporeal membrane oxygenation (ECMO) has emerged as a key tool in treating refractory cardiac arrest following cardiac surgery, particularly in younger patients, improving survival and neurological outcomes^[9]^. Its effectiveness relies on the rapid stabilization of hemodynamics and brain perfusion, making prompt initiation critical after identifying cardiac arrest. Despite its potential, ECMO is complex and requires a multidisciplinary team. Hemorrhage is the most common complication, affecting over 50% of cases due to the need for anticoagulation. To maximize ECMO’s benefits while minimizing risks, the development of specific protocols, specialized training, and resource allocation are essential for managing post-cardiac surgery resuscitation^[10-11]^.
In summary, the guidelines recommend specific changes to the usual CPR protocols for post-cardiac surgery cases up to 10 days after surgery^[5-8]^ (Table 1).
Finally, the mortality rate after CRA in postoperative cardiac surgery units can be extremely high, ranging from 50 to 70%, according to data from the United States of America. However, this mortality can be significantly reduced to 35% when specific care protocols, such as the Cardiac Surgery Unit Advanced Life Support recommended by the European Association of Cardio Thoracic Surgery and the STS^[5]^, are routinely implemented and used for training and capacity-building in cardiovascular postoperative units.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Brand J Mc Donald A Dunning J. Management of cardiac arrest following cardiac surgery BJA Educ 2018181162210.1016/j.bjae.2017.11.002.33456790 PMC 7807979 · doi ↗ · pubmed ↗
- 2Society of Thoracic Surgeons Task Force on Resuscitation After Cardiac Surgery The society of thoracic surgeons expert consensus for the resuscitation of patients who arrest after cardiac surgery Ann Thorac Surg 201710331005102010.1016/j.athoracsur.2016.10.033.28122680 · doi ↗ · pubmed ↗
- 3Yadava OP Levine AJ. CSU-ALS protocol for cardiac arrest Indian J Thorac Cardiovasc Surg 202137447147210.1007/s 12055-021-01221-1.34220033 PMC 8218151 · doi ↗ · pubmed ↗
- 4Miller AC Rosati SF Suffredini AF Schrump DS. A systematic review and pooled analysis of CPR-associated cardiovascular and thoracic injuries Resuscitation 201485672473110.1016/j.resuscitation.2014.01.028.24525116 PMC 4031922 · doi ↗ · pubmed ↗
- 5Soar J Berg KM Andersen LW Böttiger BW Cacciola S Callaway CW Adult advanced life support: 2020 international consensus on cardiopulmonary resuscitation and emergency cardiovascular care science with treatment recommendationsresuscitation 2020156 A 80A 11910.1016/j.resuscitation.2020.09.012.33099419 PMC 7576326 · doi ↗ · pubmed ↗
- 6Chan PS Krumholz HM Nichol G Nallamothu BK American Heart Association National Registry of Cardiopulmonary Resuscitation Investigators Delayed time to defibrillation after in-hospital cardiac arrest N Engl J Med 2008358191710.1056/NEJ Moa 0706467.18172170 · doi ↗ · pubmed ↗
- 7Patanwala AE Slack MK Martin JR Basken RL Nolan PE. Effect of epinephrine on survival after cardiac arrest: a systematic review and meta-analysis Minerva Anestesiol 201480783184324193240 · pubmed ↗
- 8Leeuwenburgh BP Versteegh MI Maas JJ Dunning J. Should amiodarone or lidocaine be given to patients who arrest after cardiac surgery and fail to cardiovert from ventricular fibrillation?Interact Cardiovasc Thorac Surg 2008761148115110.1510/icvts.2008.188656.18796471 · doi ↗ · pubmed ↗