Effect of basic psychological satisfaction needs on resilience in patients with first acute myocardial infarction: the mediating role of family resilience and hope
Hong Ding, Liyun Miao, Yali Bai, Yan Wang

TL;DR
This study explores how meeting basic psychological needs can improve resilience in patients after their first heart attack, with family resilience and hope playing key mediating roles.
Contribution
The study identifies family resilience and hope as mediators linking basic psychological need satisfaction to psychological resilience in first-time heart attack patients.
Findings
Basic psychological needs satisfaction positively predicts psychological resilience through family resilience and hope.
Four significant mediation pathways were confirmed between basic psychological needs and resilience.
Family resilience and hope are critical for enhancing patient outcomes after acute myocardial infarction.
Abstract
Psychological resilience is key to coping with adversity, stress buffering, and trauma. Acute myocardial infarction (AMI), a major life event, triggers severe psychological stress, especially in first-time patients facing heightened adversity. This diminishes resilience and worsens the prognosis. Evidence links basic psychological need satisfaction to resilience, but the mediating roles of family resilience and hope remain untested. This study aimed to explore the influence of psychological satisfaction needs on the psychological resilience of patients with first-time AMI, and to investigate the chain intermediary role of family resilience and hope in it. This cross-sectional study was conducted from June 2023 to June 2025. Patients with first-time AMI and treated at our hospital were enrolled via convenience sampling. Data were collected using Basic Psychological Needs Scales (BPNS),…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
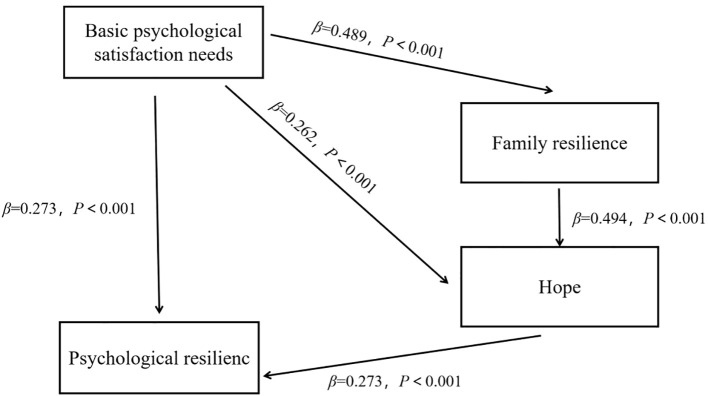 Figure 1
Figure 1| Variables | Cases/ | |
|---|---|---|
| Age (year) | ≥60 | 84 (46.93) |
| <60 | 95 (53.07) | |
| Gender (n,%) | Male | 92 (51.40) |
| Female | 87 (48.60) | |
| Degree of education (n,%) | Junior high school and below | 49 (27.37) |
| High school and above | 130 (72.63) | |
| Marital status (n,%) | Unmarried | 40 (22.35) |
| Married | 84 (46.93) | |
| Divorce | 42 (23.46) | |
| Spouse | 13 (7.26) | |
| Religious beliefs (n,%) | Yes | 37 (20.67) |
| No | 142 (79.33) | |
| Average family monthly income (n,%) | <2000 yuan | 31 (17.32) |
| 2000~4000 yuan | 85 (47.49) | |
| >4000 yuan | 63 (35.20) | |
| Source of cost (n,%) | New farming | 72 (40.22) |
| Employee medical insurance | 69 (38.55) | |
| Self-pay | 38 (21.23) | |
| Whether complicated with hypertension (n,%) | Yes | 61 (34.08) |
| No | 118 (65.92) | |
| BMI(kg/m2) | 24.38 ± 3.86 | |
| Killip grade (n,%) | I | 37 (20.67) |
| II | 68 (37.99) | |
| III | 74 (41.34) | |
| Length of hospital stay (d) | 16.59 ± 4.16 | |
| Item | Scare ( | |
|---|---|---|
| CD-RIS | Tenacity | 27.12 ± 1.81 |
| Optimism | 16.89 ± 1.92 | |
| Strength | 18.94 ± 1.98 | |
| BPNS | Independent needs | 40.31 ± 5.38 |
| Competency needs | 38.76 ± 4.52 | |
| Attribution needs | 31.28 ± 4.10 | |
| FRAS | Dilemma solution | 3.98 ± 0.84 |
| Forward-looking | 3.54 ± 0.84 | |
| Excellent life | 3.61 ± 0.71 | |
| Problem solving | 3.75 ± 0.78 | |
| Intimacy and harmony | 3.84 ± 0.83 | |
| Social support | 3.45 ± 1.13 | |
| Order well | 3.72 ± 1.09 | |
| Emotional sharing | 3.85 ± 1.02 | |
| Clear communication | 3.83 ± 0.93 | |
| Cooperation and coordination | 3.71 ± 1.01 | |
| HHI | T | 7.63 ± 1.88 |
| P | 8.69 ± 1.94 | |
| I | 8.31 ± 2.11 | |
| Item | CD-RIS | BPNS | FRAS | HHI |
|---|---|---|---|---|
| CD-RIS | 1 | |||
| BPNS | 0.513** | 1 | ||
| FRAS | 0.514** | 0.489** | 1 | |
| HHI | 0.541** | 0.504** | 0.622** | 1 |
| Item | FRAS | HHI | CD-RIS | ||||||
|---|---|---|---|---|---|---|---|---|---|
| SE |
|
| SE |
|
|
|
|
| |
| Constant | 6.328 | -0.087 | – | 3.276 | 0.415 | – | 3.293 | -0.06 | – |
| BPNS | 0.057 | 6.041** | 0.489 | 0.034 | 3.275** | 0.262 | 0.035 | 3.126** | 0.273 |
| FRAS | 0.048 | 6.169** | 0.494 | 0.056 | 2.188** | 0.211 | |||
| HHI | 0.094 | 2.803** | 0.273 | ||||||
|
| 0.243 | 0.438 | 0.397 | ||||||
|
| 0.336 | 0.428 | 0.382 | ||||||
| Model effect | Effect | Boot SE | BootLLCI | BootULCI |
|
|
|---|---|---|---|---|---|---|
| Basic psychological satisfaction needs⇒Psychological resilience | 0.098 | 0.046 | 0.157 | 0.335 | 2.141 | 0.032 |
| Basic psychological satisfaction needs⇒Family resilience⇒Psychological resilience | 0.042 | 0.049 | 0.010 | 0.205 | 0.857 | 0.391 |
| Basic psychological satisfaction needs⇒Hope ⇒Psychological resilience | 0.029 | 0.034 | 0.015 | 0.146 | 0.85 | 0.395 |
| Basic psychological satisfaction needs⇒Family resilience⇒Hope⇒Psychological resilience | 0.027 | 0.027 | 0.019 | 0.125 | 0.988 | 0.323 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsResilience and Mental Health · Cardiac Health and Mental Health · COVID-19 and Mental Health
Introduction
1
Acute myocardial infarction (AMI), defined as ischemic myocardial necrosis resulting from acute coronary occlusion and insufficient blood perfusion, typically manifests as crushing chest pain with high mortality and disability rates (1). The development of AMI is closely associated with emotional stress and behavioral patterns, establishing a vicious cycle through interactions between psychological-behavioral and somatic factors (2).
Psychological resilience refers to an individual's capacity to process severe stressors and adverse events (3). This construct constitutes a critical element in mental health cultivation and psychological crisis intervention. Studies confirm that resilience functions as a protective factor against psychological distress, fostering stress resistance and facilitating positive adaptation to adversity (4, 5). Given the sudden onset, life-threatening nature, and lack of coping experience, first-time AMI patients frequently develop severe psychological shock due to intense fear of poor prognosis, significantly reducing resilience levels (6). Diminished resilience not only amplifies psychological distress but also directly compromises treatment adherence and rehabilitation progress, potentially elevating risks of major adverse cardiovascular events (MACE) (7). Consequently, assessment of psychological resilience and its influencing factors in first-time AMI patients carries vital clinical significance (8). This approach enables disruption of the psychosomatic vicious cycle, development of precise psychological interventions, and ultimately improvement in patients' quality of life and disease prognosis.
The basic psychological needs theory posits that humans possess three fundamental psychological needs: autonomy, relatedness, and competence (9). When autonomy needs are fulfilled, patients more effectively engage in shared treatment decision-making, enhancing their sense of control during clinical processes. This is essential for developing psychological resilience and facilitating positive adaptation to health challenges. The satisfaction of belongingness needs fosters robust social support, which helps to buffer the stress of illness, sustain psychological resilience, and mobilize external resources (10). While the satisfaction of competence needs can improve self-efficacy, helping patients rebuild their confidence and promoting their internal resources to cope with adversity. Consequently, satisfaction of these three basic psychological needs correlates significantly with mental health and establishes the foundation for building and maintaining psychological resilience (11). Therefore, the state of basic psychological need satisfaction in first-time AMI patients not only associates with their resilience levels but also critically influences psychosomatic recovery trajectories. Nevertheless, the precise pathways and mechanisms mediating these effects warrant further exploration.
Family resilience refers to a family system's capacity to achieve healthy adaptation when confronting adversity or stress (12). Strong family resilience mitigates patients' negative psychological states such as anxiety and depression, exerting profound positive impacts on their physical and mental health. Hope, defined as a positive psychological state enabling individuals to believe in overcoming life challenges and achieving personal goals, empowers patients to establish clearer objectives and pursuits (13). Elevated hope levels enhance psychological resilience, while improved resilience reciprocally sustains hope.
Therefore, both family resilience and hope significantly influence patients' basic psychological need satisfaction. Building on this theoretical framework, this study aims to investigate the impact of basic psychological needs satisfaction on resilience among first-time AMI patients, examining the chain mediation effects of family resilience and hope. These findings will provide theoretical foundations and identify potential intervention targets for enhancing resilience in this population.
Methods
2
Participants
2.1
From June 2023 to June 2025, patients with AMI treated in our hospital were selected by convenient sampling as the research object.
Inclusion criteria: (1) a confirmed diagnosis of AMI, including both ST-segment elevation myocardial infarction (STEMI) and non-ST-segment elevation myocardial infarction (NSTEMI), based on standard clinical diagnostic criteria (14); (2) first onset; (3) have a certain understanding ability, can communicate in language or in writing; (4) all patients underwent coronary angiography and percutaneous coronary intervention.
Exclusion criteria: (1) persons with mental illness, audio-visual impairment or severe cognitive impairment; (2) malignant tumor or severe heart failure and respiratory failure; (3) previous history of mental illness such as depression and anxiety; (4) the clinical data are incomplete or they are still unwilling to cooperate with this researcher after explanation.
Research methods
2.2
Clinical data collection
2.2.1
Clinical data were collected from patient interviews and medical records. Collected variables included age, gender, education level, marital status, family per capita monthly income, source of expenses, whether they are complicated with hypertension and BMI. The number of people to be investigated should be 1015 times that of the items included in the survey. There are 15 items in this study, and 150225 cases should be investigated. Considering the loss rate of 10%~30%, the sample size is at least 165 cases, and the sample size of this study is 186 cases.
investigation of psychological resilience
2.2.2
The Connor-Davidson Resilience Scale (CD-RIS) was used to evaluate the mental resilience of all patients. This scale contains three factors, namely, resilience, optimism and strength, and 10 items, each of which is 0–4 points, with 0 indicating that this is not the case at all and 4 indicating that it is almost always the case. The higher the score, the higher the psychological resilience (15).
investigation of basic psychological needs
2.2.3
The basic psychological needs scales (BPNS) were used to evaluate the basic psychological needs of all patients, including autonomous needs, competence needs and belonging needs, with 21 items. Likert 7-level scoring method is adopted, and "complete non-conformity" and "complete conformity" are scored 1–7 respectively, with a total score of 21-147. The higher the score, the higher the degree of demand satisfaction (16).
investigation of family resilience
2.2.4
The family resilience assessment scale (FRAS) was used to evaluate the family resilience of all patients. The scale included 10 dimensions, including dilemma interpretation, forward-looking, excellent life, problem solving, intimacy and harmony, social support, orderly, emotional sharing, clear communication and cooperation and coordination, with 49 items. Likert's 5-level score was used, ranging from "non-conformity" to "conformity" (17).
investigation of hope
2.2.5
The Herth Hope Index (HHI) was used to evaluate the hope level of all patients, which consisted of 12 items in 3 dimensions. The dimensions of "temporary attitude and future (T)" respectively include items 1, 2, 6 and 11. The dimension of "positive readiness and expectancy (P)" includes items 4, 7, 10 and 12; And the "inter-connectedness (I)" dimension includes items 3, 5, 8 and 9. The scale adopts Likert14 scale, and the score range is 048. The higher the score, the higher the hope level (18).
Quality control
2.3
All questionnaires were distributed and collected by researchers. Before filling in, the purpose of this study was explained to patients, and all respondents agreed to fill in. In the process of filling in, unified instructions were used, and all questionnaires were collected on the spot.
Data processing
2.4
All statistical analyses were conducted using SPSS version 24.0 (IBM Corp., Armonk, NY, USA). Descriptive statistics were used to summarize the demographic and clinical characteristics. Categorical variables are reported as frequencies and percentages, while continuous variables were tested for normality using the Shapiro–Wilk test. Normally distributed data are expressed as mean ± standard deviation (± SD). Correlation analyses were conducted to assess the associations between key variables. To evaluate the mediation effects, a bootstrap resampling method with 1,000 iterations and bias-corrected confidence intervals was employed. A mediation effect was considered statistically significant if the 95% confidence interval did not include zero.
Results
3
General information of patients
3.1
In this study, a total of 186 questionnaires were distributed, 7 invalid questionnaires were excluded, and 179 questionnaires were finally recovered, with an effective rate of 96.24%. The general information of all subjects is shown in Table 1.
The scores of CD-RIS, BPNS, FRAS and HHI in 179 patients with first-time AMI
3.2
A total of 179 first-time AMI patients showed mean scores of (62.95 ± 5.71) on the CD-RISC, (110.35 ± 14.00) on the BPNS, (37.28 ± 9.87) on the FRAS, and (24.63 ± 5.93) on the HHI. The scores of each dimension of each scale are shown in Table 2.
Correlation analysis of CD-RIS, BPNS, FRAS and HHI in patients with first-time AMI
3.3
There is a positive correlation between CD-RIS and BPNS, FRAS and HHI in patients (P < 0.001), as shown in Table 3.
Analysis of intermediary effect
3.4
The total effect of basic psychological satisfaction needs of patients with first-time AMI is significant (β=0.273, P < 0.001), and the direct prediction of psychological resilience is significant. Basic psychological satisfaction can positively predict family resilience (β=0.489, P < 0.001) and hope level (β=0.262, P < 0.001). At the same time, both family resilience and hope level can positively predict patients' psychological resilience (β = 0.211, 0.273; P < 0.001), as shown in Table 4.
Mediation effect test
3.5
An intermediary pathway analysis is established to explore the indirect influence of basic psychological satisfaction needs on psychological resilience. The tested pathways included (1) Basic psychological satisfaction needs→Psychological resilience, (2) Basic psychological satisfaction needs→Family resilience→Psychological resilience, (3) Basic psychological satisfaction needs→Hope→Psychological resilience, and (4) Basic psychological satisfaction needs→Family resilience→Hope→Psychological resilience. The 95% CI of each path is (0.01570.335), (0.0100.205), (0.0150.146) and (0.0190.125), respectively, all of which do not include 0, indicating that all the mediating effect paths exist. The detailed results are presented in Table 5 and illustrated in Figure 1.
Chain mediation model of basic psychological satisfaction needs, psychological resilience, family resilience and hope level of patients with first-time AMI.
Discussion
4
This study reveals that the psychological resilience score of first-time AMI patients (62.95 ± 5.71) falls below normative thresholds. This result is significantly lower than that reported by N.L. et al. in their survey of general AMI patients (19). The discrepancy may stem from the exclusive inclusion of first-onset cases in our cohort. As an acute cardiovascular emergency, AMI often evokes a sense of impending doom, causing not only physical deterioration but also multifaceted stressors, such as decreased self-care ability, heavy economic burden and lack of various social roles (20). Confronted with these challenges, patients frequently demonstrate limited crisis management abilities, hindering effective coping strategies (21). Consequently, their psychological resilience levels remain suboptimal, exacerbating negative emotions and adversely affecting prognosis. It is suggested that clinicians prioritize psychological resilience assessments in first-time AMI patients to enhance mental health outcomes and facilitate better psychosocial adaptation.
Our correlation analysis shows that there is a positive correlation between CD-RIS and BPNS scores in patients with first-time AMI, and the total effect of basic psychological satisfaction needs on psychological resilience is significant (β=0.273, P < 0.001), demonstrating a positive predictive relationship. The degree of basic psychological need satisfaction is the performance of the individual's ability to participate in activities independently, show the ability to achieve goals and establish good relations with others (22). Previous studies confirm that patients with greater basic psychological need satisfaction exhibit enhanced subjective well-being, more positive emotional experiences, and improved social adaptation (23). Conversely, unmet basic psychological needs significantly increase risks for depression and other psychological/behavioral disorders (24, 25). Notably, robust psychological resilience buffers against adverse environmental influences, enabling patients to more readily achieve a high level of independent demand satisfaction, competent demand satisfaction and belonging demand satisfaction. Consequently, clinical nursing practice for first-time AMI patients should incorporate structured psychological support designed to improve disease-specific knowledge and rehabilitation awareness, which is essential for promoting basic psychological need satisfaction and facilitating positive adaptation to illness.
Mediating effect analysis of this study shows that basic psychological need satisfaction can positively predict family resilience and hope (β=0.489, 0.262, P < 0.001). At the same time, both family resilience and hope can positively predict patients' psychological resilience (β = 0.211, 0.273, P < 0.001). The results suggest that family resilience and hope constitute significant determinants of psychological resilience in this population. Critically, the effects of basic psychological need satisfaction, family resilience, and hope on psychological resilience function synergistically rather than independently (4). Hope level individuals tend to show stronger willpower, and such patients are more concerned about reality and willing to actively solve problems. Strong family resilience provides patients with stable emotional support, unconditional acceptance, and a collaborative problem-solving environment, which reduces their anxiety and fear and fosters a positive attitude toward the disease. Conversely, when family members experience poor psychological well-being, it can increase intra-family tension, thereby depleting the family's supportive resources. This shortage of resources makes it difficult for patients to receive adequate care and support, ultimately accelerating the decline in their hope levels (26–29). These results underscore the importance of integrating family-focused educational interventions into clinical nursing. Clinicians should encourage patients' families to provide robust emotional and practical support, as effective family assistance is crucial for promoting the patient's psychological well-being.
Further validation of mediation pathways confirms the significance of each path. Among them, the path of basic psychological satisfaction needs⇒family resilience⇒hope⇒psychological resilience has the highest clinical practicality. These findings indicate that basic psychological need satisfaction ultimately enhances psychological resilience through two synergistic mechanisms: strengthening family support systems and cultivating individual hope (30). Therefore, in clinical intervention, it is suggested to adopt various methods such as group psychological counseling, online and offline health education, and continuing nursing to meet patients' basic psychological needs as much as possible, and to improve family resilience and hope level by means of synchronous family intervention and peer education, so as to systematically enhance patients' psychological resilience in coping with first-time AMI.
However, this study is limited by its cross-sectional design, which only captures the participants' status at a single time point and cannot delineate their dynamic changes over time. Future research should employ longitudinal or intervention designs in first-time AMI patients to track the trajectory of psychological resilience and its influencing factors across different post-onset periods. Furthermore, the generalizability of the findings may be constrained by the relatively small sample size. Future studies with larger, more diverse samples and higher levels of evidence are warranted to further validate the effects of family resilience and hope on satisfying basic psychological needs and fostering psychological resilience.
Conclusion
5
This study analyzes the complex interaction among the basic psychological satisfaction needs, psychological resilience, family resilience and hope level of patients with first-time AMI. The results show that family resilience and hope serve as mediators between basic psychological need satisfaction and psychological resilience in patients with first-time AMI. Clinical care should coordinate community and family resources to enhance external social support and psychosocial companionship, so as to improve patients' psychological resilience and ultimately promote better disease prognosis.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Arabadjian M Duberstein ZT Sperber SH Kaur K Kalinowski J Xia Y. Role of Resilience in the Psychological Recovery of Women With Acute Myocardial Infarction. J Am Heart Assoc. (2023) 12:e 027092. doi: 10.1161/JAHA.122.027092, PMID: 37026542 PMC 10227277 · doi ↗ · pubmed ↗
- 2Wang J Wu Y Zhou J Li S She L. Resilience and its influencing factors after emergency percutaneous coronary intervention in young and middle-aged patients with first acute myocardial infarction. Sci Rep-UK. (2024) 14:9507. doi: 10.1038/s 41598-024-59885-9, PMID: 38664486 PMC 11045793 · doi ↗ · pubmed ↗
- 3Troy AS Willroth EC Shallcross AJ Giuliani NR Gross JJ Mauss IB. Psychological Resilience: An Affect-Regulation Framework. Annu Rev Psychol. (2023) 74:547–76. doi: 10.1146/annurev-psych-020122-041854, PMID: 36103999 PMC 12009612 · doi ↗ · pubmed ↗
- 4Wang Y Qiu Y Ren L Jiang H Chen M Dong C. Social support, family resilience and psychological resilience among maintenance hemodialysis patients: a longitudinal study. BMC Psychiatry. (2024) 24:76. doi: 10.1186/s 12888-024-05526-4, PMID: 38279114 PMC 10811847 · doi ↗ · pubmed ↗
- 5Imran A Tariq S Kapczinski Fde Azevedo CT. Psychological resilience and mood disorders: a systematic review and meta-analysis. Trends Psychiatr Psy. (2024) 46:e 20220524. doi: 10.47626/2237-6089-2022-0524, PMID: 36215270 PMC 11332678 · doi ↗ · pubmed ↗
- 6ZábóV Csiszar A Ungvari Z Purebl G. Psychological resilience and competence: key promoters of successful aging and flourishing in late life. Geroscience. (2023) 45:3045–58. doi: 10.1007/s 11357-023-00856-9, PMID: 37418098 PMC 10643728 · doi ↗ · pubmed ↗
- 7Jones JM. Surviving While Black: Systemic Racism and Psychological Resilience. Annu Rev Psychol. (2023) 74:1–25. doi: 10.1146/annurev-psych-020822-052232, PMID: 36652304 · doi ↗ · pubmed ↗
- 8Thabet A Ghandi S Barker EK Rutherford G Malekinejad M. Interventions to enhance psychological resilience in forcibly displaced children: a systematic review. BMJ Glob Health. (2023) 8:e 007320. doi: 10.1136/bmjgh-2021-007320, PMID: 36731918 PMC 9896216 · doi ↗ · pubmed ↗