Anaplastic Lymphoma Kinase (ALK) Fusion as a Resistance Mechanism to Epidermal Growth Factor Receptor (EGFR) Tyrosine Kinase Inhibitors With Complete Response After Osimertinib and Alectinib: A Case Report and Literature Review
Ben Man Fei Cheung, Aya El Helali, Dennis Kwok Chuen Leung

TL;DR
A rare resistance mechanism to EGFR inhibitors in lung cancer involves ALK fusion, which can be effectively treated with a combination of targeted therapies.
Contribution
This case report and literature review highlight ALK fusion as a treatable resistance mechanism to EGFR TKIs in NSCLC.
Findings
ALK fusion was identified in 16 cases as a resistance mechanism to EGFR TKIs, with EML4::ALK being the most common variant.
Combination therapy with EGFR and ALK TKIs showed a 66.7% objective response rate with good tolerability.
CNS involvement was common in these cases, and molecular profiling at progression is essential for identifying this resistance mechanism.
Abstract
Acquired resistance to epidermal growth factor receptor (EGFR) tyrosine kinase inhibitors (TKIs) remains a significant challenge in the management of EGFR-mutant non-small-cell lung cancer (NSCLC). While EGFR T790M mutation and MET amplification are well-established resistance mechanisms, the development of secondary oncogenic fusions such as anaplastic lymphoma kinase (ALK) rearrangements is rare but clinically actionable. We report a 62-year-old male with EGFR exon 19 deletion-positive NSCLC who initially responded to osimertinib but developed progressive brain metastasis after 13 months of treatment. Next-generation sequencing of the brain metastasis revealed an acquired EML4::ALK fusion while maintaining the original EGFR exon 19 deletion. The patient was treated with a combination of osimertinib and alectinib, achieving a complete response that has been sustained for 12 months…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
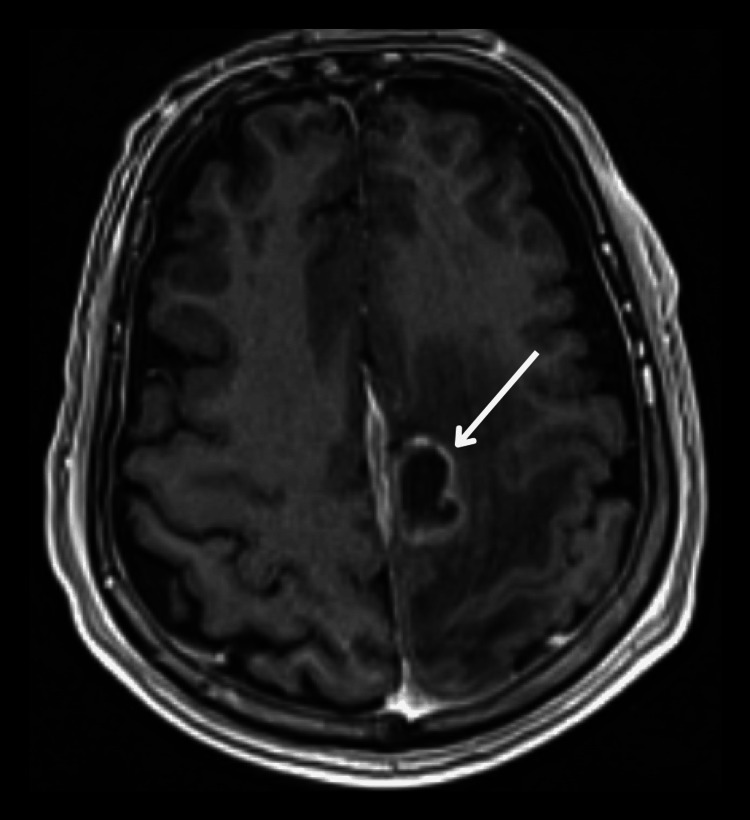 Figure 1
Figure 1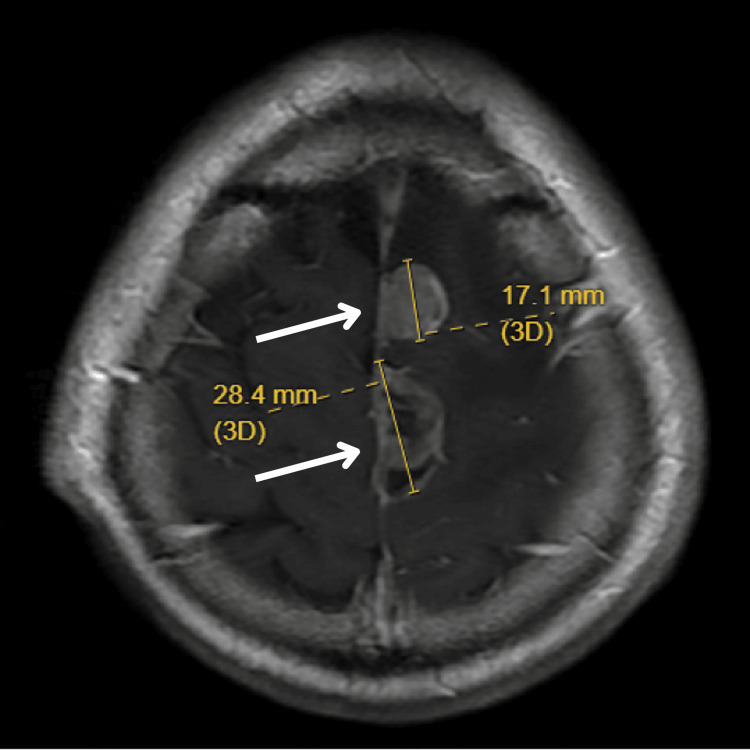 Figure 2
Figure 2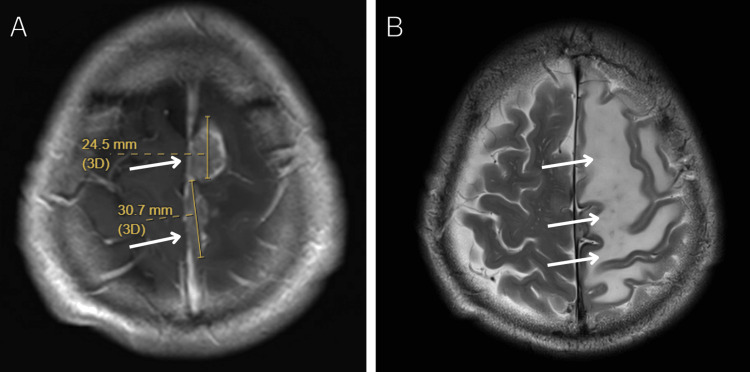 Figure 3
Figure 3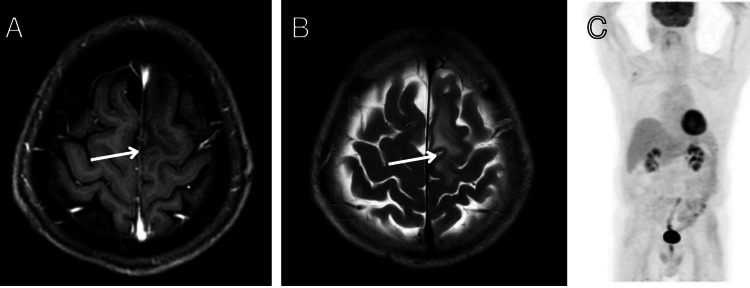 Figure 4
Figure 4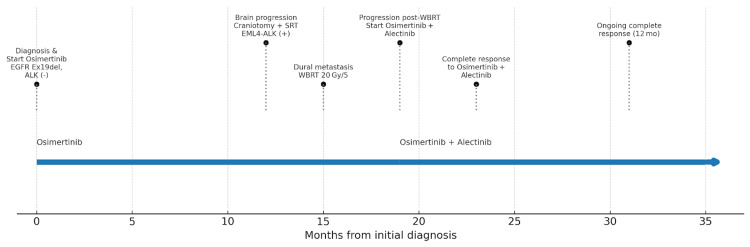 Figure 5
Figure 5| Case | First author (year) | Age/sex | EGFR mutation | EGFR-TKI history | ALK fusion | Interval to ALK resistance (months) | Post-resistance regimen | Best response | Grade ≥3 adverse events | Biopsy site | Testing | CNS progression | Extracranial progression site(s) |
| 1 | Present case | 65/M | Exon 19 del | Osimertinib | EML4-ALK | 13 | Osimertinib + alectinib | CR | None | Brain | IHC + NGS | Yes | No |
| 2 | Schrock et al. (2018), Case 7 [ | 63/F | Exon 19 deletion | Erlotinib → osimertinib | EML4-ALK | 16 | N/A | - | N/A | N/A | N/A | N/A | N/A |
| 3 | Schrock et al. (2018), Case 9 [ | 46/F | L747P | Afatinib | EML4-ALK | 21 | N/A | N/A | N/A | N/A | N/A | N/A | N/A |
| 4 | Schrock et al. (2018), Case 10 [ | 67/F | L858R → T790M | Erlotinib → afatinib → osimertinib | PLEKHA7-ALK | 29 | Osimertinib + alectinib | PR | N/A | Liquid | NGS | N/A | N/A |
| 5 | Schrock et al. (2018), Case 11 [ | 61/M | L858R | Erlotinib → afatinib | EML4-ALK | 7.5 | N/A | N/A | N/A | N/A | N/A | N/A | N/A |
| 6 | Schrock et al. (2018), Case 26 [ | 68/M | Exon 19 deletion | Erlotinib → osimertinib | STRN-ALK | N/A | No | N/A | N/A | N/A | N/A | N/A | N/A |
| 7 | Schrock et al. (2018), Case 27 [ | 62/M | Exon 19 deletion | Afatinib | EML4-ALK | N/A | No | N/A | N/A | Liquid | NGS | N/A | N/A |
| 8 | Schrock et al. (2018), Case 28 [ | 60/F | L858R | Osimertinib | TFG-ALK | N/A | No | N/A | N/A | Liquid | NGS | N/A | N/A |
| 9 | Liang et al. (2016) [ | 46/F | Exon 19 deletion | Erlotinib → chemotherapy + bevacizumab → osimertinib | EML4-ALK | 6 | Osimertinib + crizotinib → osimertinib + brigatinib | PR | None | Liquid | NGS | No | Liver |
| 10 | Offin et al. (2018), Case 1 [ | 57/F | Exon 19 deletion → T790M | Erlotinib → osimertinib + necitumumab | EML4-ALK | 23 | Osimertinib + crizotinib | PR | None | Lung | IHC + NGS | No | Lung |
| 11 | Offin et al. (2018), Case 2 [ | 65/F | Exon 19 deletion → T790M | Erlotinib → osimertinib | EML4-ALK | 21 | Osimertinib + alectinib | PR | None | Lung | IHC + NGS | No | Lung |
| 12 | Zeng et al. (2021) [ | 59/M | L858R → T790M | Gefitinib | EML4-ALK, STRN-ALK | 10 | Osimertinib + crizotinib | SD | None | N/A | N/A | No | Liver & bone |
| 13 | Hou et al. (2021) [ | 60/F | Exon 19 deletion | Gefitinib → osimertinib | EML4-ALK | 32 | Osimertinib + crizotinib → brigatinib → osimertinib + crizotinib → chemotherapy + bevacizumab + osimertinib + dasatinib → osimertinib + EGFR antibody → chemotherapy → osimertinib + alectinib | SD | Brigatinib-induced ILD | Lung | NGS | No | Lung |
| 14 | von Buttlar et al. (2021) [ | 78/F | Exon 19 deletion | Osimertinib | EML4-ALK | 34 | Osimertinib + alectinib | PR | None | Lung | NGS | Yes | Lung |
| 15 | Yin et al. (2022) [ | 60/F | Exon 19 deletion + T790M (de novo) | Osimertinib | DCTN1-ALK | 16 | Alectinib | PR | None | Liquid | NGS | Yes | Lung, pleural effusion |
| 16 | Portugal et al. (2023) [ | 42/F | L858R | Osimertinib | EML4-ALK | 10 | Osimertinib + alectinib | SD | None | Lung | NGS | No | Lung, adrenal |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLung Cancer Treatments and Mutations · Lung Cancer Research Studies · Cancer therapeutics and mechanisms
Introduction
The emergence of acquired resistance remains a major challenge in the management of epidermal growth factor receptor (EGFR)-mutant non-small-cell lung cancer (NSCLC) treated with tyrosine kinase inhibitors (TKIs). While EGFR T790M and MET amplification are well-established resistance mechanisms, the development of secondary oncogenic fusions, such as anaplastic lymphoma kinase (ALK) rearrangements, is rare but clinically actionable [1].
EGFR-mutant NSCLC represents approximately 10-15% of lung adenocarcinomas in Western populations and up to 50% in East Asian populations [2]. Despite significant advances with third-generation EGFR TKIs like osimertinib, which has demonstrated superior efficacy with a median progression-free survival of 18.9 months in first-line treatment [3], acquired resistance remains inevitable. Secondary ALK fusions occur in approximately 1-3% of patients with acquired resistance to EGFR TKIs [4]. Unlike other resistance mechanisms that may require chemotherapy, ALK fusions represent actionable targets that can be effectively treated with approved ALK inhibitors [5]. However, the optimal management strategy for patients with concurrent EGFR mutations and secondary ALK fusions remains unclear, particularly regarding combination targeted therapy approaches [6].
This case report describes a patient with EGFR-mutated NSCLC who developed an acquired EML4::ALK fusion after progression on osimertinib, and achieved a durable complete response with combination osimertinib and alectinib. Existing literature was also reviewed to shed light on this rare but important resistance mechanism.
Case presentation
A 62-year-old male initially presented with weakness and clumsiness. He had a performance status of 0 on presentation. MRI brain revealed a 2.5 cm high frontal contrast-enhancing lesion along the midline, suspicious of brain metastasis. Whole body PET-CT showed a 2.6 cm lung mass over the left lower lobe as well as iliac bone metastasis. Biopsy of the left lower lobe lung mass revealed adenocarcinoma of lung origin. Next-generation sequencing (NGS; Oncomine Precision Assay, Ion Torrent Genexus System, Thermo Fisher Scientific, Waltham, MA) of the tumor demonstrated EGFR exon 19 deletion mutation. ALK was negative by both NGS and immunohistochemistry (IHC) at the time. No other mutations were present.
The patient was started on osimertinib (80 mg daily) with a good response. Interval PET-CT and MRI brain demonstrated partial response to osimertinib, with resolution of neurological symptoms. The disease remained under control for one year. At this time, the patient developed new-onset right upper limb weakness and clumsiness. MRI brain demonstrated a solitary 2 cm lesion over the left frontal lobe (Figure 1). PET-CT showed sustained complete response for extracranial disease. Craniotomy with excision of brain metastasis was done. NGS (Oncomine Precision Assay, Ion Torrent Genexus System, Thermo Fisher Scientific) of the brain metastasis was done, which was positive for EGFR exon 19 deletion as well as ALK fusion rearrangement. The specific ALK fusion was EML4::ALK. Orthogonal testing showed that ALK was positive by IHC as well. The EGFR T790M mutation was negative. Postoperative stereotactic radiotherapy was delivered to the surgical cavity at 32.5 Gy over five fractions. In view of the complete resection of all progressive lesions, the patient was continued on osimertinib.
Initial presentation and early progression on osimertinib.Axial T1-weighted contrast-enhanced MRI brain image showing a solitary 2 cm enhancing lesion in the left frontal lobe at the time of disease progression on osimertinib. This lesion was surgically resected and found to harbor both EGFR exon 19 deletion and acquired EML4::ALK fusion.EGFR: epidermal growth factor receptor; ALK: anaplastic lymphoma kinase.
However, the patient developed status epilepticus three months later. MRI brain showed a new parasagittal dural metastasis (Figure 2). The patient was treated with palliative whole brain radiotherapy (WBRT) at 20 Gy in five fractions.
Disease progression on surgical resection and radiotherapy.Axial T1-weighted contrast-enhanced MRI brain image demonstrating new parasagittal dural metastasis, occurring three months after surgical resection and stereotactic radiotherapy. The patient developed status epilepticus at this time and was treated with palliative whole-brain radiotherapy.
The patient was continued on osimertinib (80 mg daily) and interval MRI brain four months after WBRT demonstrated progressive parasagittal lesion while extracranial disease was still in remission (Figure 3).
Disease progression on osimertinib monotherapy.(A) Axial T1-weighted contrast-enhanced MRI brain image showing progressive parasagittal lesion after whole-brain radiotherapy while on continued osimertinib monotherapy. Measurements indicate tumor dimensions of 24.5 mm and 30.7 mm. (B) Axial T2-weighted MRI brain image showing significant perilesional edema, demonstrating continued disease progression despite osimertinib treatment.
ALK fusion was hence deemed to be the resistance mechanism to osimertinib. The patient was started on a combination of osimertinib (80 mg daily) and alectinib (600 mg twice daily). Four months after starting combination EGFR and ALK inhibitor, interval MRI brain demonstrated complete response of dural metastasis with resolution of all neurological symptoms (Figures 4A, 4B). The patient is on osimertinib with alectinib to date, with a complete response for one year (Figure 4C). The patient had regular follow-ups every month for safety monitoring. The patient did not experience any significant toxicity from treatment.
Complete response to combination therapy.(A) Axial T1-weighted contrast-enhanced MRI brain image demonstrating complete response of the dural metastasis four months after initiation of combination osimertinib and alectinib therapy. (B) Axial T2-weighted MRI brain image demonstrating near complete resolution of edema four months after initiation of combination osimertinib and alectinib therapy. (C) Whole body PET-CT demonstrating complete extracranial response four months after initiation of combination osimertinib and alectinib therapy, showing no evidence of metabolically active disease.
The timeline of treatment is presented in Figure 5.
Treatment timeline.Timeline illustrating the patient's treatment course from initial diagnosis through combination targeted therapy. The timeline shows initial presentation with brain and extracranial metastases, response to osimertinib, development of brain-specific progression with acquired ALK fusion, and subsequent complete response to combination osimertinib and alectinib therapy. Key molecular findings and treatment interventions are highlighted at relevant time points.EGFR: epidermal growth factor receptor; ALK: anaplastic lymphoma kinase; SRT: stereotactic radiotherapy; WBRT: whole brain radiotherapy.
Discussion
Resistance mechanism to EGFR inhibitors is heterogeneous [7]. The most commonly described mechanism of resistance to EGFR inhibitors was the T790M mutation [1]. Other documented mutations included the EGFR C797X mutation, MET amplification, and HER2 amplification [8]. Emergence of oncogenic fusion as a resistance mechanism to EGFR TKIs is a rare but documented phenomenon estimated to account for 3-10% of resistance [1]. Amongst patients with secondary oncogenic fusion, ALK was the second most common resistance mechanism, accounting for 23% of the alterations, while BRAF fusion was the most common (32%) [9]. Here, we reviewed all reported cases of ALK fusion as a resistance mechanism to EGFR TKIs in the literature (Table 1).
A total of 16 cases of ALK fusion resistance to EGFR TKIs were recorded. Median time to development of ALK fusion resistance was 16 months (range: 6-34 months). The most common primary EGFR mutation was exon 19 deletion (56%; n = 9), while the L858R mutation consisted of 31% of the reported cases (n = 5). Most patients developed secondary ALK fusion after exposure to osimertinib (n = 12). However, three patients developed secondary ALK fusion after afatinib, while one patient developed ALK fusion after gefitinib. This indicated that secondary ALK fusion is not a resistance mechanism specific to treatment with osimertinib but secondary to EGFR TKIs treatment in general.
Most of the secondary ALK fusion gene was EML4::ALK fusion (68.8%; n = 11). However, there were multiple reported rare ALK fusion partners as well, including STRN, DCTN1, PLEKHA7, and TFG. Though EML4::ALK remained the most prevalent fusion type, this population is still highly enriched for uncommon ALK fusions (31.2%). For comparison, EML4 was documented to account for over 95% of fusion variants in de novo ALK mutant NSCLC [17].
Central nervous system (CNS) involvement was common. A total of 33% (n = 3) of all cases with reported disease site (n = 9) had CNS involvement. Secondary ALK mutant NSCLC showed a high propensity for CNS metastasis consistent with historical rates of CNS metastasis in de novo ALK mutant NSCLC [18]. This highlights the need for CNS-penetrating TKIs such as lorlatinib or alectinib, as well as CNS-directed local therapies.
ALK-directed TKI was effective in the treatment of secondary ALK fusion. For patients on combination EGFR and ALK-directed TKI, the objective response rate was 66.7% (stable disease = 3; partial response = 5; complete response = 1; N = 9). The most common regimen was osimertinib plus alectinib (n = 5), followed by osimertinib plus crizotinib (n = 4). Combination of EGFR inhibitor with ALK inhibitor was well tolerated without any grade three or beyond adverse events. The only grade three adverse event documented was brigatinib-induced interstitial lung disease whilst on single-agent brigatinib. The patient later tolerated osimertinib plus crizotinib without high-grade toxicities.
The above review of the literature demonstrated the effectiveness and safety of combination EGFR and ALK-directed TKIs in this rare acquired resistance [19]. Importantly, the combination of EGFR and ALK TKIs was effective in rare ALK fusion alterations as well. Given the propensity for CNS spread in EGFR and ALK co-altered tumors, osimertinib plus alectinib or lorlatinib would be preferable [18].
We acknowledged the following limitations for the current study. Firstly, generalizability is limited by the retrospective nature of the case report. Prospective registries may aid generalizability in the future. Secondly, there was a lack of serial circulating DNA monitoring. By monitoring circulating DNA, the clonal evolution of the present case can be studied. Finally, the literature review of case reports and case series was limited to pooling and comparison due to incomplete reporting of outcomes. Prospective basket trials on combination treatment with multiple TKIs may provide evidence on the efficacy of dual EGFR-ALK blockade.
Conclusions
Secondary ALK fusion represents a rare but clinically significant resistance mechanism for NSCLC patients treated with EGFR TKIs, occurring in a small number of resistance cases with a median time to development of 16 months. Comprehensive molecular profiling at the time of disease progression is essential for identifying this patient subgroup, as early detection enables prompt initiation of appropriate targeted therapy. Orthogonal validation with immunohistochemistry remains important when tissue is available to confirm NGS findings. This resistance mechanism is not specific to any particular EGFR TKI and has been observed across different generations of EGFR inhibitors. The molecular landscape of secondary ALK fusions differs from de novo ALK-positive NSCLC, with enrichment for uncommon fusion partners beyond the typical EML4-ALK rearrangement. CNS involvement is common at 33% in this patient population, emphasizing the importance of using CNS-penetrant targeted therapies. Combination therapy with EGFR and ALK inhibitors demonstrates promising efficacy with an objective response rate of 66.7% and an acceptable tolerability profile, making it a viable treatment option for this rare but actionable resistance mechanism.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Resistance mechanisms to osimertinib in EGFR-mutated non-small cell lung cancer Br J Cancer Leonetti A Sharma S Minari R Perego P Giovannetti E Tiseo M 72573712120193156471810.1038/s 41416-019-0573-8PMC 6889286 · doi ↗ · pubmed ↗
- 2A prospective, molecular epidemiology study of EGFR mutations in Asian patients with advanced non-small-cell lung cancer of adenocarcinoma histology (PIONEER)J Thorac Oncol Shi Y Au JS Thongprasert S 154162920142441941110.1097/JTO.0000000000000033 PMC 4132036 · doi ↗ · pubmed ↗
- 3Osimertinib in untreated EGFR-mutated advanced non-small-cell lung cancer N Engl J Med Soria JC Ohe Y Vansteenkiste J 11312537820182915135910.1056/NEJ Moa 1713137 · doi ↗ · pubmed ↗
- 4Assessment of resistance mechanisms and clinical implications in patients with EGFR T 790M-positive lung cancer and acquired resistance to osimertinib JAMA Oncol Oxnard GR Hu Y Mileham KF 15271534420183007326110.1001/jamaoncol.2018.2969 PMC 6240476 · doi ↗ · pubmed ↗
- 5Crizotinib versus chemotherapy in advanced ALK-positive lung cancer N Engl J Med Shaw AT Kim DW Nakagawa K 2385239436820132372491310.1056/NEJ Moa 1214886 · doi ↗ · pubmed ↗
- 6Molecular mechanisms of resistance to first- and second-generation ALK inhibitors in ALK-rearranged lung cancer Cancer Discov Gainor JF Dardaei L Yoda S 11181133620162743222710.1158/2159-8290.CD-16-0596 PMC 5050111 · doi ↗ · pubmed ↗
- 7Understanding and targeting resistance mechanisms in NSCLC Nat Rev Cancer Rotow J Bivona TG 6376581720172906800310.1038/nrc.2017.84 · doi ↗ · pubmed ↗
- 8Acquired EGFR C 797S mutation mediates resistance to AZD 9291 in non-small cell lung cancer harboring EGFR T 790M Nat Med Thress KS Paweletz CP Felip E 5605622120152593906110.1038/nm.3854 PMC 4771182 · doi ↗ · pubmed ↗