Ranking factors across multiple domains in predicting adolescent mental health: a Bayesian machine learning approach
Shan Zhao, Xuanjing Li, Xiang Gao, Yipeng Lv, Yang Cao, Gaofeng Mi, Hui Wang, Li Niu, Yan Li

TL;DR
This study uses machine learning to identify and rank factors affecting adolescent mental health in China, highlighting the importance of life experiences and resilience.
Contribution
The novel use of Bayesian machine learning to rank multiple domain factors influencing adolescent mental health in a developing country context.
Findings
Life stress, benevolent events, environmental sensitivity, and coping strategies were common top predictors of mental health outcomes.
Stress mindset and expressive suppression uniquely predicted sleep quality and depressive symptoms, respectively.
Abstract
The prevalence of mental health problems among adolescents is on the rise globally, and is a pressing public health concern in many developing countries, including China. While a growing body of epidemiological research has identified potential factors affecting adolescent mental health, few have considered both risk and protective factors across multiple domains or utilized machine learning approaches to identify and rank these factors. This is a cross-sectional study based on data from 3,526 adolescent participants aged 11–15 years in the Qu County Study in China, and aims to identify and rank factors across five domains—including sociodemographic factors, academic functioning, extracurricular activities, life experiences, and resilience factors—in predicting adolescent mental health outcomes. A Bayesian machine learning approach is used to identify and rank important factors in…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
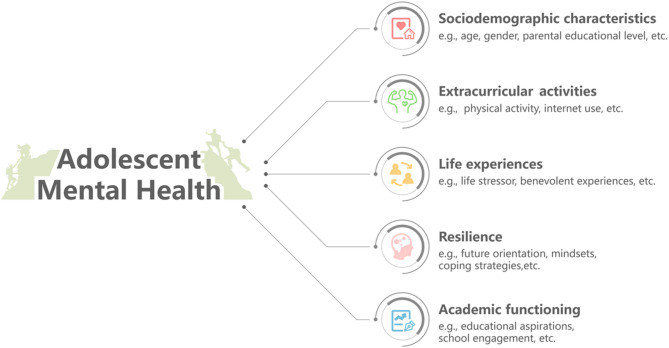 Figure 1
Figure 1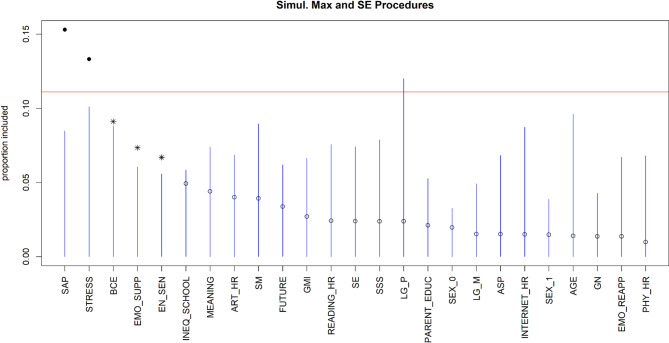 Figure 2
Figure 2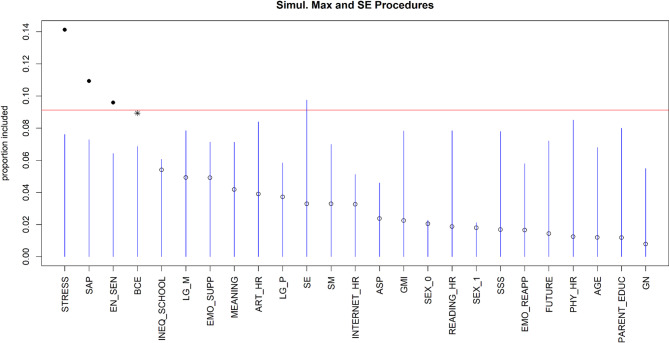 Figure 3
Figure 3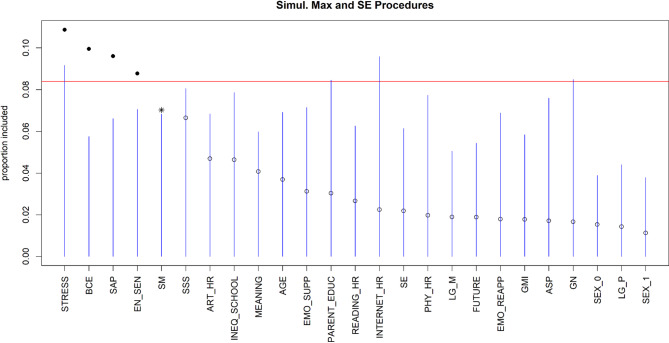 Figure 4
Figure 4- —https://doi.org/10.13039/501100001809National Natural Science Foundation of China
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsChild and Adolescent Psychosocial and Emotional Development · COVID-19 and Mental Health · Sleep and related disorders
Introduction
The World Health Organization (WHO) defines mental health as a state of well-being in which individuals can cope with the normal stressors of life and function productively [1]. Mental health problems are the leading cause of morbidity and mortality among adolescents globally [2]. Without proper interventions, mental health problems during adolescence may have lasting impact on physical health, social life, and longevity in later years [3]. Following the COVID-19 pandemic, several meta-analysis studies found that 1 in 4 children and adolescents under age 18 reported having symptoms of depression or sleep disturbances, and 1 in 5 reported experiencing anxiety symptoms [4, 5]. These high rates of mental health problems almost doubled those reported prior to the pandemic [4, 5]. A recent nationwide survey in China has also demonstrated comparable prevalence rates for mental health problems among Chinese adolescents (i.e., 23.3% for depression and 33.0% for poor sleep quality) [6]. Given the notable rise in the prevalence of adolescent mental health problems [7, 8], there is an urgent need for an improved understanding of risk and protective factors of adolescent mental health to inform effective and actionable prevention strategies. In this context, the present study focuses on depression, anxiety, and poor sleep, which represent three of the most common, burdensome, and interrelated mental health concerns in adolescence [5, 9].
Bronfenbrenner’s ecological systems theory [10] provides a useful framework for understanding how factors across multiple levels—including family environment, individual psychosocial characteristics, and behavioral patterns—influence adolescent development. Guided by this theory, prior research has identified a range of risk and protective factors for adolescent mental health [11–16]. For example, adverse family environments such as low socioeconomic status and exposure to domestic violence (macrosystem and microsystem) have been linked to poorer adolescent mental health [17, 18]. In contrast, benevolent experiences and individual resilience (microsystem and individual factors) function as important protective factors [19–22]. Resilience, in this context, refers to the capacity to adapt effectively to adversity or significant stressors and to recover while maintaining functioning [23]. Based on the existing literature, the present study organizes predictors into five domains—sociodemographic characteristics, academic functioning, extracurricular activities, life experiences, and resilience. These domains align with different ecological layers and have been consistently emphasized in both ecological theory and empirical research as critical to adolescent development and mental health.
Although prior research has improved our understanding of factors associated with adolescent mental health, most studies have relied on traditional regression-based analyses. These approaches assume linearity, normality, and independence, assumptions that often do not hold in real-world data [24]. Moreover, regression models typically explain only a modest proportion of the variance in mental health outcomes and are often underpowered to simultaneously examine a comprehensive set of theory-driven factors across multiple domains. To address these limitations, recent studies have begun to apply machine learning techniques, which can accommodate large, complex datasets and generate insights under more flexible assumptions [25, 26].
Despite these advances, the evidence base remains limited in the following ways. First, much of the research has focused on predictors of single mental health outcomes, overlooking transdiagnostic factors that may influence multiple outcomes simultaneously. This is important because some mental health outcomes, such as sleep disturbances and depressive symptoms, are closely correlated and often predict one another [27, 28]. A deeper understanding of the shared predictors could therefore help identify adolescents at heightened vulnerability. Second, previous research has mostly concentrated on risk factors of adolescent mental health [29], with comparatively little attention to protective factors. For instance, structural risk factors such as family financial strain are consistently linked to adolescent depression [30]; yet these risks can be difficult to modify, particularly in resource-limited contexts. By contrast, protective factors such as coping strategies and resilience may represent more feasible and scalable targets for prevention. Third, although machine learning has been increasingly adopted, approaches with stronger predictive performance and more rigorous methods for quantifying predictor importance are still needed. Bayesian Additive Regression Trees (BART), a Bayesian ensemble method, offers superior predictive performance and a principled framework for evaluating predictor importance [31, 32]. BART has been applied successfully to identify and rank key predictors of chronic conditions such as coronary heart disease, stroke, and cancer [33–35]. Extending this approach to adolescent mental health holds promise for identifying both risk and protective factors across multiple mental health outcomes with greater robustness.
Addressing these gaps, the present study applies the BART approach to identify and rank factors across five domains—including sociodemographic factors, academic functioning, extracurricular activities, life experiences, and resilience factors—in relation to adolescent mental health. We also examine the associations between these predictors and mental health outcomes. We hypothesize that predictors from all five domains will contribute to these outcomes (i.e., depression, anxiety, and sleep quality), with some emerging as transdiagnostic factors and others as outcome-specific. We then apply principled variable selection algorithms informed by the machine learning outputs to evaluate their relative contributions. Collectively, these analyses aim to advance understanding of multilevel risk and protective factors for adolescent mental health.
Methods
Participants
The data for the current study came from the Qu County Study, an ongoing cohort study on the physical and mental health of adolescents in China. We used baseline data collected in October 2023 through paper-and-pencil surveys administered at the two largest public schools in Qu County, Sichuan Province, China. All seventh- and eighth-grade students were invited to participate. A total of 4,983 students were eligible, and 4,897 agreed to participate, yielding a 98.3% participation rate at recruitment. Surveys were administered during regular school hours, with adolescents completing the questionnaires in their respective classrooms under the supervision of trained research assistants. The research assistants explained the study purpose and procedures, obtained informed consent, and addressed any questions from the adolescents.
Of the 4897 adolescents who provided informed consent and completed the questionnaires, 103 were excluded due to missing demographic or outcome data. An additional 1268 were excluded due to missing data on key predictor variables (n = 206 for missing environmental factors, n = 399 for missing academic functioning variables, n = 116 for missing lifestyle information, and n = 547 for missing psychological characteristics). Our final analytical sample included 3,526 adolescents, aged 11 to 15 years, with a mean age of 13.09 years (SD = 0.72), representing all complete cases required for analysis. This sample size is in line with prior applications of BART and is appropriate for stable estimation and mitigating overfitting [36]. Among them, 47.1% were male. Younger participants and female students were more likely to be excluded due to missing data compared to those in the final sample (ps < 0.001). Table 1 presents an overview of the sociodemographic and mental health characteristics of the sample.
Table 1. Sample characteristicsDomainVariableM (SD) / n (%)Min–MaxSociodemographiccharacteristicsSex–Male1659 (47.1%)Female1867 (52.9%)Age13.09 (0.72)11–15Parental highest educational level–Middle school or below1530 (43.4%)High school898 (25.5%)2- or 3-year college319 (9%)4-year college or bachelor’s degree or above779 (22.1%)Subjective SES^a^4.85 (1.27)1–10Extracurricular activitiesPhysical activity (h/week)2.88 (3.82)0–65Reading time (h/week)3.81 (4.99)0–60Internet use (h/week)5.16 (6.72)0–60Art (h/week)1.30 (2.38)0–56Academic functioningMindset of intelligence^b^4.62 (0.99)1–6Educational aspiration–High school or below170 (4.8%)2- or 3-year college115 (3.3%)4-year college or bachelor’s degree1624 (46%)master’s degree or above1617 (45.9%)Learning goalsPerformance-oriented learning goal3.90 (1.15)1–6Mastery-oriented learning goal4.16 (1.10)1–6School engagement3.20 (0.36)1.27-4Life experienceExperience of life stressors2.07 (0.48)1–4Experience of benevolent events7.42 (2.05)0–10ResilienceFuture orientation3.10 (0.57)1–4Meaning in life4.73 (1.39)1–7Gender norm attitude^c^2.81 (0.74)1–5Perceived economic inequality2.39 (0.90)1–5Environmental sensitivity5.08 (0.76)1–7Shift-and-persist strategies2.86 (0.51)1–4Emotion regulation strategiesExpressive suppression4.25 (1.15)1–7Cognitive reappraisal4.51 (0.95)1–7Stress mindset^d^1.88 (0.60)0–4Mental health outcomesDepressive symptoms9.99 (5.70)0–30Anxiety symptoms6.16 (4.92)0–21Poor sleep quality2.25 (0.75)1–4^a^ Individual perceived social status compared with others in their living city^b^ Individual beliefs about whether intelligence is malleable or not^c^ Individual stereotypical attitudes toward masculinities and femininities^d^ Individual beliefs about whether stress is enhancing or debilitating
Measures
Outcome variables
We examined three outcome variables in this study: depressive symptoms, anxiety symptoms, and sleep quality. Depressive symptoms were assessed using the 10-item version of the Center for Epidemiologic Studies Depression Scale (CESD) [37]. The CESD is a well-validated measure with strong reliability and validity demonstrated across diverse populations, including Chinese adolescents [38]. Participants were asked to rate the frequency of each of the 10 symptoms that were provided (e.g., felt depressed). Respondents were given on a 4-point Likert scale from 0 (rarely or none of the time) to 3 (all of the time) and were summed to create a total score ranging from 0 to 30. A higher score therefore indicates more depressive symptoms. A cutoff score of 10 has been suggested in previous research [39]; thus, participants with scores above this threshold were considered to have clinically significant depressive symptoms. In this study, the Cronbach’s coefficient α was 0.84 and the McDonald’s omega reliability coefficient was 0.85.
Anxiety symptoms were measured using the Generalized Anxiety Disorder Scale (GAD-7) [40, 41], a well-validated and widely used instrument for adolescents, which has demonstrated strong psychometric properties in Chinese populations. Participants were asked to evaluate the frequency of each of the seven listed symptoms on a 4-point Likert scale (0 = rarely or none of the time to 3 = all of the time). The scale ranges from 0 to 21, and anxiety symptoms can be indicated as mild, moderate, or severe, as indicated by scores of ≥ 5, ≥10, and ≥ 15, respectively [41]. The scale demonstrated excellent internal consistency, with Cronbach’s α = 0.90 and McDonald’s ω = 0.90.
Sleep quality was assessed using the single subjective sleep quality item from the Pittsburgh Sleep Quality Index, which has been shown to be reliable and valid when compared with polysomnography [42]. Participants were asked to rate their overall sleep quality during the last month, with responses ranging from 1 (excellent) to 4 (poor), with a higher score representing poorer sleep quality. The single-item sleep quality measure is widely used in large-scale studies and has demonstrated acceptable test–retest reliability and construct validity across diverse samples, including Chinese adolescents [43, 44].
Predictors
Consistent with Bronfenbrenner’s ecological systems theory and prior empirical work [10], predictors were organized into five domains that capture key aspects of adolescents’ developmental contexts. Within each domain, the specific variables were selected based on their theoretical relevance and availability in the dataset.
Sociodemographic predictors
Basic sociodemographic information was collected including age, sex (0 = male, 1 = female), parental highest educational level (1 = illiterate or semi-literate, 2 = primary school, 3 = middle school, 4 = high school, 5 = 2- or 3-year college, 6 = 4-year college or bachelor’s degree, 7 = master’s degree or above) and subjective socioeconomic status (SES). Participants’ subjective SES was assessed using the MacArthur Scale of Subjective Social Status [45]. The participants were instructed to evaluate their social status in comparison to others in the city and choose the rung that best matched their social standing. A higher score therefore indicates a higher level of subjective SES.
Extracurricular activity predictors
Participants were asked to estimate the number of hours they spent each week engaging in each of the activities, including physical activities, art, reading, and internet use.
Academic predictors
The mindset of intelligence scale was used to evaluate participants’ beliefs about intelligence [46], either as malleable or fixed. Secondly, participants’ educational aspiration was assessed by asking for the highest level of education that they hope to obtain, a widely used single-item measure in the literature [47]. In addition, six items were used to measure learning goals, including performance-oriented and mastery-oriented goals [48]. Finally, participants’ school engagement was measured by a 15-item scale assessing how they were behaviorally, cognitively, and emotionally engaged in activities at school [49].
Life experience predictors
Participants rated the extent to which they encountered a list of life stressors, including family, peer, and academic stress, which are the most relevant stressors among adolescents based on the literature [50]. Besides, they were also asked to evaluate and quantify positive early life experiences utilizing the 10-item Benevolent Childhood Experience Checklist [51].
Resilience predictors
Participants reported their optimism towards the future and sense of meaning and purpose in life on short scales used in previous research and national surveys [52, 53]. In addition, participants’ gender norm attitude was measured by the subscale of the gender norm instrument, which mainly focused on gender stereotype traits [54]. Moreover, the three-item perceived income inequality scale was used to measure the perceived inequality at school [55]. Participants’ beliefs about stress, either as beneficial or debilitating, were measured using the 8-item Stress Mindset Measure-General (SMM-G) [56]. Additionally, the 12-item Highly Sensitive Child Scale was used to assess participants’ environmental sensitivity [57]. Participants also reported their emotion regulation skills, including two subscales of expressive suppression and cognitive reappraisal [58]. Finally, participants completed the 13-item shift-and-persist questionnaire to assess the frequency with which they adjusted to stressors or adversities (i.e., shift) and confronted adversity with perseverance (i.e., persist) [59]. Detailed psychometric information for all predictors is provided in the supplementary material. Figure 1 presents the conceptual framework of the current study.
Fig. 1. Conceptual framework of the current study
Statistical analysis
Bayesian Additive Regression Trees (BART), a state-of-the-art machine learning technique, was employed to determine and rank important predictors of adolescent mental health outcomes [36]. BART has demonstrated better predictive performance in numerous research areas when compared to other machine learning methods such as random forests and boosted models [31, 34]. BART is a Bayesian “sum-of-trees” model that uses regularization priors to constrain each tree. Specifically, the outcome is modeled as a sum of many regression trees, each of which makes a small contribution to the overall fit. Regularization priors constrain individual trees to remain shallow “weak learners,” which prevents overfitting while allowing the ensemble to flexibly capture complex, nonlinear, and interactive effects [31, 36, 60]. Inference is carried out through a Markov chain Monte Carlo (MCMC) algorithm that samples from the posterior distribution of the ensemble, providing reliable estimates and measures of uncertainty. In our analyses, outcomes are treated as continuous variables in the machine learning analyses. All predictors were used in their original units. For each outcome, we used 1250 posterior draws for each MCMC, eliminating the first 250 as burn-in to ensure a steady process. The default hyperparameters of the bartMachine package (50 trees, k = 2, α = 0.95, β = 2) were applied, consistent with the recommendations of Chipman et al. (2010) and prior research demonstrating their stability [36]. Cross-validation for the number of trees was not conducted, as earlier studies suggest that 50 trees typically provide an effective balance between predictive accuracy and computational efficiency [60].
To evaluate predictor importance, we used the framework developed by Bleich et al. (2014), which computes variable inclusion proportions (VIPs)—the proportion of times a predictor is selected as a splitting rule across posterior samples [31]. To reduce likelihood of spurious associations, null distributions of VIPs are generated through response permutation, providing principled thresholds for which predictors are truly important. Predictors were then ranked by their VIP values, with a higher value indicates higher importance for a specific predictor. Model performance was assessed using two complementary metrics: Pseudo-R², which represents the proportion of variance explained by the model, and Root Mean Squared Error (RMSE), which quantifies the average prediction error; both metrics have been widely used in previous research [34, 61]. Finally, marginal associations between the top predictors and the outcome were illustrated using the partial dependence functions, which show how each predictor relates to the outcome after accounting for all other predictors in the model. These plots estimate the expected outcome across the observed range of a given predictor partially out the contribution of other factors. This approach facilitates interpretation of BART results by illustrating both the direction and shape of predictor–outcome relationships [60]. All the analyses were performed using the bartMachine Package in R 4.3.1.
Results
Of the 3,526 adolescents in the analytical sample, 42% reported clinically significant depressive symptoms, 56.5% reported mild or higher levels of anxiety, and 33.3% reported poor or unsatisfied sleep quality (see Table S2 for details). Moreover, depression and anxiety were positively correlated (r = 0.75, p < 0.001), while poor sleep quality was positively correlated with both anxiety (r = 0.42, p < 0.001) and depression (r = 0.53, p < 0.001).
Figure 2 presents the ranking of different factors that predict depressive symptoms, with the model showing good predictive performance (Pseudo-R² = 0.61, RMSE = 3.54). The top five predictors of depressive symptoms are the implementation of shift-and-persist strategies, experiences of life stressors and benevolent events, the use of expressive suppression strategies, as well as individual environmental sensitivity. The implementation of shift-and-persist strategies appeared to be the most important predictor as shown by the largest VIP value. We also explored marginal relationships between the top predictors and depressive symptoms (see Figure S1 in the supplemental material). The results suggested a generally linear relationship between shift-and-persist strategy, life stressors, benevolent experiences, environmental sensitivity, expressive suppression strategies and depressive symptoms.
Fig. 2. Visualization of the variable selection procedures for depressive symptoms. The standard threshold levels of the variable selection procedure are represented by the blue lines. The red line represents a more rigorous threshold, set at the 95th percentile of null importance values obtained from 10 permutations of the predictors. Solid dots represent variables that cross this threshold. Asterisks indicate variables that pass the blue line but do not reach the red line. An asterisk or a solid dot indicates the variables that have been selected, while unselected variables are indicated by open dots
For anxiety symptoms (Pseudo-R² = 0.46, RMSE = 3.60), the top four predictors are experiences of life stressors, the implementation of shift-and-persist strategies, individual environmental sensitivity and benevolent experiences (see Fig. 3). Life stressor experiences appeared to be the most significant predictor, as indicated by the highest VIP value. The partial dependence plots of marginal effects on each variable with the highest importance on anxiety symptoms are presented in Figure S2, suggesting that individuals who experienced a greater number of life stressors, were more sensitive to environmental factors, had fewer benevolent experiences, and employed shift-and-persist strategies less frequently reported higher levels of anxiety symptoms.
Fig. 3. Visualization of the variable selection procedures for anxiety symptoms. The standard threshold levels of the variable selection procedure are represented by the blue lines. The red line represents a more rigorous threshold, set at the 95th percentile of null importance values obtained from 10 permutations of the predictors. Solid dots represent variables that cross this threshold. Asterisks indicate variables that pass the blue line but do not reach the red line. An asterisk or a solid dot indicates the variables that have been selected, while unselected variables are indicated by open dots
For sleep quality (Fig. 4), the top five predictors are experiences of life stressors, benevolent events, the implementation of of shift-and-persist strategies, individual environmental sensitivity and stress mindset (Pseudo-R² = 0.24, RMSE = 0.65). As indicated by the highest VIP value, life stressor experiences again seem to be the most significant predictor. Further results suggested a linear relationship between shift-and-persist strategy, life stressors, benevolent experiences, environmental sensitivity, stress mindset and sleep quality (see Figure S3).
Fig. 4. Visualization of the variable selection procedures for sleep quality. The standard threshold levels of the variable selection procedure are represented by the blue lines. The red line represents a more rigorous threshold, set at the 95th percentile of null importance values obtained from 10 permutations of the predictors. Solid dots represent variables that cross this threshold. Asterisks indicate variables that pass the blue line but do not reach the red line. An asterisk or a solid dot indicates the variables that have been selected, while unselected variables are indicated by open dots
Discussion
This study applies a Bayesian machine learning approach to identify and rank the protective and risk factors for various mental health outcomes in a sample of Chinese adolescents. Key risk factors included greater exposure to life stressors, higher environmental sensitivity, and greater reliance on expressive suppression strategies, whereas key protective factors included a stress-is-enhancing mindset, higher levels of benevolent experiences, and greater use of shift-and-persist coping strategies. Our findings are consistent with Bronfenbrenner’s ecological systems theory, which emphasizes that adolescent mental health is shaped by dynamic interactions across multiple levels of influence. The results highlight the salience of individual characteristics as well as microsystem factors within the family and school environment. By integrating both individual and contextual influences, our study underscores the importance of considering multi-level determinants when identifying risk and protective factors for adolescent mental health.
Key predictors varied across mental health indicators, but common factors—such as life stressors and benevolent experiences—emerged. These findings align with previous research on the impact of adversity [22, 62], and extend it by emphasizing the importance of benevolent experiences for sleep quality among adolescents. Furthermore, our findings demonstrate that positive experiences show robust associations with mental health, even when controlling for other factors. Future research could examine whether increasing benevolent experiences through school-based programs and parental guidance is associated with lower mental health risks.
Our results also showed that resilience-related characteristics—such as environmental sensitivity and shift-and-persist strategies—are strong common predictors of multiple outcomes. In contrast, expressive suppression and stress mindset are significant contributors to depressive symptoms and sleep quality of adolescents, respectively. These findings are consistent with earlier research highlighting the substantial effects of shift-and-persist strategies, emotion regulation, and environmental sensitivity on depression and anxiety [19, 20, 63]. Our results further suggest that shift-and-persist strategies may be associated with benefits beyond emotional well-being, extending to health-related behaviors such as sleep. Morever, while prior studies have demonstrated that individuals who are sensitive to the environment and those who have a stress-is-debilitating mindset are more likely to report higher depression or anxiety [20, 64]. The current findings added to the body of literature by highlighting the substantial associations of stress mindset and environmental sensitivity with sleep quality. Future research is warranted to explore the longitudinal association between environmental sensitivity, stress mindset and adolescents’ sleep quality. While our study primarily drew on an ecological systems framework to guide variable selection and interpretation, other theoretical perspectives may also provide complementary insights. For instance, emotion dysregulation frameworks may deepen understanding of the mechanisms through which regulation strategies such as expression suppression contribute to psychopathology [65]. Incorporating these perspectives in future work could enrich the interpretation of complex, multidomain predictors identified by the current study.
For adolescents, a sensitive period for mental health risks but also “windows of opportunity” for early intervention [66], these findings collectively highlight the potential value of psychological characteristics, especially those that are malleable, in directing screening practices and guiding future intervention strategies aimed at promoting mental health. Patterns such as heightened environmental sensitivity, limited use of shift-and-persist strategies, or a stress-is-debilitating mindset may serve as indicators of adolescents at greater risk and could benefit from closer monitoring and targeted support. Policy changes to enhance access to high-intensity treatments for mental health are still necessary for adolescents residing in middle- or low-income regions. Nevertheless, implementing these changes could be a protracted process. Future research could examine whether brief psychological interventions that promote resilience delivered through various youth care systems (e.g., primary care, and school programs) would supplement existing support systems and provide benefits for adolescents who currently lack access to additional care. Moreover, given that the outcomes assessed in this study are closely associated with suicidal behavior [67, 68], future research could explore whether the psychological characteristics identified are also pertinent to suicide prevention efforts at the educational, or community levels.
Several limitations should be noted when interpretating these findings. First, the cross-sectional design limits our ability to infer causality or bidirectional associations. As data collection in the Qu County Study continues, longitudinal data will allow us to test the predictive value of these factors for future mental health problems. Second, the sample is drawn from a single region in Southwestern China and is not nationally representative. Nonetheless, most participants came from middle- or lower-class backgrounds, providing valuable insight into the mental health challenges faced by socioeconomically disadvantaged adolescents in China. Future research should examine whether these findings generalize to populations in other cultural contexts and socioeconomic settings. Third, although BART is generally robust to multicollinearity and provides stable predictions, VIP and marginal associations should be interpreted with caution, as highly correlated predictors may conflate shared variance and obscure the unique contribution of individual variables. Finally, this study did not include all relevant variables or potential confounders, such as intelligence quotient, biological markers, or neurocognitive assessments. Incorporating objective measures—such as wearable devices to track daily activity and stress-related biomarkers—could enhance our understanding of predictors of adolescent mental health.
In conclusion, this study identified multidimensional predictors of various mental health outcomes in a large sample of Chinese adolescents. The findings indicate that life stressors, benevolent experiences, environmental sensitivity, shift-and-persist strategies, expressive suppression, and stress mindset were significantly associated with depressive symptoms, anxiety symptoms, and sleep quality among adolescents. Future research, particularly longitudinal and intervention studies, is needed to evaluate whether modifiable life experiences and resilience-related characteristics may help support adolescents’ mental well-being.
Supplementary Information
Below is the link to the electronic supplementary material.
Supplementary Material 1.