The effect of smart pillboxes on TB stigma among adults in a cluster-randomised TB treatment trial
L. Jennings, N. Maraba, R. Mukora, P. Hippner, K. Velen, C. Orrell, S. Charalambous, K. Fielding

TL;DR
This study found that TB stigma was low among adults in South Africa, and using smart pillboxes did not increase stigma during treatment.
Contribution
The study quantitatively evaluates TB stigma during treatment and assesses the impact of smart pillboxes on stigma.
Findings
Baseline experience of TB stigma or internalised stigma was low (≤3%).
Disclosure of TB status outside the household was common (42.3%).
Use of smart pillboxes did not increase TB stigma during treatment.
Abstract
TB stigma has been shown to result in delayed health-seeking behaviours and treatment initiation. Few studies have quantitatively described stigma during treatment. As part of the TB Mate trial, we summarise TB stigma at treatment start and the effect of the intervention on stigma in follow-up. In the TB Mate trial, we conducted a cluster-randomised trial in 18 primary health care facilities from three provinces in South Africa to evaluate the use of alarmed electronic pillboxes in drug-sensitive TB on treatment adherence. We administered a questionnaire, measuring five TB stigma domains, at baseline, 6 months, and 18 months. We conducted a sub-analysis of these stigma data. Overall, 2,469/2,657 adults with TB enrolled had a baseline stigma questionnaire. At baseline, reporting experience of stigma or internalised stigma was low (≤3%), whereas disclosure of TB status outside of the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
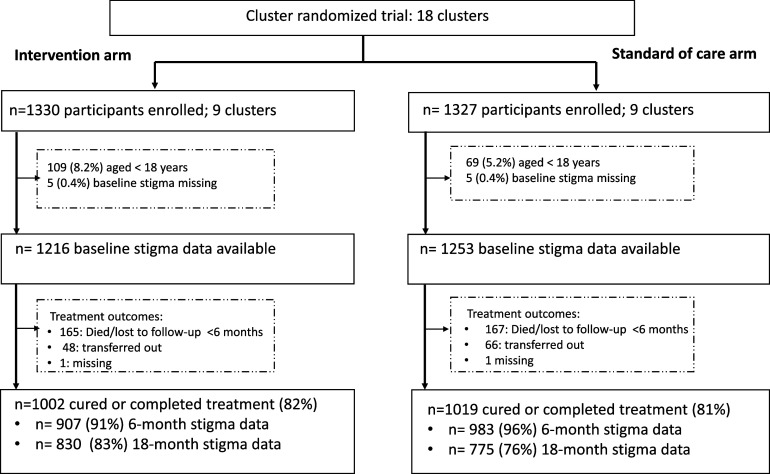 Figure 1
Figure 1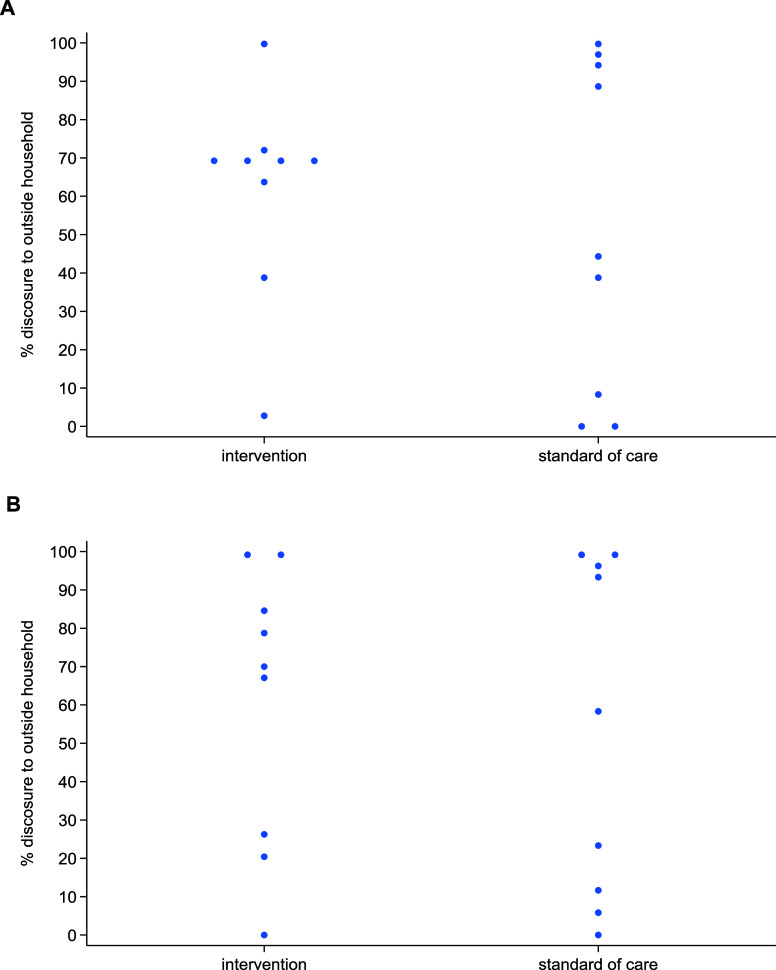 Figure 2
Figure 2| Since you have fallen ill with TB, have you experienced any of the following | |
|---|---|
| Social exclusion domain | At least one of |
| 1. Been excluded from a social gathering | Yes/No |
| 2. Abandoned by spouse/partner | Yes/No |
| 3. Isolated by your household | Yes/No |
| 4. Your children or family have been isolated/shunned | Yes/No |
| Been made fun of domain | At least one of |
| 5. Lost respect or standing in the community | Yes/No |
| 6. Been teased, insulted, or sworn at | Yes/No |
| 7. Been gossiped about | Yes/No |
| Health-setting stigma domain | |
| 8. Been treated worse than patients with other diseases by health staff | Yes/No |
| Internalised stigma domain | |
| 9. Unclean or dirty because of your TB | Yes/No |
| Disclosure domain | |
| 10. Did you tell or have you told anyone outside of your household about your TB diagnosis? | Yes/No |
| Intervention | SOC | Total | ||
|---|---|---|---|---|
| n = 1,216 | n = 1,253 | n = 2,469 | ||
| Country or origin | South Africa | 1,184 (97.4%) | 1,189 (94.9%) | 2,373 (96.1%) |
| Sex | Male | 783 (64.4%) | 768 (61.3%) | 1,551 (62.8%) |
| Female | 433 (35.6%) | 485 (38.7%) | 918 (37.2%) | |
| Ethnicity | Black African | 1,089 (89.6%) | 1,194 (95.3%) | 2,283 (92.5%) |
| Age, years | Median (Q1, Q3) | 37 (29, 47) | 36 (29, 46) | 36 (29-46) |
| Education | ≤Grade 7 | 195 (16.0%) | 238 (19.0%) | 433 (17.5%) |
| Grade 8–11 | 536 (44.1%) | 527 (42.1%) | 1,063 (43.1%) | |
| ≥Grade 12 | 485 (39.9%) | 488 (38.9%) | 973 (39.4%) | |
| Marital status | Single | 829 (68.2%) | 946 (75.5%) | 1,775 (71.9%) |
| Married/cohab | 324 (26.6%) | 246 (19.6%) | 570 (23.1%) | |
| Divorced/widowed | 63 (5.2%) | 61 (4.9%) | 124 (5.0%) | |
| HIV/ART status | Negative | 610 (50.2%) | 449 (35.8%) | 1,059 (42.9%) |
| Pos, not on ART | 278 (22.9%) | 399 (31.8%) | 677 (27.4%) | |
| Pos, on ART | 268 (22.0%) | 393 (31.4%) | 661 (26.8%) | |
| Unknown | 60 (4.9%) | 12 (1.0%) | 72 (2.9%) | |
| Previous TB | Yes | 307 (25.2%) | 295 (23.5%) | 602 (24.4%) |
| TB diagnosis | Bacteriological positive | 997 (82.1%) | 892 (71.3%) | 1,889 (76.6%) |
| Province | Gauteng | 431 (35.4%) | 343 (27.4%) | 774 (31.3%) |
| KwaZulu-Natal | 356 (29.3%) | 434 (34.6%) | 790 (32.0%) | |
| Western Cape | 429 (35.3%) | 476 (38.0%) | 905 (36.7%) | |
| Stigma domains | ||||
| Social exclusion | Yes | 15 (1.2%) | 26 (2.1%) | 41 (1.7%) |
| Made fun of | Yes | 25 (2.1%) | 26 (2.1%) | 51 (2.1%) |
| Health-setting stigma | Yes | 3 (0.2%) | 9 (0.7%) | 12 (0.5%) |
| Internalised stigma | Yes | 37 (3.0%) | 23 (1.8%) | 60 (2.4%) |
| Disclosure | Yes | 544 (44.7%) | 501 (40.0%) | 1,045 (42.3%) |
| SOC | Intervention | Crude PR (95% CI) | |||||
|---|---|---|---|---|---|---|---|
| n (%) | GM, % | # clusters with zero outcomes | n (%) | GM, % | # clusters with zero outcomes | ||
| At 6 months | N = 983 | N = 9 | N = 907 | N = 9 | |||
| Social exclusion | 8 (0.8%) | — | 6 | 13 (1.5%) | — | 4 | — |
| Made fun of | 29 (3.0%) | 1.4% | 5 | 44 (4.9%) | 3.1% | 1 | 2.29 (0.65–8.06) |
| Health-setting stigma | 2 (0.2%) | — | 8 | 1 (0.1%) | — | 8 | — |
| Internalised stigma | 11 (1.2%) | — | 7 | 45 (5.0%) | — | 6 | — |
| Disclosure | 547 (56%) | 20% | 2 | 576 (64%) | 49% | 0 | 2.46 (0.46–13.2) |
| At 18 months | N = 775 | N = 830 | |||||
| Social exclusion | 3 (0.4%) | — | 7 | 9 (1.1%) | — | 4 | — |
| Made fun of | 6 (0.8%) | 1.1% | 5 | 25 (3.0%) | 1.7% | 4 | 1.66 (0.56–4.94) |
| Health-setting stigma | 2 (0.3%) | — | 8 | 7 (0.8%) | — | 7 | — |
| Internalised stigma | 11 (1.4%) | — | 5 | 38 (4.6%) | — | 4 | — |
| Disclosure | 434 (56%) | 28% | 0 | 519 (63%) | 37% | 1 | 1.30 (0.27–6.29) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHIV/AIDS Research and Interventions · Tuberculosis Research and Epidemiology · Bipolar Disorder and Treatment
South Africa has one of the highest TB burdens in the world, with an estimated incidence of 468 per 100,000 population in 2022, and HIV prevalence among people with TB of 54%.^1^ Stigma related to TB has been described worldwide and consists of several domains, including internalised, experienced, and anticipated or perceived stigma.^2^ Combating TB stigma and discrimination is one of the World Health Organization’s (WHO) 10 priority recommendations for ending TB.^3^ Despite this, TB stigma in South Africa is not well understood. While qualitative research has extensively described TB stigma in South Africa, it cannot be used to determine the prevalence.^4,5^ Many scales and tools for the measurement of TB stigma exist, but there is a lack of consensus on which tools should be used and which domains of stigma should be covered.^6–8^ To date, only one TB stigma scale, which covers the domain of perceived stigma, has been validated for use in South Africa.^7^ However, qualitative exploration of this tool found that it overestimated the prevalence of stigma.^9^ Other tools, such as the ZAMSTAR and Stop TB Partnership tools, cover multiple domains of stigma.^10,11^ A systematic review has shown that perceived TB stigma results in delayed health-seeking behaviours and treatment initiation^12^; however, this effect has not always been shown^13,14^ and the strength of these associations has been difficult to quantify.^2^
Digital adherence technologies (DATs), such as smart pillboxes and video-supported therapy, have increasingly been evaluated as an approach to improve treatment adherence and outcomes among people with TB. DATs have a conditional recommendation from WHO.^15–17^ There is a concern, however, that these technologies may have an impact on the privacy and confidentiality of people with TB, which may result in increased stigma.^17,18^ A scoping review of contextual factors influencing implementation of DATs among people with TB found that DATs both lowered and increased stigma, with some finding it provided more privacy and others finding it increased visibility of TB treatment.^17^
As a sub-analysis of a large cluster-randomised trial of smart pillboxes conducted in South Africa among people with drug-sensitive TB, we administered the ZAMSTAR TB stigma questionnaire at three timepoints: baseline (treatment start), 6 months (end of treatment), and 18 months. This study aimed to 1) describe the prevalence of TB stigma at treatment start and 2) explore whether the DAT intervention increased TB stigma at 6 and 18 months, versus routine care, among those who were cured or completed treatment.
METHODS
These data are from a cluster-randomised trial conducted in 18 primary health care facilities (clusters) from three provinces (Gauteng, KwaZulu-Natal, and Western Cape) in South Africa between May 2019 and February 2022.^19^ Clusters were allocated to the intervention or standard of care arm (1:1), using unstratified randomisation. The study enrolled adults and children aged 2–17 years with drug-sensitive TB, who had initiated treatment within the past 14 days at the health care facilities. All participants/caregivers were issued a smart pillbox at study enrolment, which recorded pillbox openings in real-time. In the intervention arm, the device had daily reminder alarms, which sounded at a specified time as reminders to participants to take their medication, and visual appointment reminders in the form of coloured lights indicating when clinic visits were near or due. The devices were monitored in real-time by research staff, and participants received either a text message, a phone call, or a home visit, depending on the number of times the box was not opened. In the standard of care arm, the devices were in silent mode and were not monitored in real-time. Participants were dispensed medication by clinic staff under routine care and seen by research staff at these routine visits for additional data collection for the trial. At study enrolment, socio-demographic data were collected by self-report. The treatment outcome was abstracted from the TB register. A research follow-up visit at the health facility was planned to coincide with the end of treatment (6 months) to collect a sputum specimen for culture to enhance trial endpoint measurement. In addition, participants whose treatment outcome was cured or completed treatment were followed up by research staff until 18 months after study enrolment to measure TB recurrence. The trial’s primary outcome was treatment adherence using a proxy of pillbox openings, in both arms. Secondary outcomes included poor end of treatment outcome (death, lost to follow-up, and treatment failure) and a combined measure of poor end of treatment outcome or TB recurrence by 18 months. The DAT intervention improved treatment adherence, and secondary outcomes were similar by arm.^20^
Stigma scale
We used the TB stigma scale developed from the ZAMSTAR study in South Africa and Zambia.^10^ This tool was chosen due to its recent development and assessment in sub-Saharan Africa at the time the TB Mate trial was being planned. The stigma scale aimed to address gaps in existing TB scales and to ensure coverage of the following five domains of TB stigma: experience with social exclusion (four questions), experience of being made fun of (three questions), experience with health-setting stigma (one question), internalised stigma (one question), and disclosure of TB status (one question). Each of the five domains was recorded as a binary outcome, with social exclusion and experience of being made fun of, assigned a positive score if at least one question was answered yes (Table 1). Domains were analysed separately. The questionnaire was administered by research staff to all study participants aged 15 years and above at baseline (start of TB treatment), 6 months (end of TB treatment), and 18 months (end of study). For the latter, this was restricted, by design, to those who had cured/completed treatment, in order to measure TB recurrence. The 6-month end of treatment measure coincided with the routine end of treatment clinic visit, and in order not to interfere with the measurement of trial secondary treatment outcomes, no attempt was made by research staff to actively follow up participants who had not attended this clinic visit. Therefore, stigma data were unlikely to have been measured for those that had been transferred out to another clinic, died, or been lost to follow-up on treatment.
Analysis population
We restricted analyses to trial participants aged 18 years and above with at least the baseline stigma questionnaire completed. Analysis of stigma scores at 6 and 18 months was limited to those who had a treatment outcome of cured or completed treatment at 6 months.
Statistical analysis
All analyses were conducted in Stata (version 18).^21^ At the 6 and 18 month follow-up visits, the five domains were summarised by study arm, restricted to those that had cured or completed treatment. The effect of the study arm on the 6- and 18-month stigma scores was analysed at the cluster level due to the small number of clusters.^22^ The effect estimate was the prevalence ratio (PR) based on the natural logarithm-transformed prevalences, compared by study arm across clusters using a t test. For clusters with zero events, 0.5 was added to the numerator for all clusters. An adjusted analysis was also conducted, controlling for imbalances of individual-level variables at baseline, using a two-stage approach, where there was a reasonable number of events. The first stage used logistic regression at the individual level including all baseline covariates that had imbalance by study arm, excluding arm; observed and expected number of outcomes were generated for each cluster. At the second stage, the log of the cluster-level residual (observed/expected number of events) was compared by study arm across clusters using a t test. Analysis of the stigma domains’ experience with social exclusion, health-setting stigma, and internalised stigma was not attempted due to a small number of events. The Stata ‘clan’ command was used for this analysis.^23^
Ethical statement
This study was approved by the University of Witwatersrand (180705), the University of Cape Town Human Research Ethics Committee (452/2018), and the London School of Hygiene & Tropical Medicine (16107). Permission to conduct the study in health facilities was obtained from local health authorities. Written informed consent was obtained from study participants prior to data collection.
RESULTS
Overall, 2,657 persons with TB enrolled into the TB Mate trial, of whom 178 (6.7%) were aged <18 years and 10 had missing baseline stigma questionnaire, leaving 2,469 (1,216 and 1,253 in the intervention and standard of care arms, respectively) participants contributing to subsequent analyses (Figure 1). Of these participants, 37% (918/2,469) were female, the median age was 36 years (interquartile range 29–46 years), and 44%, 28%, and 28% were HIV negative (1,059/2,397), positive not on ART (677/2,397), and positive on ART (661/2,397), respectively (Table 2). At the end of treatment, 82% (2,021/2,469) of participants were defined as cured or completed treatment, 13% (332/2,469) were classified as having poor treatment outcome (treatment failure, died, or lost to follow-up), 5% (114/2,469) had been transferred out to another facility, and two participants had missing end of treatment outcome (Figure 1).
CONSORT flow chart of participants’ disposition throughout study participation.
At baseline, the percentage of participants reporting experience of social exclusion, being made fun of, health-setting stigma, and internalised stigma was low (≤3%), and similar by arm. Overall 42.3% (1,045/2,469) of participants reported disclosing their TB diagnosis to anyone outside of their household: 40.0% in the standard of care arm and 44.7% in the intervention arm. Experience of social exclusion and experience of being made fun of were more commonly reported among participants enrolled in KwaZulu-Natal (3% [24/790] and 4% [32/790], respectively) than Gauteng (<1% [6/774] and <1% [4/774], respectively) or Western Cape (1% [11/905] and 2% [15/905], respectively). Disclosure was most common in Western Cape (61%, 553/905), followed by KwaZulu-Natal (36%, 284/790) and Gauteng (27%, 208/774) – see Supplementary Data Table S1.
At the end of treatment, 81.9% (2,021/2,469) had a treatment outcome of cured or completed treatment, and of these 93.5% (1,890/2,021) and 79.4% (1,605/2,021) had completed the stigma questionnaire, at 6 and 18 months, respectively. Non-attendance at the 18-month visit (resulting in missing stigma data at this visit) was less common for those with education grade 12 and above, HIV negative or HIV positive on ART, the intervention arm, and participants from Gauteng and KwaZulu-Natal provinces (Supplementary Data Table S3).
At 6 months, reporting experience of social exclusion, being made fun of, health-setting stigma, and internalised stigma was uncommon (Table 3). Disclosure had increased from baseline: 64% (576/907; geometric mean [GM] of cluster-level proportions 49%) reported disclosure in the intervention arm compared with 56% (547/983; GM of cluster-level proportions 20%) in the standard of care arm, giving an adjusted PR of 2.55 (95% confidence interval [CI] 0.50–12.90), adjusting for age, sex, type of TB diagnosis, ethnicity, marital status, and HIV/anti-retroviral status. There was considerable variability of reporting disclosure by cluster (Figure 2). Participants' experience of being made fun of was higher in those enrolled in KwaZulu-Natal than those in other provinces at 6 months. (6%; 42/605). Disclosure was most common in KwaZulu-Natal (73%, 367/710) (Supplementary Data Table S1B). At 18 months, disclosure was similar by arm with an adjusted PR of 1.36 (95% CI 0.32–5.89).
A: disclosure at 6 months, at the cluster level (n = 1,890); B: disclosure at 18 months, at the cluster level (n = 1,605).
DISCUSSION
This sub-analysis of a large cluster-randomised TB adherence study using smart pillboxes aimed to describe (among adults with DS-TB) the prevalence of TB stigma at treatment start and the effect of the alarmed DAT intervention on stigma at 6 and 18 months from treatment start. We found that the prevalence of the TB stigma domains of experience of social exclusion, being made fun of, health-setting stigma, and internalised stigma was low at baseline, in both arms. There was no effect of the alarmed DAT on reported stigma in these domains at the end of treatment, among the subgroup who had cured/completed treatment. Stigma domains were highly variable across clusters.
Bresenham et al.^8^ described an association between health district and stigma and, in our study, we found that disclosure rates at 6 months showed great variability by cluster. Although this finding may be due to data collection discrepancies across sites, the influence of local context on stigma has been emphasised in multiple studies^10,24–26^ and highlights the need for interventions that are multi-faceted and adaptable to different settings. Bond et al.^10^ found low prevalence of experience of social exclusion, being made fun of, and internalised stigma in South Africa, which is consistent with our findings. Low prevalence of health-setting stigma has also been described elsewhere.^10,27^ Similarly to our study, Bond et al.^10^ also found that disclosure of TB status was high at baseline and, as they noted, the relationship between stigma and disclosure is complex. While disclosure can indicate that a participant felt comfortable to do so, it can also increase the risk of the participant experiencing stigma. We did not see a difference in stigma in the intervention arm, in which the pillboxes used had audio and visual alarms, and the control group, in which the pillboxes were in silent mode. These results are not surprising given a review of contextual factors influencing implementation of DATs in TB, which showed that DATs are likely to both increase and decrease stigma depending on the context in which they are being used.^17^ This is supported by the great variability in stigma seen by cluster.
There are several limitations to this study. Baseline stigma assessment was conducted primarily at the time of starting TB treatment with individuals not having yet had the experience of taking treatment at home. It may have been more appropriate to assess baseline stigma within the first few weeks of treatment. Our analyses at 6 and 18 months were limited to participants who were cured or who had completed treatment, limiting the generalisability of our findings; we cannot comment on stigma in those who had treatment failure, died, or were lost to follow-up. This group is important to understanding the effects of stigma, but our study design did not allow us to measure stigma at these time points. Although the baseline characteristics were similar in both arms, variability of TB disclosure in clusters indicates that there are factors influencing this domain which require further study. High variability between clusters and low prevalence of stigma outcomes resulted in low power to detect differences between arms. Additionally, this was a sub-analysis of a study powered for adherence outcomes^20^ and was therefore not powered to detect differences in stigma outcomes by study arm.
Our findings show that the prevalence of TB stigma, in domains other than disclosure, in our study population was low; however, the lack of standardised tools makes this difficult to compare across studies. There was no evidence that using the DAT in active versus silent mode increased stigma in the domains of experience of social exclusion, being made fun of, health-setting stigma, or internalised stigma in people who were cured or completed TB treatment. Future research should focus on the standardisation of TB stigma measures to properly assess the impact of stigma-related interventions. Measures need to be adaptable as the prevalence of TB stigma varies by context. In addition, future studies should assess the association between TB stigma and treatment outcomes.
Supplementary Material
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1World Health Organization. Global tuberculosis report. Geneva: WHO, 2024. https://www.who.int/teams/global-tuberculosis-programme/tb-reports/global-tuberculosis-report-2024 (Accessed 2 February 2025).
- 2Courtwright A, Turner AN. Tuberculosis and stigmatization: pathways and interventions. Public Health Rep. 2010;125(Suppl 4):34-42.20626191 10.1177/00333549101250 S 407PMC 2882973 · doi ↗ · pubmed ↗
- 3World Health Organization. Implementing the end TB strategy: the essentials, 2022 update. Geneva: WHO, 2022.
- 4De Santo D, A qualitative exploration into the presence of TB stigmatization across three districts in South Africa. BMC Public Health. 2023;23(1):504.36922792 10.1186/s 12889-023-15407-2PMC 10017062 · doi ↗ · pubmed ↗
- 5Hayward SE, “As a patient I do not belong to the clinic, I belong to the community”: co-developing multi-level, person-centred tuberculosis stigma interventions in Cape Town, South Africa. BMC Glob Public Heal. 2024;2(1):55.10.1186/s 44263-024-00084-z PMC 1132478339157720 · doi ↗ · pubmed ↗
- 6Nuttall C, Interventions pathways to reduce tuberculosis-related stigma: a literature review and conceptual framework. Infect Dis Poverty. 2022;11(1):101.36138434 10.1186/s 40249-022-01021-8PMC 9502609 · doi ↗ · pubmed ↗
- 7Bajema KL, Tuberculosis-related stigma among adults presenting for HIV testing in Kwa Zulu-Natal, South Africa. BMC Public Health. 2020;20(1):1338.32883251 10.1186/s 12889-020-09383-0PMC 7469347 · doi ↗ · pubmed ↗
- 8Bresenham D, Kipp AM, Medina-Marino A. Quantification and correlates of tuberculosis stigma along the tuberculosis testing and treatment cascades in South Africa: a cross-sectional study. Infect Dis Poverty. 2020;9(1):145.33092636 10.1186/s 40249-020-00762-8PMC 7579945 · doi ↗ · pubmed ↗