Beyond Gastroenteritis: A Case of Salmonella Infection Leading to Adrenal Insufficiency
Thwe Thwe Wint Htal, Aye Pyae Tin Hla, Aye Moh Moh Paing, Kyaw Thura, Clare Pollard

TL;DR
A rare case of adrenal insufficiency caused by a Salmonella infection in a healthy young man is reported, emphasizing the need for early diagnosis.
Contribution
This case report highlights an uncommon cause of adrenal insufficiency in an immunocompetent individual.
Findings
A 20-year-old male developed bilateral adrenal abscesses from Salmonella Saintpaul infection.
Adrenal insufficiency occurred secondary to disseminated Salmonella infection.
The case underscores the importance of considering adrenal involvement in septic patients with unexplained symptoms.
Abstract
Primary adrenal insufficiency (PAI), or Addison’s disease, is a rare and potentially life-threatening condition that requires prompt diagnosis and management. While most cases are autoimmune, other causes include infections such as Salmonella, though this is rarely reported. We describe a case of bilateral adrenal abscesses and adrenal insufficiency secondary to disseminated Salmonella Saintpaul infection in a previously healthy 20-year-old male following travel to Thailand. This case highlights the importance of early recognition of adrenal involvement in septic patients with persistent fever and electrolyte imbalances, even in immunocompetent individuals.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1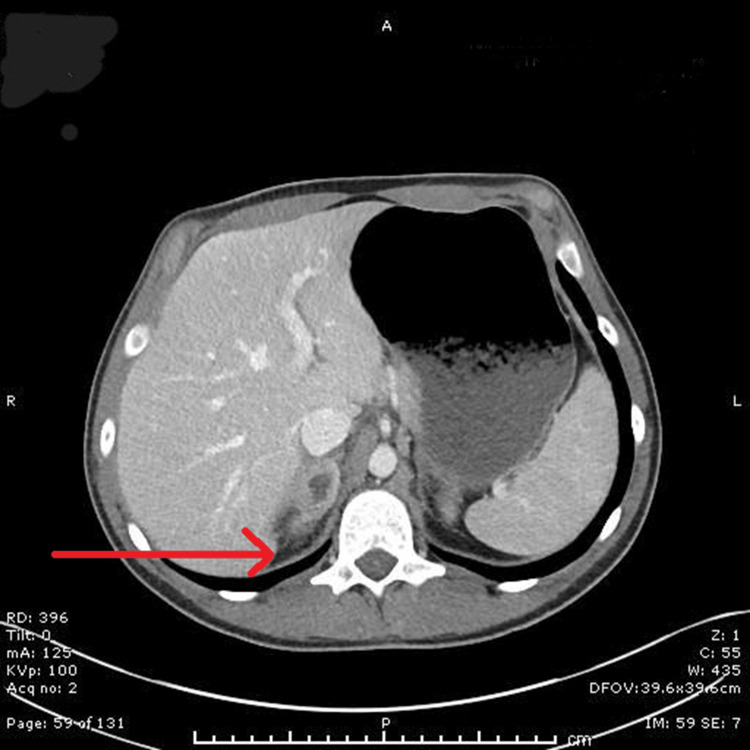 Figure 2
Figure 2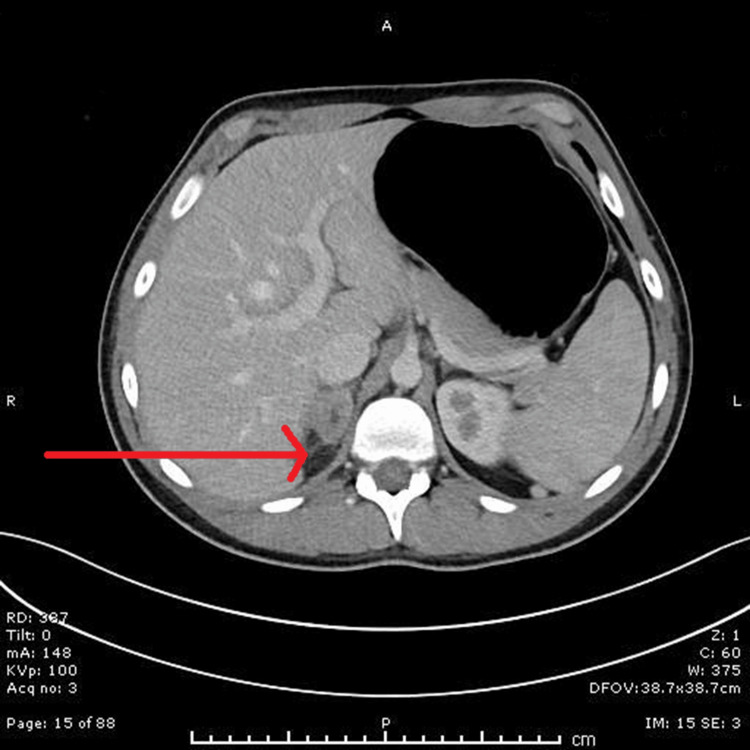 Figure 3
Figure 3| Blood results | D1 | D3 | D4 | D5 | D6 | D7 | D8 | D9 | D10 | Reference ranges |
| White cells (× 109/L) | 11.8 | 11.8 | 8.7 | 7.8 | 9 | 6.7 | 7.2 | 8.8 | 9.7 | 4.0–11.0 |
| Neutrophils (× 109/L) | 8.5 | 8.8 | 6.6 | 4.8 | 5.3 | 3.9 | 3.4 | 4.3 | 5.4 | 2.0–7.5 |
| CRP (mg/L) | 18 | 263 | X | 479 | 440 | 287 | 137 | 170 | 216 | <5 |
| Sodium (mmol/L) | 139 | 127 | 125 | 126 | 125 | 127 | 133 | 133 | 132 | 135–145 |
| Potassium (mmol/L) | 3.3 | X | 4.6 | 4.4 | 4.3 | 3.7 | 3.4 | 4.2 | 4.4 | 3.6–5.0 |
| Blood test | Result | Reference range |
| ACTH (ng/L) | 273.1 | 7–63 ng/L |
| Cortisol (nmol/L) | 26 | 138–690 nmol/L |
| Renin (mmol/L) | 8.3 | 0.3–2.2 mmol/L |
| Aldosterone (pmol/L) | 61 | Up to 630 pmol/L |
| TSH (mU/L) | 2.2 | 0.4–4.0 (mU/L) |
| Testosterone (nmol/L) | 23.9 | 9.0–31 nmol/L |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAdrenal Hormones and Disorders · Viral gastroenteritis research and epidemiology · Vitamin K Research Studies
Introduction
Adrenal insufficiency is a condition in which the adrenal glands fail to produce adequate amounts of steroid hormones, primarily cortisol and aldosterone, leading to impaired stress response and electrolyte imbalances.
Primary adrenal insufficiency is most often caused by autoimmune destruction of the adrenal cortex. However, infectious aetiologies, including tuberculosis and bacterial sepsis, can also cause adrenal damage through haemorrhage or abscess formation. Salmonella infection, though typically self-limiting, may progress to bacteraemia and deep-seated abscesses in rare cases.
Non-typhoidal Salmonella, which includes the Saintpaul strain, is one of the most common sources of bacterial foodborne disease worldwide [1]. It has been documented that in Thailand, the most common serovars of Salmonella spp. isolated from humans were Salmonella Group B, including Salmonella Typhimurium, Salmonella Derby, Salmonella Anatum, and Salmonella Stanley. Salmonella Saintpaul was found in minced pork in the northern region of Thailand [2]. Dissemination of Salmonella to extraintestinal sites is uncommon, particularly in immunocompetent hosts. Here, we present a rare case of bilateral adrenal abscesses and adrenal insufficiency in an immunocompetent young adult due to disseminated *Salmonella *Saintpaul infection.
Case presentation
A 20-year-old previously healthy male presented to the emergency department with a one-day history of nausea, vomiting, severe abdominal pain, and profuse diarrhoea following recent travel to Thailand.
On initial assessment, he appeared clinically dehydrated, with dry mucous membranes, poor skin turgor, and sunken eyes. His vital signs revealed a temperature of 38°C, heart rate of 107 beats per minute, blood pressure of 100/70 mmHg, respiratory rate of 23 breaths per minute, and oxygen saturation of 98% on room air. Arterial blood gas analysis showed an elevated lactate level of 7 mmol/L (normal range 1-2 mmol/L). In view of a possible acute abdomen, the surgical team was initially involved. However, a computed tomography (CT) scan of the abdomen was unremarkable.
Notably, the patient tested positive for COVID-19 on admission, although his chest radiograph was normal. Given evidence of sepsis secondary to gastroenteritis in the context of COVID-19 infection, he was referred to the medical team and treated with empirical antibiotic therapy. Intravenous ceftriaxone (2 g once daily) and oral azithromycin (500 mg once daily) were initiated.
On day two of admission, despite appropriate antimicrobial coverage, the patient continued to have high-grade fevers (up to 39°C) and persistent tachycardia (heart rate approximately 160 beats per minute). Broad serological testing was performed to investigate a possible viral cause of fever, including HIV, Epstein-Barr virus (EBV), cytomegalovirus (CMV), malaria blood film, and hepatitis A and E serologies, all of which returned negative.
On day three, both blood and stool cultures returned positive for Salmonella species. Antimicrobial sensitivity testing revealed the isolate was sensitive to meropenem but resistant to ciprofloxacin, azithromycin, gentamicin, and piperacillin/tazobactam. Following microbiology consultation, the antibiotic regimen was escalated to intravenous meropenem (1 g every 8 hours) and vancomycin, with continuation of azithromycin (500 mg once daily). Despite escalation of treatment, the patient’s clinical status deteriorated further, with persistent tachycardia, recurrent pyrexia, ongoing gastrointestinal symptoms, and significantly raised inflammatory markers with C-reactive protein (CRP) of 400 mg/L (normal range <5 mg/L), along with electrolyte imbalances such as mild hyponatraemia and hypokalaemia (Table 1).
On day 7 after admission, an echocardiogram was performed to rule out infective endocarditis. Although it was negative for vegetations, it revealed severe global left ventricular systolic dysfunction and right ventricular impairment, consistent with tachycardia-induced cardiomyopathy. He was transferred to the coronary care unit (CCU) for close monitoring and telemetry, and initiation of full heart failure therapy.
In an attempt to identify the source of persistent fever and symptoms, a repeat CT of the abdomen and pelvis was performed on day 10 of admission to rule out perforation or deep-seated collection. This revealed new bilateral adrenal abscesses, more prominent on the right side (Figure 1). The case was discussed with the regional infectious disease and endocrinology teams. A random cortisol level was 26 nmol/L, and he was also experiencing recurrent episodes of hypoglycaemia, prompting the initiation of high-dose corticosteroids alongside ongoing broad-spectrum antibiotics.
Contrast-enhanced CT abdomen demonstrating right adrenal abscess (left red arrow) and left adrenal abscess (right red arrow)
The patient was referred to a specialist infectious diseases unit, where he was managed conservatively, as the abscesses were not accessible for drainage by interventional radiology. He was treated with intravenous antibiotics and corticosteroids following multidisciplinary team discussion. He subsequently improved and was discharged home after two more weeks of antibiotics and a repeat CT scan, which showed improvement of the adrenal abscesses and normalisation of inflammatory markers (Figure 2).
Contrast-enhanced CT (Day 38): Red arrow indicates reduced volume of right adrenal abscess; no evidence of recurrent left adrenal abscess
Two weeks later, he re-presented with recurrent symptoms of nausea, vomiting, and lethargy. He was restarted on antibiotics and corticosteroids. A repeat CT scan demonstrated interval improvement in the adrenal abscesses (Figure 3). During the second admission, endocrine evaluation showed an elevated ACTH level of 273.1 ng/L and a low cortisol level of 26 nmol/L, confirming primary adrenal insufficiency. Renin was elevated at 8.3 and aldosterone was low at 61 pmol/L, consistent with mineralocorticoid deficiency. He was symptomatic at that time, with dizziness upon standing and postural drop, so he was started on fludrocortisone 100 micrograms daily. Thyroid function tests, serum testosterone, and HbA1c were all within normal limits, with no evidence of autoimmune polyglandular syndrome (Table 2).
Contrast-enhanced CT (day 60): Further reduction in right adrenal abscess volume; left adrenal remains clear
Before discharge, he was educated on sick-day rules and steroid replacement protocols. A follow-up plan was established, including monitoring of cortisol levels and a scheduled short Synacthen test. At the four-week follow-up after discharge, the patient reported feeling well and stable, and was taking his steroid replacement therapy regularly. His cortisol levels remained low both before and after the Synacthen test, and he was advised to continue his maintenance dose. An annual review was arranged for repeat imaging and reassessment of adrenal function.
Discussion
This case highlights a rare but severe complication of *Salmonella *Saintpaul infection, leading to bilateral adrenal abscesses and adrenal insufficiency in an immunocompetent young adult. While *Salmonella *infections typically present as gastroenteritis, invasive forms can result in bacteraemia and abscess formation in various organs, including the adrenal glands [3-5]. *Salmonella *enteritidis is the most commonly reported serotype in clinical infections. In contrast, our case identified *Salmonella *Saintpaul through both blood and stool cultures, a serotype for which no prior infection outbreaks have been documented in Thailand. Notably, outbreaks of *Salmonella *Saintpaul have predominantly been reported in the United States and Brazil [6]. Our patient had recently travelled to Thailand, a region endemic for other *Salmonella *strains, suggesting a potentially under-recognised epidemiological presence or importation of this serotype. The initial symptoms of abdominal pain, vomiting, and diarrhoea were consistent with enterocolitis. However, persistent fever, elevated lactate of 4.5 mmol/L (normal range 0.6-2.4 mmol/L), and markedly raised C-reactive protein (CRP) of 457 mg/L (normal range <5 mg/L) suggested systemic involvement. Blood and stool cultures confirmed *Salmonella *Saintpaul, a rare serotype associated with travel-related outbreaks [7].
Persistent tachycardia led to tachycardia-induced cardiomyopathy, a reversible form of heart failure caused by sustained high heart rates. This condition is often underdiagnosed but can result in significant myocardial dysfunction. Studies show that early rate control and treatment of the underlying cause can lead to recovery of cardiac function [8-10].
Adrenal abscess formation is generally secondary to haematogenous dissemination from a distant infectious focus, with bilateral involvement more commonly observed in such cases. However, previously healthy individuals can also be affected, suggesting that certain *Salmonella *strains may have a predilection for adrenal tissue [3,4]. The adrenal glands’ unique vascular anatomy, with multiple arterial inputs but a single venous drainage, predisposes them to venous stasis ("damming"), haemorrhage, and microinfarction, providing a nidus for secondary bacterial infection [11].
*Salmonella *Saintpaul, a non-typhoidal serovar, can cause adrenal injury through systemic dissemination and immune-mediated mechanisms. During bacteraemia, the organism may seed adrenal tissue, where it hijacks programmed cell death pathways such as apoptosis, pyroptosis, necroptosis, and autophagy, resulting in cellular damage and inflammation [12]. Sepsis-induced adrenal insufficiency is a recognised phenomenon, often due to direct adrenal involvement or systemic inflammatory response impairing adrenal function. Studies indicate that relative adrenal insufficiency in sepsis is associated with poor outcomes, and early recognition is crucial for initiating corticosteroid therapy [13,14].
Individuals with any form of adrenal insufficiency are particularly vulnerable, as they cannot mount the normal cortisol surge needed during acute stressors. These stressors may include infection, especially sepsis, surgery, trauma, or significant emotional distress. Clinical presentation ranges from non-specific symptoms such as fatigue, nausea, and abdominal pain to progressive hypotension, hypoglycaemia, and electrolyte imbalance. Without prompt recognition and treatment, adrenal crisis can rapidly lead to circulatory collapse and death. In this case, recurrent hypoglycaemia and a critically low cortisol level (26 nmol/L) underscored the importance of early testing and therapeutic intervention with hydrocortisone replacement, which is lifesaving [15].
In terms of long-term management of hypoadrenalism, evidence from a systematic review suggests that nearly half (46.4%) of affected patients require sustained corticosteroid therapy, reflecting the risk of persistent adrenal insufficiency [16]. In this case, follow-up clinic assessment demonstrated consistently low serum cortisol levels, confirmed by a positive Synacthen test. Based on these findings, the patient was commenced on lifelong corticosteroid replacement therapy. This case underscores the importance of a multidisciplinary approach involving infectious disease specialists, endocrinologists, and the use of broad-spectrum antibiotics transitioning to targeted therapy as essential in controlling the infection. Additionally, patient education on steroid sick-day rules was crucial in preventing adrenal crisis following hospital discharge.
Learning points
Persistent fever despite initial broad-spectrum antibiotic therapy should prompt reassessment for rare infectious foci, such as deep-seated abscesses or endovascular involvement, underscoring the need to consider adrenal pathology in febrile patients with persistent systemic symptoms and unexplained metabolic derangements. Additionally, tachycardia-induced cardiomyopathy is recognised as a reversible complication of systemic stress and infection, further highlighting the complexity of such cases. Effective management requires multidisciplinary care and comprehensive patient education to address both infectious and endocrine sequelae. This case also contributes to the limited literature on Salmonella-induced adrenal abscesses.
Conclusions
This case illustrates a rare but clinically significant manifestation of *Salmonella *Saintpaul infection, culminating in bilateral adrenal abscesses and adrenal insufficiency in an immunocompetent individual. It underscores the importance of maintaining a high index of suspicion for extraintestinal complications in patients with persistent systemic symptoms following travel to endemic regions. Early recognition and multidisciplinary management, including targeted antimicrobial therapy, cardiac support, and hormone replacement, were pivotal to recovery. Clinicians should remain vigilant for adrenal involvement in systemic *Salmonella *infections, as timely intervention can be lifesaving and prevent long-term sequelae.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1The global burden and epidemiology of invasive non-typhoidal Salmonella infections Hum Vaccin Immunother Balasubramanian R Im J Lee JS 142114261520193008170810.1080/21645515.2018.1504717 PMC 6663144 · doi ↗ · pubmed ↗
- 2High-resolution melting-curve analysis for serotyping of Salmonella spp. group B isolated from minced pork in the Northern part of Thailand J Assoc Med Sci Poonchareon K Nuanmuang N Prommuang P Sriisan S 6372292018 https://he 01.tci-thaijo.org/index.php/bulletin AMS/article/view/136475
- 3Isolated adrenal abscess secondary to Salmonella Arch Surg O'Neill JA Jr Hall WH 4544569019651424742810.1001/archsurg.1965.01320090132029 · doi ↗ · pubmed ↗
- 4Non-typhi Salmonella adrenal abscess in an HIV-infected patient Scand J Infect Dis Kao PT Liu CP Lee CM Hung YC 3703723720051605157610.1080/00365540510034527 · doi ↗ · pubmed ↗
- 5Isolated splenic abscess due to Salmonella Berta in a healthy adult BMJ Case Rep Kobayashi T Bogdanic F Pujagic E Goto M 13202010.1136/bcr-2020-235318 PMC 716745032269050 · doi ↗ · pubmed ↗
- 6Worldwide population dynamics of Salmonella saintpaul: outbreaks, epidemiology, and genome structure Genes (Basel) Panzenhagen P Shah DH Rodrigues DD Conte Junior CA 16202510.3390/genes 16030254 PMC 1194237940149406 · doi ↗ · pubmed ↗
- 7Case report: post-salmonellosis abscess positive for Salmonella Oranienburg BMC Infect Dis Castlemain BM Castlemain BD 3372220223538276710.1186/s 12879-022-07217-5PMC 8981806 · doi ↗ · pubmed ↗
- 8Arrhythmia-induced cardiomyopathies: mechanisms, recognition, and management J Am Coll Cardiol Gopinathannair R Etheridge SP Marchlinski FE Spinale FG Lakkireddy D Olshansky B 171417286620152644914310.1016/j.jacc.2015.08.038PMC 4733572 · doi ↗ · pubmed ↗