Anatomical Burden of Prior Percutaneous Coronary Intervention and Long-Term Outcomes After Coronary Artery Bypass Grafting: An Analysis Spanning 2 Decades
Go Yamashita, Jiro Sakai, Takumi Takauchi, Shun Otani, Shoya Nakano, Ryo Fujimoto, Atsushi Sugaya, Shingo Hirao, Tatsuhiko Komiya

TL;DR
This study finds that multiple prior heart procedures increase risks after heart bypass surgery, with more complications and lower survival rates.
Contribution
The study introduces a novel analysis of how the number of prior heart procedures affects long-term outcomes after bypass surgery.
Findings
Multiple-lesion PCI was linked to higher risks of cardiac death, heart attack, and repeat procedures.
Single-lesion PCI had outcomes similar to no prior PCI except for increased heart failure hospitalizations.
Long-term survival was significantly lower in the multiple-lesion PCI group compared to others.
Abstract
This study aimed to determine whether the anatomical burden of prior percutaneous coronary intervention (PCI) influences long-term outcomes after coronary artery bypass grafting, beyond the impact of intervention presence alone. This retrospective study analysed consecutive patients undergoing coronary artery bypass grafting at a single institution between 2000 and 2024. The inclusion criteria comprised isolated, non-emergent surgery. Patient categorization was based on prior PCI-treated lesions: none, single, or multiple. The primary end-point was long-term overall survival. The secondary end-points included cardiac death, myocardial infarction, stroke, heart failure hospitalization, and repeat revascularization. Long-term outcomes were assessed using Kaplan-Meier analysis and Cox multivariable models, adjusting for 26 clinical factors. Of 2442 patients, 1205 met the inclusion…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
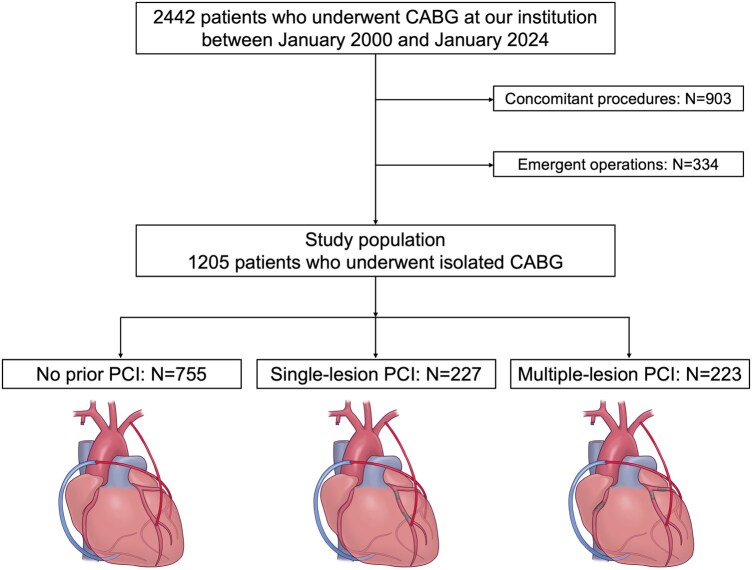 Figure 1
Figure 1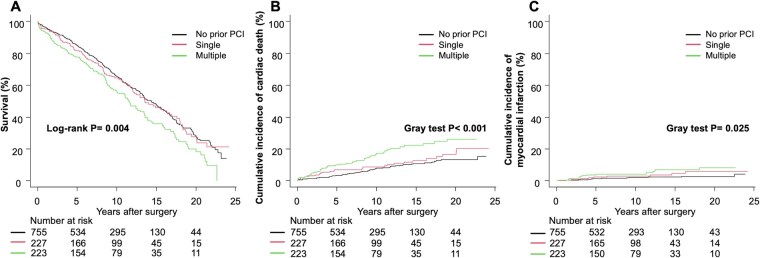 Figure 2
Figure 2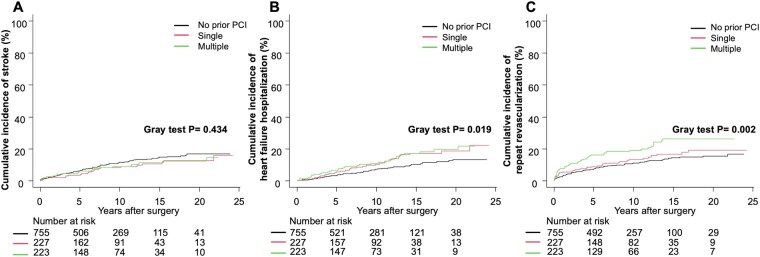 Figure 3
Figure 3| Characteristics | No PCI | Single-lesion PCI | Multiple-lesion PCI |
|
|
|---|---|---|---|---|---|
|
|
|
| |||
| Age, years, (SD) | 67.4 (10.8) | 66.7 (9.9) | 67.6 (8.9) | .615 | .307 |
| Age ≥ 75 | 192 (25.4) | 56 (24.7) | 49 (22.0) | .590 | .312 |
| Male | 595 (78.8) | 181 (79.7) | 176 (78.9) | .963 | .907 |
| BMI ≥ 25.0 kg/m² | 252 (33.4) | 80 (35.2) | 83 (37.2) | .546 | .272 |
| Hypertension | 589 (78.0) | 189 (83.3) | 195 (87.4) | .004 | <.001 |
| Hyperlipidaemia | 497 (65.8) | 146 (64.3) | 156 (70.0) | .404 | .362 |
| Current smoker | 120 (15.9) | 36 (15.9) | 20 (9.0) | .025 | .021 |
| Diabetes | 424 (56.2) | 129 (56.8) | 147 (65.9) | .031 | .017 |
| eGFR <45, without dialysis | 123 (16.3) | 46 (20.3) | 42 (18.8) | .313 | .241 |
| Dialysis | 60 (7.9) | 20 (8.8) | 43 (19.3) | <.001 | <.001 |
| Previous stroke | 122 (16.2) | 33 (14.5) | 45 (20.2) | .247 | .265 |
| Atrial fibrillation | 42 (5.6) | 10 (4.4) | 12 (5.4) | .838 | .775 |
| Old myocardial infarction | 223 (29.5) | 139 (61.2) | 130 (58.3) | <.001 | <.001 |
| Peripheral vascular disease | 134 (17.7) | 40 (17.6) | 45 (20.2) | .682 | .465 |
| Chronic obstructive pulmonary disease | 37 (4.9) | 9 (4.0) | 11 (4.9) | .832 | .885 |
| Anaemia (haemoglobin <11.0 g/dL) | 141 (18.7) | 53 (23.3) | 51 (22.9) | .179 | .098 |
| Thrombocytopaenia (platelets <100 × 109/L) | 21 (2.8) | 1 (0.4) | 2 (0.9) | .037 | .027 |
| LVEF ≤40% | 115 (15.2) | 36 (15.9) | 29 (13.0) | .651 | .502 |
| Bare metal stent | 0 | 158 (69.6) | 144 (64.6) | <.001 | <.001 |
| First-generation drug-eluting stent | 0 | 31 (13.7) | 80 (35.9) | <.001 | <.001 |
| Second-generation and newer drug-eluting stents | 0 | 43 (18.9) | 53 (23.8) | <.001 | <.001 |
| Drug-coated balloon | 0 | 3 (1.3) | 15 (6.7) | <.001 | <.001 |
| Characteristics | No PCI | Single-lesion PCI | Multiple-lesion PCI |
|
|
|---|---|---|---|---|---|
|
|
|
| |||
| Surgical characteristics | |||||
| Off-pump | 668 (88.5) | 196 (86.3) | 192 (86.1) | .515 | .276 |
| Number of anastomoses (SD) | 3.31 (0.96) | 3.31 (0.99) | 3.23 (0.85) | .496 | .313 |
| Internal thoracic artery use | 752 (99.6) | 222 (97.8) | 221 (99.1) | .031 | .167 |
| Target of chronic total occlusion | 288 (38.1) | 67 (29.5) | 62 (27.8) | .003 | .001 |
| Endarterectomy | 14 (1.9) | 8 (3.5) | 5 (2.2) | .329 | .469 |
| Total arterial revascularization | 255 (33.8) | 79 (34.8) | 66 (29.6) | .443 | .334 |
| Medication at discharge | |||||
| Antiplatelet therapy | 744 (98.5) | 222 (97.8) | 215 (96.4) | .131 | .046 |
| Dual antiplatelet therapy | 230 (30.5) | 78 (34.4) | 84 (37.7) | .106 | .034 |
| Aspirin | 721 (95.5) | 214 (94.3) | 198 (88.8) | .001 | <.001 |
| Clopidogrel | 163 (21.6) | 52 (22.9) | 67 (30.0) | .032 | .014 |
| Statins | 354 (46.9) | 100 (44.1) | 110 (49.3) | .532 | .713 |
| Beta-blockers | 323 (42.8) | 82 (36.1) | 94 (42.2) | .197 | .517 |
| ACE-I/ARB | 294 (38.9) | 102 (44.9) | 81 (36.3) | .147 | .857 |
| Outcome | No prior PCI | Single-lesion PCI | Multiple-lesion PCI |
|
|
|---|---|---|---|---|---|
| Re-exploration for bleeding | 15 (2.0) | 6 (2.6) | 10 (4.5) | .117 | .044 |
| IABP-support | 20 (2.6) | 6 (2.6) | 7 (3.1) | .921 | .724 |
| ECMO-support | 2 (0.3) | 2 (0.9) | 3 (1.3) | .141 | .048 |
| Gastrointestinal bleeding | 4 (0.5) | 1 (0.4) | 4 (1.8) | .131 | .090 |
| New-onset stroke | 16 (2.1) | 6 (2.6) | 9 (4.0) | .282 | .121 |
| New-onset dialysis | 6 (0.8) | 1 (0.4) | 1 (0.4) | .769 | .507 |
| Deep wound infection | 13 (1.7) | 5 (2.2) | 7 (3.1) | .422 | .195 |
| Prolonged ventilation | 50 (6.6) | 18 (7.9) | 25 (11.2) | .078 | .027 |
| Acute kidney injury | 183 (24.2) | 48 (21.1) | 76 (34.1) | .003 | .016 |
| In-hospital death | 11 (1.5) | 4 (1.8) | 6 (2.7) | .465 | .231 |
| Outcome | Group | Crude HR (95% CI) |
| Adjusted HR (95% CI) |
|
|---|---|---|---|---|---|
| Survival | No prior PCI | Reference | – | Reference | – |
| Single-lesion PCI | 1.05 (0.85-1.30) | .662 | 0.96 (0.76-1.21) | .719 | |
| Multiple-lesion PCI | 1.42 (1.15-1.74) | <.001 | 1.21 (0.97-1.52) | .096 | |
| Cardiac death | No prior PCI | Reference | – | Reference | – |
| Single-lesion PCI | 0.97 (0.62-1.52) | .900 | 1.15 (0.68-1.96) | .600 | |
| Multiple-lesion PCI | 2.16 (1.51-3.08) | <.001 | 1.91 (1.25-2.93) | .003 | |
| Myocardial infarction | No prior PCI | Reference | – | Reference | – |
| Single-lesion PCI | 1.26 (0.58-2.74) | .560 | 1.97 (0.79-4.90) | .140 | |
| Multiple-lesion PCI | 2.20 (1.14-4.23) | .019 | 2.26 (1.06-4.82) | .035 | |
| Stroke | No prior PCI | Reference | – | Reference | – |
| Single-lesion PCI | 0.70 (0.43-1.15) | .160 | 0.62 (0.37-1.04) | .069 | |
| Multiple-lesion PCI | 0.97 (0.64-1.48) | .900 | 0.86 (0.53-1.38) | .530 | |
| Heart failure hospitalization | No prior PCI | Reference | – | Reference | – |
| Single-lesion PCI | 1.55 (1.04-2.32) | .034 | 1.61 (1.01-2.56) | .042 | |
| Multiple-lesion PCI | 1.34 (0.90-2.00) | .140 | 1.54 (0.98-2.42) | .059 | |
| Repeat revascularization | No prior PCI | Reference | – | Reference | – |
| Single-lesion PCI | 1.07 (0.72-1.59) | .720 | 1.35 (0.88-2.07) | .170 | |
| Multiple-lesion PCI | 1.70 (1.23-2.36) | .001 | 1.92 (1.34-2.76) | <.001 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAcute Myocardial Infarction Research · Coronary Interventions and Diagnostics · Cardiac Imaging and Diagnostics
INTRODUCTION
Coronary artery bypass grafting (CABG) remains the standard treatment for complex coronary artery disease, particularly in patients with diabetes and high anatomical complexity.1^,^2 However, the approach to coronary revascularization has evolved considerably, with more patients now undergoing CABG after percutaneous coronary intervention (PCI). A contemporary analysis of the Society of Thoracic Surgeons Database revealed that the proportion of patients with prior PCI who subsequently underwent CABG increased from 20.0% in 2008 to 25.0% in 2018.3^,^4 The impact of prior PCI on CABG remains debatable.5–9 Meta-analyses have suggested that previous PCI may negatively impact early postoperative outcomes, including higher in-hospital and 30-day mortality.6–8 However, most studies have primarily examined the presence or frequency of prior PCI,9 potentially overlooking the anatomical complexity of PCI-treated lesions. This issue is particularly relevant as cardiac surgeons frequently encounter technical challenges when constructing bypass grafts in vessels with multiple stents, potentially affecting short- and long-term outcomes. However, the relationship between the number of PCI-treated lesions and subsequent CABG outcomes remains unclear. Despite established associations between prior PCI and CABG outcomes, the specific impact of anatomical PCI burden on long-term clinical events after CABG has not been systematically evaluated.
Therefore, we evaluated how the number of prior PCI-treated lesions, rather than the mere presence or frequency of PCI, influences long-term clinical outcomes following CABG. To investigate this relationship, we analysed over 2 decades of consecutive CABG procedures performed at a single institution.
PATIENTS AND METHODS
Ethical statement
This retrospective, observational, single-centre study was approved by the Institutional Review Board of Kurashiki Central Hospital (Approval No. 4456; Approval Date: August 6, 2024). The requirement for informed consent was waived due to the retrospective nature of the study. Any collection and storage of data or biological material from research participants for multiple and indefinite use was conducted in accordance with the WMA Declaration of Taipei. The research ethics committee approved the establishment and ongoing use of such databases and biobanks.
Study design and population
We retrospectively analysed data from consecutive adult patients (aged ≥ 18 years) who underwent CABG at our institution between January 2000 and January 2024 (n = 2442). The exclusion criteria were: (1) concomitant cardiac procedures, including valve surgery or aortic procedures; (2) emergent operations requiring immediate surgical intervention. No patients were excluded based on sex, comorbidities, or the number of bypass grafts. After applying these criteria, only patients who underwent isolated CABG were included in the final analysis.
Definition of prior PCI lesions and patient classification
The coronary artery system was divided into 3 main regions: left anterior descending artery (LAD), left circumflex artery (LCx), and right coronary artery (RCA). Patients were categorized into 3 groups based on the location of prior PCI-treated lesions: no prior PCI (patients with no history of PCI), single-lesion PCI (patients with PCI in 1 coronary region), and multiple-lesion PCI (PCI in 2 or more regions). Prior stent implantation in the left main trunk was considered as 2-region involvement and classified into the multiple-lesion PCI group. The frequency of PCI procedures did not influence group classification. For instance, patients who underwent multiple PCIs in the same region (eg, 2 procedures in the LAD) were classified into the single-lesion PCI group.
Definitions for baseline characteristics and outcome measures
The primary end-point was long-term overall survival (OS). The secondary end-points included cardiac death, myocardial infarction (MI),10 stroke, heart failure hospitalization, and repeat revascularization. Detailed definitions of all baseline characteristics and outcome measures are provided (see Supplementary Method). In-hospital outcomes, including acute kidney injury (AKI) (assessed using established criteria11), bleeding complications, mechanical support requirements, and mortality, were comprehensively evaluated to assess perioperative safety across groups. Patient characteristics and operative data were obtained from medical records. Follow-up data were collected through outpatient clinic chart reviews, telephone interviews, and postal questionnaires for patients who did not attend the outpatient clinic. Data collection was completed on March 31, 2024. Given our annual follow-up protocol, patients who had clinic visits or were contacted within 12 months of this date were considered to have complete follow-up. Follow-up completeness was assessed using the percentage method, calculated as the proportion of patients with known vital status within 12 months of study end divided by the total number of enrolled patients.
Surgical procedures
The surgical technique has been previously described.9 In the early 2000s, while the internal thoracic artery remained the primary conduit, the right gastroepiploic artery (RGEA) and radial artery (RA) were frequently incorporated as additional arterial conduits to facilitate an aorta-no-touch technique. The introduction of a harmonic scalpel (Ethicon Endo-Surgery Inc.) significantly improved internal thoracic artery harvesting,12 leading to increased adoption of bilateral internal thoracic artery grafting. Recently, there has been a shift towards incorporating no-touch saphenous vein grafts (NT-SVG) into our revascularization strategy13 (see Figure S1).
Statistical analysis
Continuous variables are presented as mean (standard deviation) or median (interquartile range [IQR]) depending on normality, as assessed by Shapiro-Wilk test. Variables among groups were compared using 1-way analysis of variance or Kruskal-Wallis test, as appropriate.
Categorical variables are presented as counts and percentages and were compared using chi-square test or Fisher’s exact test. When significant group differences were found, post hoc pairwise comparisons used Fisher’s exact test with Holm’s correction. Trend analyses were performed to assess dose-response relationships across PCI burden categories. Cochrane-Armitage trend tests were used for binary outcomes and Jonckheere-Terpstra tests for continuous outcomes. Median follow-up time was calculated using the reverse Kaplan-Meier method. Long-term clinical outcomes, including OS, were estimated using Kaplan-Meier analysis. Differences were assessed by the log-rank test. For cardiac death, the cumulative incidence function was estimated with non-cardiac death as a competing risk. For other postoperative outcomes (MI, stroke, heart failure hospitalization, and repeat revascularization), cumulative incidence functions were estimated considering death as a competing risk. Differences between groups were compared using Gray’s test. The effects of multiple-lesion and single-lesion PCI, relative to no prior PCI, were estimated using Cox proportional hazards models for OS and Fine-Gray competing risk models for cause-specific outcomes. Adjusted hazard ratios (HRs) with 95% confidence intervals (CIs) and subdistribution HRs (sHRs) with 95% CIs were calculated using multivariable models incorporating 26 clinically relevant covariates (Tables 1 and 2), selected based on clinical importance, prior prognostic evidence,14 and baseline differences (P < .05). Missing data were assessed for all variables. Complete case analysis was performed for the multivariable models, as missing data were <1% for all baseline covariates. No imputation was performed, given the minimal missing data and assumption of missing completely at random mechanism. Patients were censored at death, last known contact, or March 31, 2024, whichever occurred first. All statistical analyses were performed using R software version 4.4.1 (The R Foundation for Statistical Computing, Vienna, Austria), with significance set at 2-sided P < .05.
RESULTS
Baseline characteristics
The final study cohort comprised 1205 patients who underwent isolated CABG, stratified into 3 groups: no prior PCI (n = 755), single-lesion PCI (n = 227), and multiple-lesion PCI (n = 223) (Figure 1). From 2000 to 2024, the annual proportion of patients with prior PCI ranged from 17.6% to 52.2% (Figure S2). The prevalence of hypertension, eGFR, dialysis, and prior MI differed among groups, with prior MI being markedly higher in patients with previous PCI (no PCI: 29.5%, single-lesion: 61.2%, multiple-lesion: 58.3%; P < .001), suggesting more extensive coronary disease in these patients. However, left ventricular function was similar across groups, with comparable left ventricular ejection fraction (LVEF) rates ≤40% (15.2%, 15.9%, and 13.0%, for no prior PCI, single-lesion PCI, and multiple-lesion PCI, respectively; P = .651). Bare metal stents (BMS) were most commonly implanted (25.1%), followed by first-generation drug-eluting stents (9.2%). Off-pump CABG was performed in 87.6% of cases. The number of arterial grafts, targets of chronic total occlusion, and intraoperative blood transfusion varied. Most patients were prescribed antiplatelet therapy, with aspirin being the most common (94.0%), while clopidogrel use varied among groups. Significantly increasing trends for hypertension (P < .001), diabetes (P = .017), and dialysis (P < .001) were noted across PCI burden categories (Tables 1 and 2 and Table S1).
Flow Diagram Illustrating Patient Selection and Study Groups Classification. Abbreviations: CABG: coronary artery bypass grafting; PCI: percutaneous coronary intervention
In-hospital clinical outcomes
The incidence of AKI differed significantly across groups (no prior PCI, 24.2%; single-lesion PCI, 21.1%; multiple-lesion PCI, 34.1%; P = .003, P for trend = .016). Holm’s post hoc test showed that the multiple-lesion PCI group had a higher incidence than both the single-lesion PCI (P = .007) and no prior PCI groups (P = .009), while no significant difference was found between the no prior PCI and single-lesion PCI groups (P = .373). In-hospital mortality was similar across all groups (P = .465). Other complications—re-exploration for bleeding, mechanical circulatory support, gastrointestinal bleeding, new-onset stroke, dialysis, deep wound infection, and prolonged ventilation—did not differ significantly (Table 3). The distribution of stented territories differed between groups (Table S2). In the single-lesion PCI group, RCA was most frequently stented (62.1%), while the multiple-lesion PCI group showed high rates of stenting across all territories, with particularly high LAD involvement (85.7%). Early graft patency rates are shown in Table S3.
Long-term clinical outcomes
The complete follow-up rate calculated per the percentage method was 92.4%. The median follow-up time for the entire cohort, calculated using the reverse Kaplan-Meier method, was 12.0 years (IQR: 11.3-12.9), with a maximum of 24.2 years. Median follow-up times were 11.3 years (10.6-12.5), 14.0 years (11.3-15.8), and 12.1 years (10.9-15.5) for the no prior PCI, single-lesion, and multiple-lesion PCI groups, respectively. Analysis of long-term outcomes revealed several key findings. OS differed significantly across groups over the entire follow-up period (log-rank P = .004; Figure 2A). At 15 years, the observed survival rates were 35.8%, 46.0%, and 48.0% for the multiple-lesion, single-lesion, and no prior PCI groups, respectively. For OS, analysed using Cox proportional hazards models, the risk of all-cause death in the multiple-lesion PCI group was numerically higher but not statistically significant (adjusted HR: 1.21; 95% CI: 0.97-1.52; P = .096). Competing risk analyses showed significant differences between groups for cardiac death (Gray’s test, P < .001; Figure 2B) and repeat revascularization (Gray’s test, P = .002; Figure 3C), with borderline significance for MI (Gray’s test, P = .025; Figure 2C) and heart failure hospitalization (Gray’s test, P = .019; Figure 3B). Stroke outcomes did not differ significantly (Gray’s test, P = .434; Figure 3A). After adjusting for confounders using Fine-Gray competing risk models (Table 4), the multiple-lesion PCI group showed higher risks of cardiac death (adjusted sHR: 1.91; 95% CI: 1.25-2.93; P = .003), MI (adjusted sHR: 2.26; 95% CI: 1.06-4.82; P = .035), and repeat revascularization (adjusted sHR: 1.92; 95% CI: 1.34-2.76; P < .001) compared with the no prior PCI group. For heart failure hospitalization, the multiple-lesion PCI group showed a trend towards increased risk (adjusted sHR: 1.54; 95% CI: 0.98-2.42; P = .059), while the single-lesion PCI group had significantly higher risk (adjusted sHR: 1.61; 95% CI: 1.01-2.56; P = .042). For stroke, no significant differences were observed among the 3 groups (adjusted sHR for multiple-lesion: 0.86; 95% CI: 0.53-1.38; P = .530).
Clinical Outcomes According to Prior PCI Status. (A) Kaplan-Meier curves for overall survival. (B) Cumulative incidence curves for cardiac death with non-cardiac death as a competing risk. (C) Cumulative incidence curves for myocardial infarction with all-cause death as a competing risk. Abbreviation: PCI: percutaneous coronary intervention
Clinical Outcomes According to Prior PCI Status (Continued). (A) Cumulative incidence curves for stroke with all-cause death as a competing risk. (B) Cumulative incidence curves for heart failure hospitalization with all-cause death as a competing risk. (C) Cumulative incidence curves for repeat revascularization with all-cause death as a competing risk. Abbreviation: PCI: percutaneous coronary intervention
During follow-up, 36 patients experienced MI (detailed angiographic findings are provided in Table S4).
DISCUSSION
The present study highlights several key findings regarding the impact of prior PCI treatment on subsequent CABG outcomes. First, patients who underwent multiple-lesion PCI had significantly higher rates of AKI during the immediate postoperative period than those with no prior PCI or single-lesion PCI. Second, multiple-lesion PCI was associated with worse long-term outcomes, including increased risk of cardiac death, MI, and repeat revascularization. Third, patients who underwent single-lesion PCI showed outcomes comparable to those without prior PCI for most end-points, except for heart failure hospitalization. These findings build upon previous studies that primarily focused on the presence or frequency of prior PCI procedures. While meta-analyses have suggested adverse effects of prior PCI on short-term outcomes after CABG,6–8 our study demonstrates that the anatomical burden of PCI-treated lesions, rather than the mere presence of prior PCI, may be a more relevant predictor of long-term outcomes. The higher incidence of postoperative AKI in the multiple-lesion PCI group warrants further investigation. This finding may be attributed to cumulative contrast exposure and higher prevalence of baseline renal dysfunction in this group. These observations underscore the need for meticulous perioperative renal management in patients with extensive PCI history.
Post-CABG MI analysis revealed 41.7% occurred in previously stented lesions with failed grafts, highlighting revascularization challenges. Technical difficulties include altered vessel architecture,15 compromised distal runoff,6 and limited anastomotic sites.5^,^9 The generally comparable outcomes between the single-lesion PCI and no prior PCI groups (except for heart failure hospitalization) suggest that limited PCI exposure may not significantly compromise surgical revascularization in most aspects, provided that appropriate patient selection and techniques are used. This has important implications for the “heart team” approach to revascularization, indicating that initial PCI of a single lesion may be reasonable for selected patients who may eventually undergo CABG.14
The extent of epicardial coronary artery disease has been identified as a strong predictor of perioperative MI following CABG.16 In our study, patients with multiple-lesion PCI likely had more extensive and diffuse coronary disease, which may have contributed to their higher perioperative complication rates and worse long-term outcomes. Although we did not systematically measure perioperative MI, the elevated incidence of AKI in the multiple-lesion PCI group may reflect their overall higher perioperative risk profile, as major perioperative complications often cluster in high-risk patients.
Our findings have significant implications for clinical revascularization strategies. The number of PCI-treated lesions has emerged as a crucial factor in risk assessment for subsequent CABG, beyond the traditional consideration of prior PCI. Patients with a multiple-lesion PCI require tailored perioperative strategies, particularly renal function monitoring, given their higher risk of AKI. Additionally, the technical challenges observed, especially the high rate of graft failure in previously stented vessels, underscore the importance of careful conduit selection and precise anastomotic site placement. The increased risk of adverse cardiac events in these patients highlights the need for a more rigorous post-CABG surveillance.
These observations also carry broader implications for the heart team’s decision-making. When determining initial treatment strategies for complex coronary artery disease, the potential impact of extensive stenting on future surgical options should be carefully weighed. This is particularly relevant given our finding that single-lesion PCI did not significantly compromise surgical outcomes, suggesting that limited PCI remains a viable option for patients who may eventually require CABG. This knowledge should inform revascularization planning, especially for younger patients with longer life expectancy. Additionally, our study reflects the historical context of coronary intervention, where BMS predominated over DES. However, the evolving stent landscape limits our ability to draw firm conclusions regarding newer-generation DES. Further studies are needed to evaluate the impact of current-generation stents on subsequent CABG outcomes.
This study has limitations. First, as a retrospective, single-centre study, its findings may have limited generalizability. Second, although multivariate adjustments were performed, unmeasured confounders may have influenced the results. Third, our definition of PCI burden based on the number of treated territories does not capture other important aspects, such as the total stent length or number of stents per vessel, which were not available in our database. These metrics might provide additional insights into the relationship between PCI complexity and CABG outcomes. Fourth, standardized risk scores, such as EuroSCORE or STS score, were not available due to the extended study period and evolving score algorithms. However, our multivariable models incorporated 26 clinical variables that encompass most risk factors included in these standardized scores. Finally, we did not collect data on post-infarction left ventricular aneurysm, which could influence surgical outcomes, particularly given the higher prevalence of prior MI in the PCI groups. While we adjusted for overall left ventricular function (LVEF ≤40%), this does not capture the specific impact of ventricular aneurysm.
CONCLUSION
Over 2 decades, multiple-lesion PCI was associated with higher risks of cardiac death, MI, and repeat revascularization after CABG, while stroke did not differ materially among groups. Single-lesion PCI yielded outcomes broadly comparable to no prior PCI, aside from a higher risk of heart failure hospitalization; in contrast, multiple-lesion PCI showed only a trend towards increased heart failure hospitalization. Although our multivariable models adjusted for 26 covariates, unmeasured confounding remains possible. Accordingly, the anatomical extent of prior PCI should be considered in revascularization planning for surgical candidates, and confirmation in larger, multicentre cohorts with granular PCI metrics and prospective comparative designs is warranted before drawing definitive conclusions.
Supplementary Material
ivaf237_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sousa-Uva M , Neumann F-J, Ahlsson A, et al; ESC Scientific Document Group. 2018 ESC/EACTS guidelines on myocardial revascularization. Eur J Cardiothorac Surg. 2019;55:4-90.30165632 10.1093/ejcts/ezy 289 · doi ↗ · pubmed ↗
- 2Virani SS, Newby LK, Arnold SV, et al. 2023 AHA/ACC/ACCP/ASPC/NLA/PCNA guideline for the management of Patients With Chronic Coronary Disease: A report of the American heart association/American college of cardiology joint committee on clinical practice guidelines. Circulation. 2023;148:e 9-e 119. 10.1161/CIR.000000000000116837471501 · doi ↗ · pubmed ↗
- 3Shahian DM , O’Brien SM, Filardo G, et al; Society of Thoracic Surgeons Quality Measurement Task Force. The Society of Thoracic Surgeons 2008 cardiac surgery risk models: part 1—coronary artery bypass grafting surgery. Ann Thorac Surg. 2009;88:S 2-S 22.19559822 10.1016/j.athoracsur.2009.05.053 · doi ↗ · pubmed ↗
- 4O’Brien SM , Feng L, He X, et al Adult cardiac surgery risk models: part 2-statistical methods and results. Ann Thorac Surg. 2018;105:1419-1428.29577924 10.1016/j.athoracsur.2018.03.003 · doi ↗ · pubmed ↗
- 5Ueki C , Miyata H, Motomura N, et al Previous percutaneous coronary intervention does not increase adverse events after coronary artery bypass surgery. Ann Thorac Surg. 2017;104:56-61.28131427 10.1016/j.athoracsur.2016.10.028 · doi ↗ · pubmed ↗
- 6Ueki C , Sakaguchi G, Akimoto T, et al Influence of previous percutaneous coronary intervention on clinical outcome of coronary artery bypass grafting: a meta-analysis of comparative studies†. Interact Cardio Vasc Thorac Surg. 2015;20:531-537; discussion 537.25583647 10.1093/icvts/ivu 449 · doi ↗ · pubmed ↗
- 7Altarabsheh SE , Deo SV, Hang D, et al Coronary artery bypass grafting after percutaneous intervention has higher early mortality: a meta-analysis. Ann Thorac Surg. 2015;99:2046-2052.25865763 10.1016/j.athoracsur.2014.12.073 · doi ↗ · pubmed ↗
- 8Zhang H , Zhao Z, Yao J, et al Prior percutaneous coronary intervention and outcomes in patients after coronary artery bypass grafting: a meta-analysis of 308,284 patients. Ther Adv Chronic Dis. 2022;13:20406223221078755.35586304 10.1177/20406223221078755 PMC 9109498 · doi ↗ · pubmed ↗