Optic Disc Characteristics in Children Born Preterm With and Without ROP: Results From the Gutenberg Prematurity Eye Study Young (GPESY)
Achim Fieß, Sandra Gißler, Stephanie Grabitz, Eva Mildenberger, Timo Uphaus, Marianne Hahn, Norbert Pfeiffer, Alica Hartmann, Alexander K. Schuster

TL;DR
This study examines optic disc features in children born preterm, finding that prematurity and ROP treatment affect retinal nerve fiber layer thickness and other optic nerve characteristics.
Contribution
The study provides new insights into optic nerve head morphology in preterm children with and without ROP, linking perinatal factors to structural changes.
Findings
Extremely preterm children had thinner peripapillary retinal nerve fiber layer (pRNFL) except temporally.
ROP-treated children showed thicker temporal and inferotemporal pRNFL but thinner superonasal sectors.
Prematurity was associated with larger vertical cup-to-disc ratio (vCDR) and smaller minimal rim width (MRW).
Abstract
We investigated optic nerve head morphology in children born preterm with and without retinopathy of prematurity (ROP), focusing on peripapillary retinal nerve fiber layer (pRNFL) thickness, minimal rim width (MRW), Bruch's membrane opening (BMO), and vertical cup-to-disc ratio (vCDR) in relation to perinatal factors (gestational age [GA], birth weight [BW], perinatal adverse events [PAE]). This prospective observational cohort included 793 former preterm children aged four to 17 years, stratified into late preterm (GA 33–36 weeks), moderate preterm (GA 29–32 weeks), extreme preterm (GA ≤28 weeks), preterm with untreated ROP, preterm with ROP treatment, and full-term controls (GA ≥37 weeks). Effects of perinatal factors on pRNFL, MRW, BMO area, and vCDR were evaluated. Extremely preterm children had a thinner pRNFL (β = −9.25, P < 0.001), except temporally. ROP-treated children showed…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure
Figure| Group 1 GA | Group 2 GA 33–36 Wks No ROP | Group 3 GA 29–32 Wks No ROP | Group 4 GA | Group 5 GA | Group 6 GA | |
|---|---|---|---|---|---|---|
| Participants (n)/eyes (n) | 257/502 | 240/474 | 164/318 | 70/136 | 53/99 | 9/17 |
| Sex (female) | 137 (53.3) | 118 (49.2) | 86 (52.4) | 40 (57.1) | 32 (60.4) | 5 (55.6) |
| Age (y), mean (SD) | 11.25 (3.60) | 11.20 (3.75) | 11.72 (3.89) | 11.07 (3.79) | 12.62 (5.11) | 11.78 (3.73) |
| Gestational age (weeks), mean (SD) | 38.98 (1.28) | 34.64 (1.03) | 30.88 (1.06) | 26.21 (1.44) | 26.68 (2.38) | 24.33 (0.87) |
| Birth weight (kg), mean (SD) | 3.37 (0.40) | 2.34 (0.41) | 1.57 (0.35) | 0.84 (0.24) | 0.96 (0.36) | 0.66 (0.23) |
| Birth weight <1500 | 0 (0.0%) | 7 (2.9%) | 72 (43.9%) | 70 (100.0%) | 50 (94.3%) | 9 (100.0%) |
| Birth weight <1000 | 0 (0.0%) | 0 (0.0%) | 9 (5.5%) | 52 (74.3%) | 33 (62.3%) | 8 (88.9%) |
| Birth weight percentile, mean (SD) | 44.71 (24.74) | 34.02 (22.83) | 40.93 (22.28) | 36.47 (25.94) | 43.58 (27.97) | 20.00 (27.44) |
| ROP | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 53 (100.0%) | 9 (100.0%) |
| ROP Stage | ||||||
| 1 | 0 | 0 | 0 | 0 | 27 | 0 |
| 2 | 0 | 0 | 0 | 0 | 14 | 1 |
| 3 | 0 | 0 | 0 | 0 | 12 | 7 |
| 4 | 0 | 0 | 0 | 0 | 0 | 1 |
| ROP plus disease | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 3 (5.7%) | 4 (44.4%) |
| Perinatal adverse events | 0 (0.0%) | 1 (0.4%) | 7 (4.3%) | 26 (37.1%) | 22 (41.5%) | 9 (100.0%) |
| IVH | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 7 (10.0%) | 3 (5.7%) | 1 (11.1%) |
| NEC | 0 (0.0%) | 1 (0.4%) | 4 (2.4%) | 3 (4.3%) | 2 (3.8%) | 2 (22.2%) |
| BPD | 0 (0.0%) | 0 (0.0%) | 3 (1.8%) | 23 (32.9%) | 21 (39.6%) | 9 (100.0%) |
| Pre-eclampsia | 4 (1.6%) | 21 (8.8%) | 29 (17.7%) | 11 (15.7%) | 11 (20.8%) | 1 (11.1%) |
| Placental insufficiency | 0 (0.0%) | 8 (3.3%) | 6 (3.7%) | 5 (7.1%) | 3 (5.7%) | 1 (11.1%) |
| HELLP Syndrome (yes) | 0 (0.0%) | 8 (3.3%) | 18 (11.0%) | 6 (8.6%) | 2 (3.8%) | 0 (0.0%) |
| Gestational diabetes | 32 (12.5%) | 19 (7.9%) | 19 (11.6%) | 3 (4.3%) | 3 (5.7%) | 0 (0.0%) |
| Maternal smoking during pregnancy | 12 (4.7%) | 7 (2.9%) | 7 (4.3%) | 5 (7.1%) | 7 (13.2%) | 2 (22.2%) |
| Breastfeeding | 222 (86.4%) | 181 (75.4%) | 115 (70.1%) | 47 (67.1%) | 24 (45.3%) | 1 (11.1%) |
| Ocular parameters | ||||||
| Visual acuity (LogMAR) | ||||||
| OD, median [IQR] | 0.00 [0.00, 0.10] | 0.00 [0.00, 0.10] | 0.00 [0.00, 0.10] | 0.00 [0.00, 0.10] | 0.00 [0.00, 0.20] | 0.20 [0.20, 0.20] |
| OS, median [IQR] | 0.00 [0.00, 0.10] | 0.10 [0.00, 0.20] | 0.05 [0.00, 0.10] | 0.00 [0.00, 0.10] | 0.00 [0.00, 0.20] | 0.40 [0.10, 0.44] |
| Spherical equivalent (D) | ||||||
| OD, mean (SD) | 0.26 (1.42) | 0.31 (1.47) | 0.40 (1.62) | 0.24 (2.05) | 0.41 (2.10) | −1.54 (2.95) |
| OS, mean (SD) | 0.24 (1.55) | 0.34 (1.55) | 0.47 (1.80) | 0.34 (2.04) | 0.77 (1.56) | −1.33 (3.24) |
| Intraocular pressure (mm Hg) | ||||||
| OD, mean (SD) | 17.00 (3.08) | 16.36 (2.71) | 16.28 (3.11) | 18.02 (3.89) | 17.25 (4.29) | 17.34 (3.68) |
| OS, mean (SD) | 16.38 (2.91) | 15.80 (2.79) | 15.70 (2.99) | 17.13 (3.35) | 16.67 (4.88) | 16.89 (4.38) |
| Group 1 GA | Group 2 GA 33–36 Wks No ROP | Group 3 GA 29–32 Wks No ROP | Group 4 GA | Group 5 GA | Group 6 GA |
| |
|---|---|---|---|---|---|---|---|
| Eyes (n) | |||||||
| OD | 224 | 205 | 142 | 57 | 36 | 5 | |
| OS | 218 | 195 | 133 | 55 | 38 | 5 | |
| pRNFL (µm) (12° circle-scan) | |||||||
| Global, mean (SD) | 102.55 (9.93) | 101.77 (9.90) | 100.42 (10.20) | 93.12 (12.92) | 94.43 (9.30) | 93.51 (13.36) | <0.001 |
| Superotemporal, mean (SD) | 148.26 (20.38) | 149.19 (21.94) | 148.24 (22.62) | 136.92 (22.42) | 138.07 (21.87) | 123.33 (19.39) | <0.001 |
| Temporal, mean (SD) | 73.42 (13.06) | 72.19 (12.01) | 70.15 (12.36) | 66.35 (12.83) | 66.08 (10.97) | 102.94 (33.88) | <0.001 |
| Inferotemporal, mean (SD) | 145.81 (18.05) | 144.52 (19.52) | 145.76 (21.14) | 133.33 (26.75) | 133.80 (19.31) | 151.02 (27.85) | <0.001 |
| Inferonasal, mean (SD) | 114.73 (25.52) | 111.69 (25.16) | 110.31 (25.88) | 102.73 (26.58) | 102.27 (26.15) | 80.47 (30.52) | <0.001 |
| Nasal, mean (SD) | 72.44 (16.10) | 71.16 (15.53) | 68.69 (15.67) | 64.58 (15.35) | 66.69 (18.52) | 54.38 (14.09) | <0.001 |
| Superonasal, mean (SD) | 120.08 (22.72) | 122.05 (24.32) | 121.49 (22.20) | 110.33 (24.25) | 115.48 (25.71) | 78.96 (13.99) | <0.001 |
| BMO area (mm2), mean (SD) | 2.01 (0.43) | 2.03 (0.36) | 2.12 (0.48) | 2.12 (0.38) | 1.94 (0.42) | 1.68 (0.29) | 0.004 |
| MRW (µm) | |||||||
| Global, (SD) | 380.39 (57.55) | 371.88 (49.99) | 384.63 (65.07) | 345.32 (66.38) | 362.30 (71.71) | 424.28 (61.95) | <0.001 |
| Superotemporal, mean (SD) | 361.54 (68.85) | 348.71 (65.26) | 367.64 (71.81) | 325.92 (56.18) | 338.71 (69.20) | 423.37 (50.01) | <0.001 |
| Temporal, mean (SD) | 272.28 (53.86) | 265.26 (47.79) | 273.63 (46.20) | 250.52 (53.88) | 272.01 (72.46) | 362.27 (64.90) | <0.001 |
| Inferotemporal, mean (SD) | 416.65 (66.35) | 404.51 (56.44) | 420.52 (62.96) | 369.12 (67.04) | 394.74 (62.74) | 469.70 (53.29) | <0.001 |
| Inferonasal, mean (SD) | 469.02 (66.13) | 460.37 (64.89) | 472.35 (77.89) | 421.79 (89.23) | 440.10 (84.97) | 491.82 (50.13) | <0.001 |
| Nasal, mean (SD) | 411.37 (67.42) | 406.22 (60.67) | 414.61 (88.56) | 376.16 (87.02) | 387.33 (89.09) | 421.10 (83.26) | 0.001 |
| Superonasal, mean (SD) | 432.36 (78.50) | 419.37 (72.41) | 445.34 (90.89) | 392.92 (78.65) | 410.00 (85.01) | 460.71 (67.89) | <0.001 |
| Optic disc characteristics | |||||||
| Eyes OD (n) | 240 | 226 | 159 | 69 | 48 | 9 | |
| Vertical disc length (mm) | 1.73 (0.18) | 1.74 (0.17) | 1.75 (0.18) | 1.76 (0.20) | 1.71 (0.19) | 1.78 (0.19) | 0.680 |
| Vertical cup length (mm) | 0.48 (0.26) | 0.50 (0.28) | 0.53 (0.29) | 0.62 (0.32) | 0.56 (0.30) | 0.47 (0.27) | 0.008 |
| VCDR [IQR] | 0.26 [0.15, 0.38] | 0.26 [0.16, 0.38] | 0.28 [0.19, 0.42] | 0.34 [0.24, 0.47] | 0.34 [0.20, 0.42] | 0.27 [0.21, 0.39] | 0.013 |
| Longer disc diameter (mm) | 1.73 (0.18) | 1.73 (0.17) | 1.74 (0.18) | 1.75 (0.20) | 1.70 (0.19) | 1.80 (0.28) | 0.608 |
| Shorter disc diameter (mm) | 1.54 (0.16) | 1.56 (0.16) | 1.55 (0.16) | 1.57 (0.19) | 1.52 (0.19) | 1.55 (0.20) | 0.619 |
| Optic disc area (mm2) | 2.12 (0.43) | 2.14 (0.41) | 2.14 (0.42) | 2.18 (0.50) | 2.04 (0.47) | 2.23 (0.63) | 0.668 |
| Torsion angle (absolute)°, [IQR] | 17.00 [10.25, 27.50] | 17.00 [9.50, 28.00] | 15.00 [7.00, 22.00] | 12.50 [9.00, 18.50] | 14.00 [8.00, 24.50] | 11.00 [2.00, 14.00] | 0.012 |
| Tilted | 10 (4.8%) | 11 (5.2%) | 8 (5.7%) | 3 (4.8%) | 2 (4.8%) | 0 (0.0%) | 0.989 |
| Torted | 121 (57.6%) | 116 (54.0%) | 70 (48.3%) | 24 (36.4%) | 18 (41.9%) | 2 (22.2%) | 0.011 |
| Eyes OS | 221 | 211 | 140 | 57 | 46 | 7 | |
| Vertical disc length (mm) | 1.73 (0.17) | 1.73 (0.18) | 1.74 (0.18) | 1.72 (0.15) | 1.71 (0.18) | 1.87 (0.37) | 0.340 |
| Vertical cup length (mm) | 0.47 (0.26) | 0.49 (0.28) | 0.53 (0.27) | 0.58 (0.29) | 0.57 (0.28) | 0.58 (0.50) | 0.041 |
| VCDR [IQR] | 0.26 [0.16, 0.37] | 0.26 [0.16, 0.38] | 0.30 [0.20, 0.40] | 0.33 [0.24, 0.41] | 0.34 [0.18, 0.43] | 0.27 [0.12, 0.42] | 0.018 |
| Longer disc diameter (mm) | 1.74 (0.16) | 1.74 (0.18) | 1.76 (0.19) | 1.72 (0.17) | 1.72 (0.18) | 1.81 (0.37) | 0.604 |
| Shorter disc diameter (mm) | 1.55 (0.15) | 1.56 (0.16) | 1.56 (0.16) | 1.56 (0.17) | 1.54 (0.18) | 1.60 (0.29) | 0.931 |
| Optic disc area (mm2) | 2.14 (0.40) | 2.14 (0.43) | 2.18 (0.45) | 2.13 (0.42) | 2.10 (0.45) | 2.34 (0.96) | 0.759 |
| Torsion angle (absolute), [IQR] | 21.00 [13.50, 31.00] | 21.00 [13.00, 30.00] | 19.00 [12.00, 25.00] | 20.00 [14.00, 29.50] | 20.00 [12.00, 30.00] | 16.00 [12.25, 28.00] | 0.663 |
| Tilted | 7 (3.6%) | 7 (3.7%) | 6 (5.0%) | 1 (2.0%) | 1 (2.6%) | 0 (0.0%) | 0.929 |
| Torted | 118 (67.4%) | 116 (67.1%) | 71 (65.1%) | 27 (69.2%) | 20 (60.6%) | 4 (66.7%) | 0.975 |
| Global | Superotemporal | Temporal | Inferotemporal | Inferonasal | Nasal | Superonasal | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Factor |
|
|
|
|
|
|
| |||||||
| Age (y) | 0.13 [−0.15; 0.41] | 0.35 | 0.23 [−0.21; 0.77] | 0.40 | −0.38 [−0.69; −0.07] | 0.02 | 0.11 [−0.40; 0.62] | 0.67 | 0.11 [−0.56; 0.78] | 0.75 | 0.25 [−0.14; 0.64] | 0.21 | 0.64 [0.08; 1.20] | 0.03 |
| Sex (Female) | −0.16 [−1.92; 1.61] | 0.86 | 0.20 [−3.29; 3.70] | 0.91 | 1.31 [−0.71; 3.33] | 0.20 | 1.36 [−1.85; 4.57] | 0.41 | −3.13 [−7.03; 0.76] | 0.11 | −0.02 [−2.43; 2.39] | 0.99 | −1.95 [−5.61; 1.71] | 0.30 |
| Axial Length | 0.13 [−0.89; 1.15] | 0.80 | 2.09 [0.28; 3.91] | 0.02 | 1.63 [0.35; 2.92] | 0.01 | 0.28 [−1.67; 2.22] | 0.78 | −3.88 [6.07; −1.69] | <0.001 | 0.34 [−1.00; 1.68] | 0.62 | −0.16 [−2.24; 1.93] | 0.88 |
| Gestational age | ||||||||||||||
| ≤28wk | −9.25 [−12.07; −6.44] | <0.001 | −11.12 [−16.23; −6.00] | <0.001 | −2.65 [−6.23; 0.94] | 0.15 | −11.12 [−16.63; −5.61] | <0.001 | −16.88 [−23.26; −10.50] | <0.001 | −8.85 [−12.67; −5.04] | <0.001 | −11.48 [−16.99; −5.97] | <0.001 |
| 29–32 wk | −1.64 [−3.90; 0.61] | 0.15 | 2.22 [−2.13; 6.57] | 0.32 | −2.83 [−5.29; −0.38] | 0.02 | 1.97 [2.13; 6.06] | 0.35 | −4.60 [−10.02; 0.82] | 0.10 | −3.49 [−6.62; −0.35] | 0.03 | 0.51 [−4.02; 5.05] | 0.82 |
| 33–36 wk | −0.37 [−2.38; 1.65] | 0.72 | 1.09 [−2.92; 5.09] | 0.59 | −2.18 [−4.45; 0.08] | 0.06 | −1.39 [−4.88; 2.10] | 0.44 | −0.86 [−5.77; 4.05] | 0.73 | 0.25 [−2.64; 3.14] | 0.87 | 2.22 [−2.17; 6.60] | 0.32 |
| ≥37 wk | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. |
| Birth weight percentile | ||||||||||||||
| <25 | −3.77 [−5.59; −1.95] | <0.001 | −4.77 [−8.38; −1.16] | 0.01 | −0.57 [−2.73; 1.59] | 0.60 | −3.44 [−6.84; −0.04] | 0.05 | −6.29 [−10.45; −2.14] | 0.003 | −3.43 [−5.91; −0.94] | 0.007 | −7.59 [−11.38; −3.79] | <0.001 |
| 25–75 | Ref. | Ref. | Ref. | Ref. | ||||||||||
| >75 | 0.33 [−2.41; 3.07] | 0.81 | −3.25 [−8.42; 1.92] | 0.22 | −1.03 [−4.27; 2.22] | 0.54 | 1.51 [−3.11; 6.12] | 0.52 | 4.43 [−2.94; 11.80] | 0.24 | 2.84 [−1.17; 6.85] | 0.17 | −3.33 [−8.42; 1.75] | 0.20 |
| ROP | ||||||||||||||
| ROP treatment (yes) | 5.90 [−3.45; 15.24] | 0.22 | −6.83 [−21.16; 7.51] | 0.35 | 43.31 [20.12; 66.50] | <0.001 | 20.97 [1.14; 40.81] | 0.04 | −22.90 [−47.63; 1.83] | 0.07 | −3.71 [−14.30; 6.87] | 0.49 | −26.22 [−34.37; −18.06] | <0.001 |
| ROP (yes) | −0.27 [−3.73; 3.19] | 0.88 | −2.45 [−9.78; 4.88] | 0.51 | −0.23 [−3.81; 3.34] | 0.90 | −2.83 [−9.81; 4.14] | 0.43 | −4.44 [−12.55; 3.66] | 0.28 | 1.91 [−3.73; 7.55] | 0.51 | 2.71 [−5.52; 10.95] | 0.52 |
| No ROP | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. |
| Perinatal adverse events (yes) | −7.68 [−11.74; −3.63] | <0.001 | −5.97 [−13.41; 1.47] | 0.12 | 1.10 [−4.99; 7.19] | 0.72 | −4.55 [−12.59; 3.48] | 0.27 | −22.01 [−29.91; −14.11] | <0.001 | −8.61 [−13.21; −4.02] | <0.001 | −13.66 [−21.96; −5.35] | 0.001 |
| Preeclampsia (Yes) | −0.78 [−3.92; 2.35] | 0.62 | −4.20 [−9.55; 1.16] | 0.12 | −0.75 [−4.55; 3.05] | 0.70 | −3.79 [−9.94; 2.36] | 0.23 | 1.61 [−5.66; 8.89] | 0.66 | 2.77 [−1.77; 7.31] | 0.23 | −4.76 [−9.86; 0.34] | 0.07 |
| Placental insufficiency (Yes) | −3.95 [−9.15; 1.26] | 0.14 | −5.72 [−14.03; 2.59] | 0.18 | −3.67 [−9.60; 2.26] | 0.22 | −5.47 [−15.67; 4.73] | 0.29 | −5.43 [−16.69; 5.83] | 0.34 | 0.01 [−5.98; 5.99] | 1.00 | −7.47 [−15.32; 0.37] | 0.06 |
| Smoking during pregnancy (Yes) | −4.00 [−8.11; 0.11] | 0.06 | 1.59 [−6.34; 9.51] | 0.69 | −2.72 [−7.90; 2.46] | 0.30 | −4.48 [−12.73; 3.77] | 0.29 | −12.02 [−19.97; −4.08] | 0.003 | −4.54 [−8.82; −0.26] | 0.04 | −2.33 [−9.50; 4.84] | 0.52 |
| Breastfeeding (Yes) | 2.25 [0.44; 4.06] | 0.02 | 3.56 [−0.10; 7.21] | 0.06 | 0.36 [−1.90; 2.61] | 0.76 | 1.45 [−1.96; 4.85] | 0.41 | 6.27 [2.25; 10.29] | <0.002 | 0.65 [−1.88; 3.18] | 0.61 | 4.84 [1.09; 8.60] | 0.01 |
| Factor | Global | Superotemporal | Temporal | Inferotemporal | Inferonasal | Nasal | Superonasal | BMO (mm2) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
|
|
|
|
|
|
|
| |||||||||
| Age, y | −1.47 [−3.58; 0.64] | 0.17 | −2.08 [−4.47; 0.31] | 0.09 | −2.24 [−4.11; −0.36] | 0.02 | −0.85 [−3.13; 1.44] | 0.47 | −1.92 [−4.39; 0.56] | 0.13 | −1.27 [−3.95; 1.40] | 0.35 | −0.54 [−3.56; 2.49] | 0.73 | −0.003 [−0.02; 0.013] | 0.69 |
| Sex (Female) | −5.41 [−18.02 7.20] | 0.4 | 4.04 [−9.76; 17.83] | 0.57 | −9.30 [−20.43; 1.83] | 0.10 | −1.10 [−14.75; 12.56] | 0.87 | −4.57 [−19.74; 10.60] | 0.56 | −5.90 [−21.58; 9.78] | 0.46 | −7.19 [−24.08; 9.70] | 0.40 | −0.05 [−0.14; 0.04] | 0.24 |
| Axial Length | −2.49 [−4.69; −0.28] | 0.03 | −1.44 [−2.34; −0.53] | 0.002 | 0.80 [0.25; 1.39] | 0.007 | −5.45 [−9.28; −1.62] | 0.005 | −5.23 [−9.14; −1.33] | 0.009 | −0.83 [−3.62; 1.95] | 0.56 | −4.60 [−9.94; 0.75] | 0.09 | −0.01 [−0.05; 0.03] | 0.66 |
| Gestational age | ||||||||||||||||
| ≤28 weeks | −15.88 [−36.15; 4.38] | 0.125 | −16.14 [−35.76; 3.47] | 0.11 | 0.66 [−17.81; 19.13] | 0.94 | −30.36 [−51.32; −9.39] | 0.005 | −28.85 [−53.93; −3.78] | 0.02 | −16.13 [−41.50; 9.23] | 0.21 | −20.85 [−45.99; 4.29] | 0.10 | −0.01 [−0.13; 0.12] | 0.93 |
| 29–32 weeks | −0.95 [−18.79; 16.88] | 0.92 | 2.35 [−17.57; 22.27] | 0.82 | 1.27 [−12.82; 15.36] | 0.86 | −0.86 [−19.99; 18.27] | 0.93 | −0.40 [−21.60; 20.80] | 0.97 | −4.47 [−27.46; 18.52] | 0.70 | 1.74 [−22.57; 26.05] | 0.89 | 0.13 [0.01; 0.25] | 0.04 |
| 33–36 weeks | −6.17 [−19.73; 7.38] | 0.37 | −12.04 [−29.02; 4.94] | 0.16 | −5.60 [−18.43; 7.23] | 0.39 | −8.73 [−24.46; 7.01] | 0.28 | −0.77 [−17.41; 15.87] | 0.93 | −3.90 [−19.99; 12.19] | 0.63 | −10.36 [29.76; 9.04] | 0. 30 | 0.02 [−0.08; 0.11] | 0.73 |
| ≥37 weeks | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. |
| Birth weight percentile | ||||||||||||||||
| <25 | −5.51 [−18.82; 7.81] | 0.42 | −2.20 [−17.41; 13.00] | 0.78 | 0.81 [−10.82; 12.43] | 0.89 | −1.55 [−15.91; 12.82] | 0.83 | −11.55 [−27.31; 4.22] | 0.15 | −10.23 [−26.77; 6.32] | 0.23 | −6.73 [−24.74; 11.27] | 0.46 | 0.02 [−0.07; 0.11] | 0.68 |
| 25–75 | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. | ||||||||||
| >75 | −5.17 [−27.79; 17.44] | 0.65 | −12.85 [−35.89; 10.19] | 0.27 | −9.48 [−29.54; 10.59] | 0.35 | 7.00 [−20.14; 34.14] | 0.61 | 11.00 [−17.85; 39.86] | 0.45 | −9.32 [−37.94; 19.30] | 0.52 | −5.59 [−33.09; 21.91] | 0.69 | −0.004 [−0.16; 0.15] | 0.95 |
| ROP | ||||||||||||||||
| ROP treatment | 61.92 [−0.42; 124.25] | 0.05 | 74.40 [25.30; 123.50] | 0.003 | 97.44 [34.11; 160.77] | 0.003 | 75.99 [20.78; 131.2] | 0.007 | 50.44 [−0.93; 101.81] | 0.05 | 34.04 [−53.39; 121.47] | 0.45 | 48.62 [−23.43; 120.66] | 0.19 | −0.34 [−0.72; 0.03] | 0.07 |
| ROP | 0.57 [−9.30; 10.43] | 0.91 | 0.04 [−3.50; 3.58] | 0.98 | −0.32 [−1.61; 0.97] | 0.63 | 3.09 [−12.24; 18.42] | 0.69 | 1.49 [−17.16; 20.15] | 0.88 | −1.19 [−14.23; 11.86] | 0.86 | −1.61 [−22.46; 19.23] | 0.88 | 0.12 [−0.30; 0.55] | 0.57 |
| No ROP | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. |
| Perinatal adverse events | −24.18 [−52.91; 4.55] | 0.10 | −24.34 [−52.55; 3.88] | 0.09 | −18.63 [−44.82; 7.56] | 0.16 | −9.33 [−36.74; 18.09] | 0.51 | −21.08 [−55.85; 13.68] | 0.23 | −32.37 [−67.85; 3.11] | 0.07 | −28.65 [−64.34; 7.05] | 0.12 | −0.15 [−0.32; 0.02] | 0.08 |
| Preeclampsia | −4.76 [−26.71; 17.20] | 0.67 | −10.51 [−33.19; 12.17] | 0.36 | 4.24 [−16.10; 24.57] | 0.68 | −3.51 [−25.51; 18.49] | 0.75 | −9.62 [−35.64; 16.40] | 0.47 | −4.79 [−33.50; 23.91] | 0.74 | −16.04 [−42.37; 10.29] | 0.23 | −0.09 [−0.22; 0.05] | 0.22 |
| Placental insufficiency | −1.47 [−35.64; 32.71] | 0.93 | 0.49 [−34.68; 35.67] | 0.98 | −1.91 [−36.62; 32.80] | 0.91 | −0.553 [−30.45; 29.34] | 0.97 | 3.77 [−36.92; 44.45] | 0.86 | −6.59 [−47.90; 34.72] | 0.75 | 8.09 [−29.33; 45.52] | 0.67 | −0.18 [−0.40; 0.04] | 0.1 |
| Smoking during pregnancy | 2.97 [−22.64; 28.59] | 0.82 | 13.41 [−14.72; 41.55] | 0.35 | 21.82 [−4.75; 48.39] | 0.11 | 17.19 [−15.16; 49.55] | 0.30 | −7.29 [−39.09; 24.50] | 0.65 | −17.38 [−46.04; 11.29] | 0.23 | 3.94 [−30.12; 37.99] | 0.82 | 0.07 [−0.16; 0.29] | 0.56 |
| Breastfeeding | −5.85 [−19.84; 8.15] | 0.41 | −16.04 [−31.45; −0.63] | 0.04 | −8.73 [−21.46; 4.00] | 0.18 | −0.25 [−15.66; 15.16] | 0.97 | 1.72 [−15.45; 18.89] | 0.84 | −4.08 [−21.30; 13.15] | 0.64 | −7.29 [−26.20; 11.63] | 0.45 | 0.07 [−0.02; 0.16] | 0.12 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsRetinopathy of Prematurity Studies · Neonatal and fetal brain pathology · Preterm Birth and Chorioamnionitis
Preterm birth, defined as delivery before 37 weeks of gestation,1 affects neurodevelopment and is associated with changes in optic nerve head morphology.2 Several studies have assessed the optic nerve head characteristics in children and adults born preterm and mainly analyzed the thickness of the (peripapillary) retinal nerve fiber layer (pRNFL),3^–^5 cup-to-disc ratio (CDR),6^–^9 and optic disc size.10^,^11 The assessment of other optic disc characteristics such as minimal rim width (MRW)12 and opening of the Bruch's-membrane (BMO) remain scarce, although these provide additional information on the status of the optic nerve head. This is important because changes in the anatomy of the optic nerve head, especially found in preterm children, may raise suspicion of glaucoma, which may lead to lifelong antiglaucomatous medication.13 To date, one study by Lee et al.14 has assessed BMO and MRW in 120 school-aged children born preterm and full-term, including 42 children born full-term, 41 children born preterm without retinopathy of prematurity (ROP), 16 children with ROP treated with intravitreal bevacizumab, and 21 children with ROP treated with laser. They found that laser-treated children had a greater MRW and thicker temporal pRNFL than children born full-term or preterm without ROP treatment.14 Wenner et al.13 focused on pRNFL, CDR, and rim width measures in 55 children born preterm (gestational age [GA] ≤ 36 weeks, mean age 10 ± 2.5 years) with and without brain injury. Both studies involved small sample sizes and participants with ROP, but treatment assessment was only included by Lee et al.14
The aim of the Gutenberg Prematurity Eye Study Young (GPESY) was to assess the optic nerve head morphology of a large cohort of children aged four to 17 years with and without ROP including a comprehensive analysis of pRNFL-thickness, MRW, size of BMO area, and several morphological features of the optic disc such as the vertical CDR (vCDR) in relation to perinatal information such as GA, birth weight percentile, perinatal adverse events, maternal smoking during pregnancy and breastfeeding.
Material and Methods
Study Population
The GPESY was conducted at the University Medical Center of the Johannes Gutenberg University Mainz (UMCM) in Germany and involved children and adolescents aged four to 17 years born preterm or at term (between 2003 and 2018). It is a retrospective cohort study with a prospective ophthalmologic examination and an extension to the Gutenberg Prematurity Study (GPS) in adults.4^,^6^,^15^–^22 The perinatal history was assessed retrospectively by reviewing the medical record data stored in the UMCM, whereas the prospective part consisted of an extensive ophthalmologic examination. Potential participants were selected by an algorithm inviting every individual born at a GA at birth ≤32 weeks and every third individual born at a GA of 33 to 36 weeks. Additionally, eight individuals born full-term (four male individuals and four female individuals from the beginning of each month of the calendar) with a birthweight between the tenth and ninetieth percentile were recruited as controls (see Supplementary Figure S1). Written informed consent was obtained from all participants and their legal guardians before their study entry. The participants were examined, and their medical history was recorded between 2022 and 2023. The GPESY complies with Good Clinical Practice (GCP), Good Epidemiological Practice (GEP), and the ethical principles of the Declaration of Helsinki. The study protocol and documents were approved by the local ethics committee of the Medical Chamber of Rhineland-Palatinate, Germany (reference no. 2021-15830; original vote: May 5, 2021, latest update: January 19, 2022).
Assessment of Prenatal, Perinatal, and Postnatal Medical History
Medical records at the UMCM were reviewed for the following data: GA (weeks), birth weight (kg), presence of ROP, stage of ROP, ROP treatment, placental insufficiency, preeclampsia, breastfeeding, maternal smoking during pregnancy, and perinatal adverse events. Birth weight percentiles were calculated according to Voigt et al,23 based on data from a newborn cohort in the Federal Republic of Germany.
Categorization
Participants were categorized into six groups, consisting of term-born children with a GA at birth ≥37 completed weeks (group 1), participants born preterm with a GA of 33 to 36 weeks without ROP (group 2), participants born preterm with a GA of 29 to 32 weeks without ROP (group 3), participants born preterm with a GA ≤28 weeks without ROP (group 4), participants born preterm with a GA ≤32 and nontreated ROP (group 5), and those with treated ROP (group 6). In the case in which only one eye was affected with ROP, the other non-ROP eye was excluded from the analysis.
Ophthalmologic Examination
The detailed ophthalmologic examination included testing of distant corrected visual acuity (DCVA) with an ARK 1s (NIDEK; Oculus, Wetzlar, Germany) and the measurement of axial length with a LenStar (Lenstar LS900; Haag-Streit, Bern, Switzerland). Additionally, the intraocular pressure was measured with a non-contact tonometer (NT 2000; Nidek Co., Tokyo, Japan). The visual acuity was converted from decimal to logMAR.24
Optical Coherence Tomography
Spectral-domain optical coherence tomography (SD-OCT) of the peripapillary region was conducted using a peripapillary scan of 12° diameter centered on the optic disc with eye-tracking and standard 7.7 mm corneal curvature and ametropia of 0 diopters (D). We performed automated layer segmentation using the Heidelberg Eye Explorer Software tool (HEYEX, version 6.13.3.0). Global and sectorial pRNFL thickness (global, superonasal, nasal, inferonasal, inferotemporal, temporal, superotemporal) were automatically calculated by the software algorithm. Ocular magnification adjustments were made by taking into account the corneal curvature and spherical equivalent.25^,^26 Furthermore, 24 high-resolution optic nerve head radial scans and three circle scans were obtained using the Glaucoma Module Premier Edition software (version 6.10; Heidelberg Engineering Inc., Heidelberg, Germany). The BMO-MRW was defined as the shortest distance from the BMO to the internal limiting membrane and was automatically calculated with the HEYEX software (see Supplementary Fig. S3).27 The image quality of OCT scans was evaluated regarding centration and focus as well as accurate segmentation. Scans that did not meet these criteria were classified as invalid. Peripapillary RNFL layers were segmented manually in the case of missegmentation by the software, with the images excluded if segmentations could not be corrected or the quality was poor (<15 db).
Fundus Photography and Optic Disc Measurements
Fundus photography (Visucam PRO NM; Zeiss, Oberkochen, Germany) was performed in a darkened room with mydriatic pupils, including 30° and 45° images of the optic nerve head. The right eye was imaged first, and regular data quality control was conducted. The discrepancy between the number of participants reported in the characteristics section and those included in the tables of fundus image measurements reflects the number of images that were unsuitable for further evaluation (Tables 1, 2).
We captured optic disc photographs and manual measurements were conducted by an experienced masked investigator under supervision by an experienced ophthalmologist (ImageJ software, version 1.53a) as described previously.6 The following optic disc parameters were measured: vertical disc length (mm), vertical cup length (mm), VCDR, longer disc diameter (mm), shorter disc diameter (mm), optic disc area (mm^2^), torsion angle (absolute, in degrees), tilted disc, and torted disc. All measured lengths were corrected for ocular magnification, according to Garway-Heath et al.25
Covariates
The covariates were defined as factors that may affect the main outcome measures, that is age (years), sex (female), spherical equivalent (diopters), axial length (mm), optic disc size (mm^2^), GA (weeks), birth weight (kg), birthweight percentile, ROP, ROP treatment, maternal smoking, placental insufficiency, preeclampsia, breastfeeding, and perinatal adverse events such as an intraventricular hemorrhage (at least grade 3 or parenchymal hemorrhage), necrotizing enterocolitis, and moderate or severe bronchopulmonary dysplasia (defined according to the definition of the German query for quality control of the neonatal clinics28).
Statistical Analysis
The main outcome measures were the global pRNFL-thickness, the global MRW, the BMO area, and VCDR. Descriptive statistics were stratified according to the groups. Absolute and relative frequencies were calculated for dichotomous parameters, with the mean and standard deviation calculated for approximately normally distributed variables (otherwise median and interquartile range). One-way ANOVA was used to compare continuous and approximately normally distributed variables and the chi-squared test for dichotomous variables. The Kruskal-Wallis-Test was used to compare continuous variables of non-normal distribution. Linear regression with generalized estimating equations was conducted for pRNFL-thickness, global MRW, and BMO area analysis in a complete case analysis set to account for inter-eye correlations within each participant.
Because of the skewness in the VCDR distribution, the associations were analysed using a linear quantile mixed model with the eyes set as a random factor to account for the inter-eye correlation and the median (τ = 0.5) was used to calculate the estimator. Univariable analysis was performed regarding the influence of GA [groups: GA ≤ 28 weeks, GA 29–32 weeks, GA 33–36 weeks, GA ≥ 37 weeks (Reference)] , birth weight percentile [groups: <25, 25–75 (Reference), >75], ROP [groups: treated ROP, ROP, no ROP (Reference)], perinatal adverse events, preeclampsia, placental insufficiency, maternal smoking during pregnancy, and breastfeeding. The multivariable model (model 1) additionally adjusted the analyses for age (years), sex (female), axial length (mm), and optic disc area (mm^2^) for the VCDR analysis. An additional multivariable sensitivity analysis was performed after exclusion of participants with periventricular leukomalacia (PVL) (excluded were n = 2 in the group with GA 29–32 weeks, n = 6 in the group with GA ≤ 28 weeks without ROP, n = 5 in preterms with ROP without treatment, and n = 2 in preterm children with treated ROP).
The influence of perinatal factors on the pRNFL sectors, the global pRNFL and MRW as well as the BMO was analyzed using a multivariable analysis model adjusted for age (years), sex (female), GA (groups), birthweight percentile (groups) and axial length (mm) and sequentially each of the following variable separately: ROP (groups), perinatal adverse events, maternal smoking during pregnancy, preeclampsia, placental insufficiency, and breastfeeding.
Because this is an explorative study, a significance level was not defined and no adjustment for multiple testing was conducted; thus P values were reported only for descriptive purposes and should be interpreted with caution.29 Calculations were performed using R (R Core Team [2021]; R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria, URL https://www.R-project.org/, R version 4.1.2 [2021-11-01]).
Results
Participant Characteristics
This study included 1546 eyes of 793 participants born preterm and full-term (mean age = 11.41 years, 418 female subjects). Overall, 502 eyes of 257 participants with a GA ≥ 37 weeks (group 1, control group), 474 eyes of 240 participants with a GA between 33 and 36 weeks without ROP (group 2), 318 eyes of 164 participants with a GA between 29 and 32 weeks without ROP (group 3), 136 eyes of 70 participants with a GA ≤ 28 weeks without ROP (group 4), 99 eyes of 53 participants with a GA between 24 and 32 weeks with ROP without treatment (group 5), and 17 eyes of nine participants with a GA between 24 and 32 weeks and with postnatal laser or anti-VEGF treatment for ROP (group 6) were assessed and their characteristics are summarized in Table 1. Of the participants treated for ROP, one received anti-VEGF treatment whereas the others received photocoagulation treatment.
Descriptive Sectorial Papillary Measures
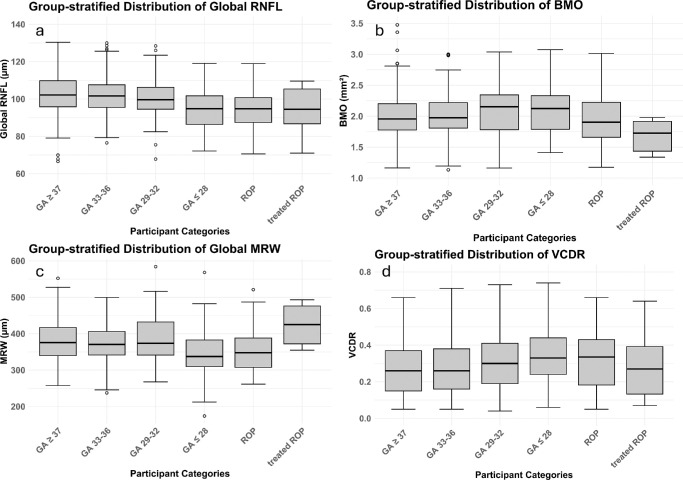
Descriptive sectorial measurements for pRNFL, BMO area, and MRW are displayed in Table 2 with graphs presented in the Figure and Supplementary Figure S2. In multivariable linear regression analyses GA ≤ 28 weeks was associated with thinner pRNFL globally (β = −9.25, P < 0.001) and in all sectors with exception of the temporal one (all P < 0.001). GA between 29 and 32 weeks was only associated with the thinning of the temporal (β = −2.83, P = 0.02) and nasal sector (β = −3.49, P = 0.03). A birth weight percentile <25 was also associated with thinning of all sectors as well as globally, apart from the temporal sector (global β = −3.77, P < 0.001). Furthermore, ROP treatment was associated with a thicker pRNFL in the temporal (β = 43.31, P < 0.001) and inferotemporal sectors (β = 20.97, P = 0.04). Perinatal adverse events were associated with a thinner pRNFL globally (β = −7.68, P < 0.001) and in all three nasal sectors (P < 0.001). Maternal smoking during pregnancy was associated with thinner inferonasal pRNFL (β = −12.02, P = 0.003) and breastfeeding was associated with a thicker global pRNFL (β = 2.25, P = 0.02), as well as in the inferonasal and superonasal sectors. Results from the pRNFL-association analyses are displayed in Table 3.
Descriptive group-stratified distribution of the optic nerve head parameters. (a) Global retinal nerve fiber layer. (b) Area of the Bruch's membrane opening. (c) Global minimum rim width. (d) Vertical cup-to-disc ratio in both eyes. BMO, Bruch's membrane opening; GA, gestational age; MRW, minimum rim width; RNFL, here: peripapillary retinal nerve fibre layer; ROP, retinopathy of prematurity; VCDR, vertical cup to disc ratio.
Association analyses with global MRW in the multivariable model, adjusted for age, sex and axial length did not show any association with different perinatal parameters. However, in temporal sectors, individuals treated for ROP showed a larger MRW (inferotemporal β = 75.99, temporal β = 97.44 and superotemporal β = 74.40, all P < 0.008). Furthermore, individuals born extremely preterm showed a smaller MRW in both inferior sectors (inferotemporal β = −30.36 and inferonasal β = −28.85, all P ≤ 0.02). Association analyses of BMO-area revealed only a marginal association with GA 29–32 weeks when adjusted for age, sex, and axial length (β = 0.13; 95% CI, 0.01–0.25; P = 0.04) (Table 4).
Linear Quantile Mixed Model Association Analyses of the Vertical Cup-to-Disc Ratio
The linear quantile mixed model showed that VCDR was associated with extremely preterm birth (β = 0.05; 95% CI, 0.003–0.09; P = 0.04), as well as moderate preterm birth (β = 0.05; 95% CI, 0.009–0.09; P = 0.02) and preeclampsia (β = 0.05; 95% CI, 0.019–0.08; P < 0.001) in the univariable analyses (Supplementary Table S1). The association with extreme prematurity (β = 0.05; 95% CI, 0.02–0.08; P = 0.001) and moderate prematurity (β = 0.04; 95% CI, 0.01–0.06; P = 0.004) persisted, and perinatal adverse events (β = 0.05; 95% CI, 0.01–0.09; P = 0.02) were also associated with a larger VCDR after adjustment in the multivariable analyses adjusted for sex, age, axial length and optic disc area. None of the other parameters revealed an association in multivariable analyses. A sensitivity analysis with exclusion of the 15 cases with PVL did show similar results.
Discussion
This is the first study to comprehensively assess the optic nerve head characteristics pRNFL, BMO area, MRW, and VCDR in a combined approach in a large cohort of children aged four to 17 years of age with and without previous ROP and ROP treatment. This analysis revealed that the main perinatal parameters leading to a thinner pRNFL were extreme prematurity and a birth weight percentile <25, whereas individuals treated for ROP displayed a thicker pRNFL in temporal and inferotemporal sectors. Furthermore, individuals affected by adverse perinatal events had a thinner pRNFL in all nasal sectors, individuals who had records of maternal smoking had a thinner inferonasal pRNFL and individuals who were breastfed had greater pRNFL-thickness globally, as well as in the inferonasal and superonasal sectors.
The pRNFL results are in line with results of previous assessments in children3^,^13^,^14 and adults born preterm,4 which found the pRNFL to be thinner in all but temporal sectors. However, the current study results in children revealed that only extreme prematurity (GA ≤ 28 weeks) was associated with a thinner pRNFL. This may be explained by changes in neonatal care with the introduction of antenatal corticosteroids, surfactant therapy, and high-frequency ventilation,30 which could have prevented the impaired development of neuronal tissue measured by pRNFL thickness in individuals born only moderately preterm but not have had sufficient effect on children born extremely preterm. The effect estimators of GA on global pRNFL thickness support this hypothesis.4 The larger VCDR, which we observed in children born more preterm, is also in line with the general thinning of the pRNFL in those individuals and has also been described in previous studies of children and adults.6^,^13 This analysis suggested that median VCDR was only associated with extreme and moderate prematurity, as well as perinatal adverse events after adjustment.31
The results regarding a thinner pRNFL with extreme prematurity are also in line with the MRW results, which tended to be thinner in children born extremely preterm. However, this was only significant in inferior sectors (inferotemporal, inferonasal) but is in line with the results by Wenner et al.13 who reported a significantly thinner rim area in children born preterm and an even smaller rim area in children born preterm with brain injury, after adjusting for spherical equivalent, birth weight, GA, bronchopulmonary dysplasia and ROP. The present study also revealed that individuals who experienced perinatal adverse events (comprising individuals with intraventricular hemorrhage) had a thinner pRNFL globally, especially in the nasal sectors. Both perinatal adverse events as well as maternal smoking affect neurodevelopment32^,^33 which might indirectly affect the pRNFL thickness, whereas breastfeeding had positive effects on brain development in a previous study,34 possibly explaining the findings with respect to pRNFL thickness. One mechanism behind the changes in optic nerve head anatomy in extremely preterm children could be retrograde transynaptical degeneration, which, following neurological injuries due to preterm birth such as PVL or other smaller white matter injuries, might explain the reason for the thinner pRNFL.35 VCDR analyses did not differ after exclusion of participants with PVL, highlighting the sole effects of immaturity. This is supported by further research showing that even children born preterm without major cerebral pathology revealed a decrease in both gray and white matter tissue.31
Regarding the BMO area, Lee et al.14 found no correlation between GA and BMO diameter in their group of preterm individuals. Likewise, the BMO area in the present study was only marginally associated with moderately preterm birth but no other factors tested, suggesting that BMO is independent of prenatal factors including GA and birth weight.
A thicker pRNFL was observed in the temporal sectors of individuals treated for ROP in both adults and now in children, which is in line with the results from previous studies,14^,^36^,^37 although not all studies differentiated between ROP and ROP treatment. Furthermore, individuals treated for ROP showed a significantly larger MRW in all temporal sectors in our analyses, which supports the findings of a larger pRNFL. This alteration might be the result of a redistribution from the superior sector (which was also reduced in our cohort) to the temporal sector along with the migration disorder of the macula and increased foveal thickness.4^,^38^,^39
Strengths and Limitations
This study is limited by its single-center and hospital-based design. Not all participants who were approached participated in the study, and missing contact details might have resulted in selection bias. Furthermore, some of the younger children especially children with extreme prematurity might have had problems with fixation, which could have biased our assessments. Although children with treated ROP were examined, this group is rather small, and there were different types of treatments (laser-treatment vs. anti-VEGF medication) within the group, although most children received treatment by photocoagulation. It also needs to be acknowledged that groups with treated ROP had higher stages of ROP and higher proportions of Plus Disease, which may have influenced the results more than the actual treatment. A sensitivity analysis with exclusion of participants with plus disease was not conducted because of the low number of affected participants which could also limit our analysis. Furthermore, the number of participants who were affected by bronchopulmonary dysplasia, intraventricular hemorrhage, and necrotizing enterocolitis was low, and therefore we summarized these as adverse events instead of assessing the effects for each event solely. Unfortunately, we are therefore unable to draw any conclusions about the effects of the individual diseases. Furthermore, the proportion of images that could not be assessed was rather high in the groups with ROP and treated ROP, which is a result of fixation instabilities and a higher proportion of developmental delays in these groups. Additionally, children born preterm have increased refractive errors which could also limit our analyses, although we adjusted our analyses for axial length and there were no cases of extremely high myopia in this cohort. The range of spherical equivalent in our included participants was −10.79 D to 7.40 D; therefore our findings may not necessarily generalize to children with even higher degrees of ametropia. Also, because prematurity, low birthweight, and several other parameters are interrelated, we performed multivariable analyses adjusting for these potential confounders. Although the association between RNFL thickness and breastfeeding remained significant, residual bias cannot be fully excluded, and the results should be interpreted with caution.
Nonetheless, this is one of the largest cohorts assessing children over a wide age span with and without ROP and ROP treatment, enabling the investigation of children born preterm without ROP. Because this is a combined prospective and retrospective cohort study, perinatal factors were assessed and integrated into the analyses of current outcomes. Investigators were blinded, and data quality was ensured by standardized examination and analysis procedures to minimize bias.
Conclusions
In conclusion, the results of this study suggest that prematurity, especially extreme prematurity, leads to a thinner pRNFL and a larger VCDR measure, and in turn, advanced ROP stages and need for ROP treatment lead to a thicker pRNFL in temporal sectors in line with MRW results, indicating that children after treatment for ROP may have a thicker MRW in all temporal sectors. In addition, the results showed that in this study, perinatal adverse events and maternal smoking during pregnancy negatively affected pRNFL thickness, suggesting a reduced pRNFL capacity and a potentially greater risk of developing age-related neurodegenerative diseases in these cases, whereas children who were breastfed as infants had a thicker pRNFL and therefore may have a greater reserve pRNFL capacity to protect against age-related pRNFL thinning.
Supplementary Material
Supplement 1
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Howson CP, Kinney MV, Lawn JE. Born Too Soon: The Global Action Report on Preterm Birth. March of Dimes, PMNCH, Save the Children. Available at: https://assets.publishing.service.gov.uk/media/57a 08a 76e 5274 a 27b 20005 e 3/201204_borntoosoon-report.pdf. Accessed February 8, 2019.
- 2Rothman AL, Sevilla MB, Mangalesh S, et al. Thinner retinal nerve fiber layer in very preterm versus term infants and relationship to brain anatomy and neurodevelopment. Am J Ophthalmol. 2015; 160: 1296–1308.26386157 10.1016/j.ajo.2015.09.015PMC 4651865 · doi ↗ · pubmed ↗
- 3Fiess A, Christian L, Janz J, et al. Functional analysis and associated factors of the peripapillary retinal nerve fibre layer in former preterm and full-term infants. Br J Ophthalmol. 2017; 101: 1405–1411.28274943 10.1136/bjophthalmol-2016-309622 · doi ↗ · pubmed ↗
- 4Fiess A, Schäffler A, Mildenberger E, et al. Peripapillary retinal nerve fiber layer thickness in adults born extremely, very, and moderately preterm with and without ROP: results from the Gutenberg Prematurity Eye Study (GPES). Am J Ophthalmol. 2022; 244: 88–97.35932823 10.1016/j.ajo.2022.07.019 · doi ↗ · pubmed ↗
- 5Akerblom H, Holmstrom G, Eriksson U, Larsson E. Retinal nerve fibre layer thickness in school-aged prematurely-born children compared to children born at term. Br J Ophthalmol. 2012; 96: 956–960.22569283 10.1136/bjophthalmol-2011-301010 · doi ↗ · pubmed ↗
- 6Fiess A, Gissler S, Mildenberger E, et al. Optic nerve head morphology in adults born extreme, very and moderate preterm with and without retinopathy of prematurity: results from the Gutenberg Prematurity Eye Study. Am J Ophthalmol. 2022; 239: 212–222.35288076 10.1016/j.ajo.2022.03.005 · doi ↗ · pubmed ↗
- 7Tong AY, El-Dairi M, Maldonado RS, et al. Evaluation of optic nerve development in preterm and term infants using handheld spectral-domain optical coherence tomography. Ophthalmology. 2014; 121: 1818–1826.24811961 10.1016/j.ophtha.2014.03.020PMC 4145027 · doi ↗ · pubmed ↗
- 8Alshaarawi S, Shatriah I, Zunaina E, Wan Hitam WH. Assessment of the optic nerve head parameters using Heidelberg retinal tomography III in preterm children. P Lo S One. 2014; 9(2): e 88056.24551076 10.1371/journal.pone.0088056 PMC 3923764 · doi ↗ · pubmed ↗