Failed Suicide Attempt: From the Forehead to the Mediastinum
N. Jacques, L. Boisliveau

TL;DR
A rare case of a suicide attempt involving the head and mediastinum is presented with a favorable outcome.
Contribution
Highlights the importance of understanding deep cervical anatomy to prevent mediastinitis in such cases.
Findings
The patient had a favorable outcome despite the risk of mediastinitis.
Anatomical knowledge of cervical spaces is crucial to prevent complications.
Abstract
Outside of gunshot wounds, suicidal behavior involving the head is rare. This case presents a patient with a favorable outcome despite a risk of mediastinitis. The anatomy of the deep cervical spaces and the absence of an anatomical barrier to the mediastinum are important to know to prevent this complication.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
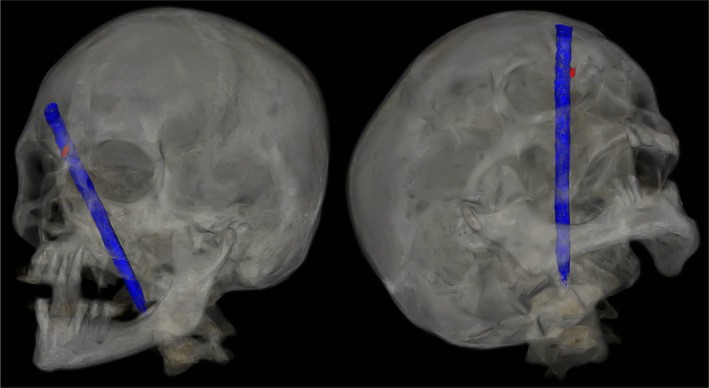 Figure 1
Figure 1 Figure 2
Figure 2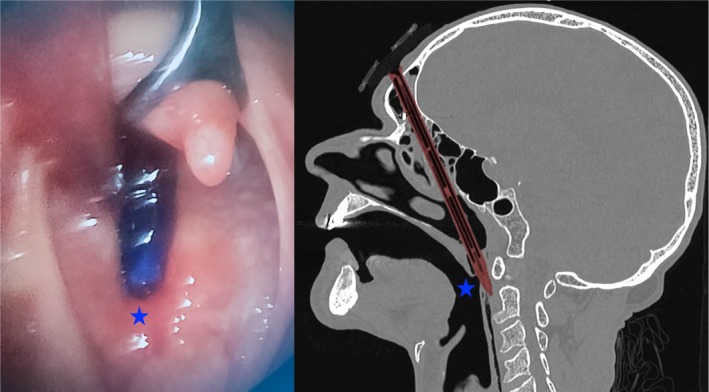 Figure 3
Figure 3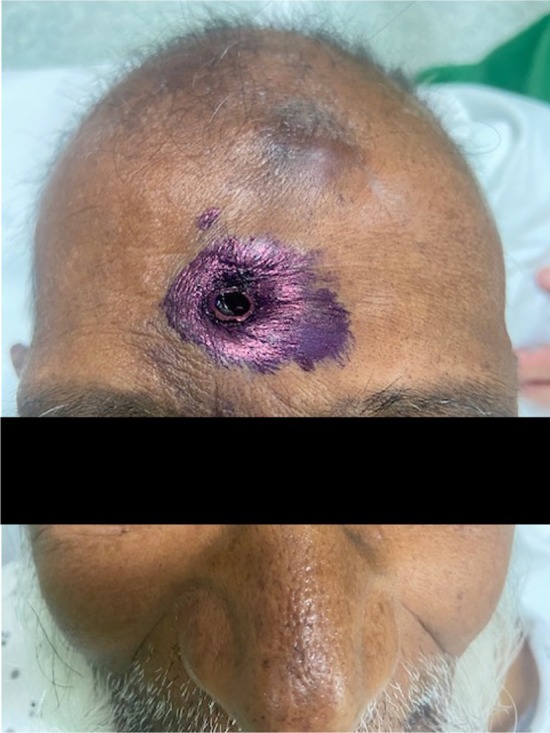 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTraumatic Ocular and Foreign Body Injuries · Facial Nerve Paralysis Treatment and Research · Child Abuse and Related Trauma
An 81‐year‐old man with no prior medical history was hospitalized for recent neurocognitive disorders associated with depressive syndrome, anorexia, and irritability. During his hospitalization, he attempted suicide by directly impacting his forehead against a vertically positioned pencil placed on the table (Figure 1). The CT scan showed the pencil penetrating from the right frontal bone through the frontal sinus (where the pencil lead had come loose) and the ethmoidal cells (Figure 2), then entering the oropharynx and crossing the posterior pharyngeal wall (Figure 3) without vascular or neurological lesions but with the presence of air in the retropharyngeal space and upper mediastinum. The patient was managed by retrograde removal of the pencil under general anesthesia (Figure 4). Post‐operative care consisted of prophylactic Amoxicillin/Clavulanate, placement of a nasogastric tube to protect the pharyngeal suture, and resumption of oral intake on Day 5. There is no anatomical barrier between the mediastinum and the neck [1]. The major risk is the spread of a cervical infection along the deep cervical fascia to the mediastinum. In cases of strong clinical suspicion, mediastinitis secondary to infection of the cervical soft tissues should be ruled out. In our patient's case, the retropharyngeal spaces were involved, leading to the use of Amoxicillin/Clavulanate as prophylactic antibiotic therapy to prevent mediastinitis [2]. The recovery was good, without evidence of mediastinitis. Suicidal behavior involving the head is rare, especially outside of gunshot wounds. Only a few similar cases have been reported in the literature. Moreover, penetrating cranial injuries typically result in death due to the density of critical vascular and neurological structures in this anatomical region. The survival of the patient in this case, along with a favorable outcome, makes this report especially noteworthy. Finally, the sudden onset, the severity of the act, and the recent neurocognitive disorders prompted an extensive search for an organic etiology, such as anti‐NMDA receptor encephalitis, depending on the clinical context [3].
Author Contributions
N. Jacques: conceptualization, writing – original draft, writing – review and editing. L. Boisliveau: resources, validation.
Consent
Written informed consent was obtained from the patient.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1V. F. Chong and Y. F. Fan , “Radiology of the Retropharyngeal Space,” Clinical Radiology 55, no. 10 (2000): 740–748, 10.1053/crad.2000.0510.11052873 · doi ↗ · pubmed ↗
- 2I. Brook , “Microbiology and Management of Peritonsillar, Retropharyngeal, and Parapharyngeal Abscesses,” Journal of Oral and Maxillofacial Surgery 62, no. 12 (2004): 1545–1550.15573356 10.1016/j.joms.2003.12.043 · doi ↗ · pubmed ↗
- 3J. Dalmau , T. Armangué , J. Planagumà , et al., “An Update on Anti‐NMDA Receptor Encephalitis for Neurologists and Psychiatrists: Mechanisms and Models,” Lancet Neurology 18, no. 11 (2019): 1045–1057, 10.1016/S 1474-4422(19)30244-3.31326280 · doi ↗ · pubmed ↗