Safety and Efficacy of Intraoperative Neuromonitoring: An Umbrella Review
Aziz Rezapour, Naser Derakhshani, Seyedeh Narges Pouyan, Vahid Alipour, Seyed Jafar Ehsanzadeh, Arash Zare‐Sadeghi, Jalal Arabloo

TL;DR
This umbrella review evaluates the safety and effectiveness of intraoperative neuromonitoring in various surgeries, finding mixed evidence and a need for more research.
Contribution
The study provides a comprehensive umbrella review of IONM's clinical outcomes across multiple surgical procedures.
Findings
IONM reduces the risk of recurrent laryngeal nerve injury in thyroidectomy.
Combined EEG and SSEP monitoring improves sensitivity in carotid endarterectomy.
BIS-guided anesthesia does not reduce consciousness risk.
Abstract
Intraoperative neuromonitoring (IONM) plays a crucial role in several surgical procedures. This study aimed to review the safety and efficacy evidence of IONM technology. A comprehensive search was conducted in databases, including PubMed, Scopus, Web of Science core collection, Embase, and Cochrane library. Systematic reviews and meta‐analyses assessing clinical outcomes, safety, and diagnostic accuracy in patients undergoing neurosurgery with and without IONM were included. Methodological quality was assessed using the JBI tool. The present umbrella review followed the PRISMA guidelines. A total of 48 systematic reviews and meta‐analyses were included in this study. The evidence demonstrated that IONM is clinically effective in reducing the risk of temporary recurrent laryngeal nerve paralysis and overall recurrent laryngeal nerve injury after thyroidectomy. Moreover, the use of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
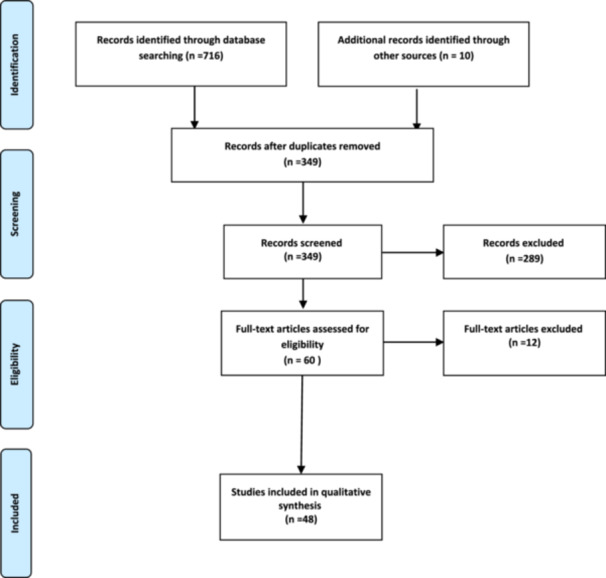 Figure 1
Figure 1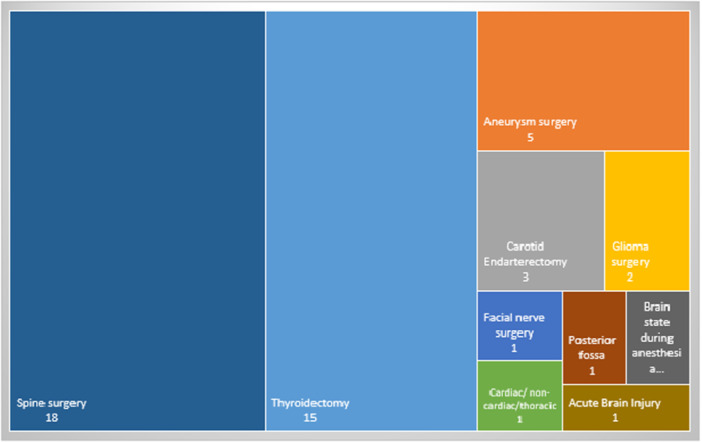 Figure 2
Figure 2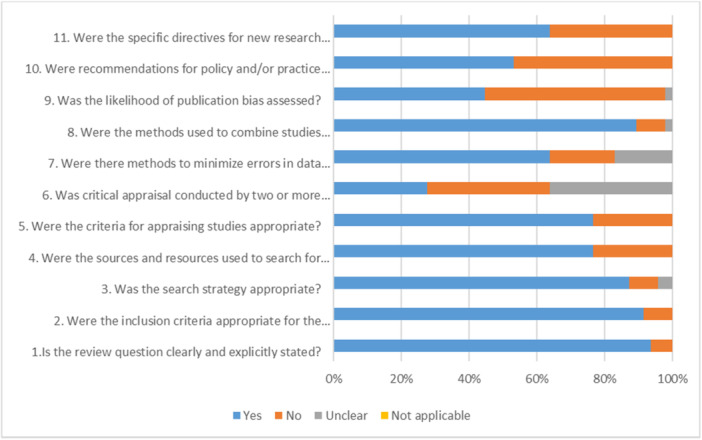 Figure 3
Figure 3| Database | Search strategy | # Results |
|---|---|---|
| PubMed | “Intraoperative Neurophysiological Monitoring”[Mesh] OR “neurophysiologic* monitoring*”[tiab] OR “Intraoperative Neurophysiologic*”[tiab] OR neuromonitoring[tiab] Filters: Meta‐Analysis, Systematic Review | 83 |
| Embase | (‘neuromonitoring’/exp OR ‘intraoperative neurophysiological monitoring’/exp OR ‘intraoperative neurophysiological monitoring’ OR ‘intraoperative neuromonitoring’/exp OR ‘intraoperative neuromonitoring’ OR ‘neurophysiological monitoring’/exp OR ‘neurophysiological monitoring’) AND ‘human’/de AND (‘meta analysis’/de OR ‘meta analysis topic’/de OR ‘systematic review’/de OR ‘systematic review topic’/de) | 257 |
| Web of Science core collection |
TS = (“Intraoperative Neurophysiologic* Monitoring” OR “neurophysiologic* monitoring*” OR “Intraoperative Neurophysiologic*” OR neuromonitoring) AND TS = (“meta analysis” OR “meta‐analysis” OR “systematic review”) Timespan: All years. Indexes: SCI‐EXPANDED, SSCI, A&HCI, ESCI. | 85 |
| Scopus | (TITLE‐ABS‐KEY ((“neuromonitoring” OR “intraoperative neurophysiological monitoring” OR “intraoperative neuromonitoring” OR “neurophysiological monitoring”)) AND TITLE‐ABS‐KEY (“meta analysis” OR “meta‐analysis” OR “systematic review”)) | 290 |
| Cochrane Reviews | MeSH descriptor: [Intraoperative Neurophysiological Monitoring] explode all trees | 1 |
| Additional records identified through other sources | 10 | |
| Total | 726 |
| Author & year | Type of study | Study objective | Databases | Searching time | Number and type of included studies | Quality assessment | Quality assessment tool | Analysis | Type of statistical analysis | Measures |
|---|---|---|---|---|---|---|---|---|---|---|
| [ | Systematic review and meta‐analysis | Evaluation of the effects of IONM compared with visual identification of the nerve to prevent RILN injury in adults undergoing thyroid surgery. | CENTRAL, MEDLINE, Embase, ICTRP Search Portal, and Clinicaltrials.gov. (21 August 2018) | 2013–2018 | 5 Randomized controlled trial study (RCT) | Yes | GRADE | Yes | Random effect model | Risk ratio |
| [ | Systematic review | Investigation and evaluation of the use of IONM in endoscopic thyroidectomy |
CENTRAL, MEDLINE, Cochrane, and EMBASE (from January 1, 2000, to September 1, 2016) | 2000–2015 | 9 studies (6 retrospective studies/3 randomized prospective studies) | No | No | No | No | — |
| [ | Meta‐analysis | Comparison of the effect of the recurrent laryngeal nerve (RLN) compared to RLN identification alone on the actual degree of vocal cord paralysis after thyroidectomy. | MEDLINE (1966‐July 2008), EMBASE (1980‐July 2008), Cochrane Central Register of Clinical Trials (CENTRAL), Cochrane Database of Systematic Reviews, clinicaltrials.gov, and The National Guideline Clearinghouse databases | 2009– 1991 | 43 studies (1 Randomized clinical trial، 7 comparative trials 34 case series) | Yes | CONSORT | Yes | Random effect model | Odd ratio |
| [ | Meta‐analysis | Conducting a meta‐analysis of the combined results of individual studies to measure the frequency of RLN and EBSLN injuries in patients undergoing neuromonitoring during thyroidectomy compared to the usual method of identification | The Cochrane Central Register of Controlled Trials (CENTRAL) on The Cochrane Library (2012), The National Library of Medicine (PubMed) (1966–December 2012), EMBASE (1980–December 2012) and The Latin American and Caribbean Health Sciences Library (LILACS) (1980–December 2012). | 2009–2012 | 6 Randomized controlled trial study | Yes | GRADE | Yes | Random effect model | Risk difference |
| [ | Meta‐analysis | To evaluate whether IONM can reduce the incidence of RLN palsy to a greater extent than visual identification of RLN alone in re‐thyroid surgeries | PubMed, SCIE and Wan Fang databases/studies published up to 31 August 2016. | 2004–2014 | 9 studies (2 study prospective cohort7 study retrospective cohort) | Yes | Newcastle‐Ottawa Scale (NOS) | Yes | Random effect model | Risk ratio |
| [ | Systematic review and meta‐analysis | To evaluate the role of IONM in reducing RLN paralysis during high‐risk thyroidectomy and to identify which high‐risk subgroups will benefit the most. | Pubmed, Medline, Embase and Cochrane central register of clinical trials (CENTRAL) from 1st January 2000 to 30th June 2015 | 2004–2014 | 10 studies (2 study prospective comparative and 8 study retrospective) | Yes | Newcastle‐Ottawa Scale (NOS) | Yes | Fixed effect model | Odd ratio |
| [ | Meta‐analysis | Using the meta‐analysis method to evaluate the role of IN in helping thyroid surgery | PubMed, Embase, and the Cochrane library from January 1, 2004 to July 30, 2016. | 2004– 2016 | 24 studies (4 Randomized controlled trial studies & 20 study RCS) | Yes | Cochrane Collaboration tool | Yes | Random effect model | Odd ratio |
| [ | Meta‐analysis | To evaluate the effect of IONM during thyroid surgery | The web‐based PubMed database (1950 through April 2011), Embase (1974 through April 2011), and the Cochrane Central Register of Controlled Trials (CENTRAL, The Cochrane Library, Issue 2 of 4, April 2011) | 1992– 2009 | 14 (2 randomized clinical trials & 12 comparative studies) | Yes | Cochrane Risk of Bias tool | Yes | Random effect model | Odd ratio |
| [ | Meta‐analysis | Determining the benefit of using intermittent neuromonitoring during surgery to prevent permanent nerve paralysis |
PubMed, Scopus, and Cochrane Central Register of Controlled Trials until August 2014 | 2004–2014 | 14 studies (4 randomized controlled trials) & (10 studies on‐randomized controlled trials (NRS)) | Yes | Cochrane Collaboration's tool | Yes | Fixed effect model | Risk ratio/risk difference |
| [ | Systematic review and meta‐analysis | Evaluation of the advantage of IONM in identifying EBSLN during thyroid surgery | MEDLINE, PubMed, Web of Science, and Cochrane Library January 1, 1995, through July 1, 2018 | 2009–2016 | 7 study | Yes | Cochrane Collaboration tool | Yes | Random effect model | risk ratio |
| [ | Systematic review and meta‐analysis | Risk estimation of bilateral RLN paralysis with and without intraoperative neuromonitoring | PubMed, Scopus (EMBASE), and the Cochrane Library in the period 2000‐2014 | 2000–2014 | 40 studies (…. clinical trials, …. cohort studies case series) | No | No | Yes | Random effect model | Adjusted incidence/risk ratio |
| [ | Systematic review and meta‐analysis | Assessing the potential improvement of IONM versus visual identification of RLN alone (VA) in reducing the incidence of vocal cord paralysis | Embase, Medline, Cochrane, PubMed, and Google Scholar databases in August 2013 | 2004–2013 | 20 studies (3 prospective randomized trials,7 prospective trials & 10 studies observational retrospective) | Yes | MOOSE | Yes | Fixed effect model | Standardized Mean Difference |
| [ | Systematic review | Evaluating the effectiveness of intraoperative neuromonitoring (IONM) in preventing recurrent laryngeal nerve palsy (RLNP) during thyroid surgery. | MEDLINE, EMBASE, and PubMed from 1999 forwards | 2004–2014 | 17 studies (12 comparative studies ، 1 randomized clinical trial ، 2 non‐randomized clinical trials & 2 studies) | No | No | No | Not reported | Not reported |
| [ | Meta‐analysis | Determination of the effects of IONM in thyroidectomy |
MEDLINE (PubMed), BIOSIS Previews (ISI Web of Knowledge) and Cochrane library from January 1980 to July 2017 | 2002–2017 | 34 studies (3 randomized controlled trials 3 & non‐randomized trials) | Yes | Newcastle‐Ottawa Scale (NOS) | Yes | Random effect model | Risk ratio/risk difference |
| [ | Meta‐analysis | Evaluation of the risk of temporary or permanent RLN damage in thyroid surgery with or without IONM | PubMed and Ovid, and the Cochrane Library database from January 1994 to February 2012 | 2002–2009 | 8 studies (2 randomized trials 6 comparative study‐randomized) | No | No | Yes | Fixed effect model | Risk ratio |
| Author & Year | Type of study | Study objective | Databases | Searching time | Number and type of included studies | Quality assessment | Quality assessment tool | Analysis | Type of statistical analysis | Index |
|---|---|---|---|---|---|---|---|---|---|---|
| [ | Systematic review و meta‐analysis | To evaluate whether IOM can prevent nerve damage during clipping of intracranial aneurysm | PubMed/Medline, Scopus, and Cochrane databases. January 1999 and January 2019 | 2010–2019 | 4 studies (three studies including group retrospective studies (before and after using IOM) and one prospective cohort study to evaluate IOM changes during MCA aneurysm surgery | Yes | MINORS | Yes | Random effect model | Odd ratio |
| [ | Systematic review | Evaluation: (a) diagnostic accuracy of cEEG as a confirmatory test, (b) prognostic value of EEG patterns indicative of seizures and DCI, and (c) efficacy of neuromonitoring using cEEG in terms of improving clinical outcome following SAH | Cochrane Central Register of Controlled Trials (The Cochrane Library), Medline (PubMed), EMBASE, Scopus, from January 1, 1980 to June 15,2014 | 1991–2014 | 18 studies (single‐center case series (including a randomized clinical trial) | Yes | QUADAS‐2 | No | — | |
| [ | Systematic review و meta‐analysis | Investigating the diagnostic accuracy of different evoked potential monitoring techniques in predicting postoperative neurological deficits in brain aneurysm surgery | MEDLINE, Embase and Cochrane databases 1983 through March 2016 | 1994–2013 | 15 prospective study | Yes | QUADAS | Yes | Random effect model | |
| [ | Meta‐analysis | To assess the accuracy of the intraoperative evoked potential (EP) diagnostic test (DTA) for the diagnosis of brain injury during brain aneurysm surgery. | EDLINE, EMBASE, LILACS, IndMed and a variety of other sources from 1 January 1960 to 5 January 2016 (last updated on 27 June 2018) | 1987– 2017 | 35 observational studies (prospective and retrospective clinical studies) | Yes | QUADAS‐2 | Yes | Random effect model | |
| [ | Systematic review | Evaluation of the benefit and application of neuromonitoring in descending aneurysm repair surgery and thoracoedema (DTA and TAAAR). |
OVID Medline, PUBMED, Scopus, and COCHRANE (from their dates of inception until February 2014) | 1999– 2013 | 15 prospective and retrospective study | No | — | No | — | — |
| Author & year | Type of surgery | Type of study | Study objective | Databases | Searching time | Number and type of included studies | Quality assessment | Quality assessment tool | Analysis | Type of statistical analysis |
|---|---|---|---|---|---|---|---|---|---|---|
| [ | Carotid endarterectomy | Meta‐analysis | Evaluating the efficacy of intraoperative SSEP change in predicting the risk of stroke in the postoperative period: more than 24 h but within 30 days | PubMed, Web of Science, and Embase | 1985–2015 | 25 prospective and retrospective studies | No | No | Yes | Bivariate normal model |
| [ | Carotid endarterectomy | Meta‐analysis | To determine whether multimodal monitoring leads to increased diagnostic sensitivity and accuracy? | Embase, PubMed, and Web of Science databases from 1945 through 26th March 2015 | 1995–2012 | 4 prospective and retrospective studies | Yes | QUADAS 2 | Yes | Bivariate model |
| [ | Carotid endarterectomy | Meta‐analysis | To determine the diagnostic accuracy of electroencephalogram (EEG) in predicting postoperative strokes through a meta‐analysis of existing literature. | PubMed and Web of Science databases for relevant literature from 1945 through 8 August 2014 | 1975– 2007 | 30 prospective and retrospective clinical trial studies | Yes | QUADAS | Yes | Bivariate model |
| [ | Glioma surgery | Systematic review & meta‐analysis | Investigation of early and permanent postoperative defects in patients who underwent insular glioma surgery using awake craniotomy with direct electrical stimulation (DES) versus surgery under general anesthesia. |
PubMed, Ovid MEDLINE, and Ovid EMBASE (January 1990 to January 2018) | 1997–2016 | 5 prospective and 3 retrospective studies | Yes | Newcastle‐Ottawa Scale | Yes | Random effect model |
| [ | Glioma surgery | Systematic review | Investigating the effect of assistive technologies during surgery on the rate of risk (EOR) in glioma surgery, compared to conventional unassisted surgery. | MEDLINE (PubMed), Scopus, Web of Science, and SciELO (2006 ‐2014) | 2006– 2013 | 6 prospective controlled studies | No | No | No | No |
| [ | Cardiac/noncardiac/chest surgery | Systematic review & meta‐analysis | Evaluating the effectiveness of brain monitoring of the depth of anesthesia in reducing postoperative cognitive function and postoperative delirium | MEDLINE, EMBASE, and Cochrane Library databases NA | 2011–2013 | 5 clinical trials | No | No | Yes | Random effect model |
| [ | Tumor surgery of skull base and Cerebellopontine Angle | Systematic review | To review the current literature with emphasis on all aspects of FN monitoring for Cerebellopontine Angle and skull base tumor from description to NO success in predicting the performance of standard and emerging monitoring methods. | PubMed (up to February 2011) | DES: (1979 –2010) free‐running EMG: (1987‐2010) FMEP: (2001–2011) | In DES, 27 retrospective studies and 35 prospective studies/in EMG 6 retrospective studies and seven prospective studies/in FMEP 3 retrospective studies and 3 prospective studies | No | No | No | No |
| [ | Posterior fossa surgery | Systematic review | The review of the available evidence has been carried out with an objective study; an intraoperative examination of the neural circuits involved in the pathophysiology of cerebellar mutism syndrome | PubMed central (Searching Date Not Mentioned) | not mentioned | 2 studies (type of study not mentioned) | Not mentioned | Not mentioned | Not mentioned | Not mentioned |
| [ | Acute brain injury | Systematic review | To determine the optimal use and indications of electroencephalography (EEG) in the intensive care management of acute brain injury (ABI). | PubMed (January 1990 through August 15, 2013) | 1979‐2013 | 3 clinical trial studies, 1 case study, 80 prospective observational studies, 78 retrospective studies | Yes | GRADE | No | No |
| [ | The state of the brain during anesthesia | Systematic review & meta‐analysis | Will anesthesia management by processed EEG reduce the rate of unwanted consciousness with recall during anesthesia, postoperative delirium, postoperative neurocognitive disorders, and ultimately, long‐term mortality after surgery, or No. | Ovid MEDLINE/EMBASE/Cochrane Central Register of Controlled Trials/Cochrane Database of Systematic Reviews/PubMed/Web of Science (2000 to October 1, 2018) | 2003‐2019 | 15 clinical trials | Yes | GRADE | Yes | Random effect model |
| Author & year | Type of surgery | Type of study | Study objective | Databases | Searching time | Number and type of included studies | Quality assessment | Quality assessment tool | Analysis | The statistical model used in analysis |
|---|---|---|---|---|---|---|---|---|---|---|
| [ | Spine deformity surgery | Structural causality model and meta‐analysis | Improving MEP performance in deformity surgeries considering potential confounders | Embase from inception to January 2019 | 2002–2019 | 21 cohort studies | No | — | Yes | Structural causal model (SCM) |
| [ | Pedicle screw placement | Systematic review & meta‐analysis | To determine the ability and reliability of tEMG technology to identify malpositioned pedicle screws | the US National Library of Medicine, the Web of Science Core Collection database, and the Cochrane Central Register of Controlled Trials for PS studies | 1994–2014 | 26 studies | Yes | the Downs and Black checklist | Yes | In the performed meta‐analysis, sensitivity, specificity, overall, and subgroup ROC AUC were calculated. Publication bias was also assessed through 1‐tailed funnel plots |
| [ | Spinal cord tumor surgery in Iran modular extra modular | Single‐center retrospective cohort and meta‐analysis | Summary of clinical outcomes of IONM in patients with ID‐EM spinal tumors | PubMed, Embase, Web of Science, and Scopus databases January 1980, to September 6, 2018 | 2015–2010 | 5 Retrospective | No | Duval and Tweedie's trim and fill test (publication bias) | Yes | Pooled diagnostic accuracy was assessed with a 95% confidence interval. A random effect model was used to estimate the cumulative diagnostic accuracy. Publication bias was assessed by drawing funnel plots, where the x‐ and y‐axes were the logit of event rates and standard errors of each study, respectively, and Duval and Tweedie's trim and fill test to determine the number of possible missing articles and the diagnostic value of the adjustment. has been used |
| [ | Cervical decompression surgery | Systematic review | Reviewing the evidence related to the use of technology in cervical decompression surgery in the degenerative environment and trying to identify the best‐supported applications | PubMed and MEDLINE databases and Cochrane Central Registry of Controlled Trials (from March to July 2017) | 2017–2004 | 8 [randomized controlled trials (RCTs), case series (CS), retrospective case series (RCS), and prospective cohort studies (PCS)] | Yes | American Academy of Orthopedic Surgeons (AAOS) | No | No |
| [ | Spine surgery | Systematic review & meta‐analysis | Evaluation of IONM in the prevention of spinal cord injuries | MEDLINE (PubMed), Embase, Lilacs, and Cochrane Central Register databases of randomized assays (January 2007 to September 2017) | 2016–2006 | 6 comparative clinical studies | Yes | MINORS | یله | Random effect model |
| [ | Carino‐encephalic surgery, spine surgery, peripheral vascular surgery | Systematic review | Providing some recommendations based on the best available evidence, with study objective to standardize methods to support IONM in reducing the risk of secondary nerve damage in patients undergoing Carino‐encephalic surgery, spine surgery, peripheral vascular surgery | American University of Beirut Medical Center (one document), PubMed Central (four documents), Springer Link (eight documents), OVIDSP (seven documents), Researchgate (two documents), Science Direct (11 documents) and Wiley Online Library (three documents) and Scottish Intercollegiate Guidelines Network (SIGN) systems to establish the level of evidence (LoE) and grade of recommendation (GoR). | 2017–2009 | 1 guideline, 2 systematic review studies, 8 RCT studies, 44 observational studies, and 1 study without specific classification. | Yes | the CEPD and SIGN scales | No | — |
| [ | Surgery of intramedullary spinal tumors | Systematic review & meta‐analysis | Summary and review of reported evidence on the use of IONM of spinal cord tumors | Embase, Medline Epub, Cochrane Central, Web of Science, and Google Scholar from January 2000 to February 2018 | 2018–2005 | 31 studies in qualitative analysis meta‐analysis of 15 studies | Yes | QUADAS II | Yes | Bivariate model |
| [ | Anterior cervical procedures for spondylotic myelopathy | Meta‐analysis | Evaluation of different IONM techniques in anterior cervical procedures | MEDLINE and the Web of Science for studies published up to February 2013 | 2012–1994 | 22 random, cohort and observational studies | No | Yes | ||
| [ | Corrective surgeries for idiopathic scoliosis patients | Meta‐analysis | Evaluation of common warning criteria and diagnostic value of MEP changes in spine surgery | MEDLINE/PubMed database to determine eligible studies published before October 2014 | 2012–1998 | 12 retrospective cohort study | Yes | QUADAS‐2 | Yes | Bivariate model |
| [ | Spine surgery | Meta‐analysis | Evaluation of efficacy (TcMEP) in predicting impending nerve amputation during corrective spine surgery for patients with idiopathic scoliosis (IS) | PubMed/MEDLINE, Web of Science, and EMBASE from 1945 to January 2014 | 2014–1996 | 25 retrospective cohort study | Yes | QUADAS‐2 | Yes | Univariate random effects comparison model |
| [ | Deformity surgery for idiopathic scoliosis | Meta‐analysis | Objectives to determine the sensitivity, specificity, diagnostic Odd ratio, and area under the receiver operating characteristic (ROC) curve of intraoperative SSEP/TcMEP combinations in relation to neurological outcome in patients undergoing idiopathic scoliosis correction surgery. | Pubmed/MEDLINE, Web of Science, and Embase electronic databases from January 1974 through January 2015 | 2015–2007 | 7 studies | Yes | QUADAS‐2 | Yes | Univariate random effects |
| [ | Deformity surgery for idiopathic scoliosis | Meta‐analysis | Determination of diagnostic accuracy (SSEP) to predict postoperative neurological outcome in patients undergoing spinal deformity surgery for correction of adolescent idiopathic scoliosis (AIS). | MEDLINE and World Science databases from January 1950 through January 2014 | 2014–1983 | 15 retrospective cohort and prospective studies | Yes | QUADAS 2 | Yes | Bivariate model |
| [ | Cervical surgery | Systematic review & meta‐analysis | Evaluation of the sensitivity and specificity of neuromonitoring and the risk of neurological damage after anterior cervical spine surgery (ACSS) with and without (ION) | Medline, Embase, Cochrane Reviews, SCOPUS, Web‐of‐Science (Searching Date Not Mentioned) | 2014–1996 | 9 retrospective studies including 26,357 patients | Yes | MINORS | Yes | Comparison of random effects/mixed effect logistic regression to compare the sensitivity and specificity of non‐modal and multimodal ION |
| [ | Spine surgery | Systematic review | Validation review of recommended warning criteria for IONM | MEDLINE, Excerpta Medica data BASE (EMBASE), Cochrane Controlled Trials Registry, Google Scholar Database of Abstracts of Reviews of Effects (DARE), and Cumulative Index to Nursing and Allied Health Literature (CINAHL) databases after 1980. | 52 cohort studies | No | — | — | ||
| [ | Spinal nerve surgery and monitoring | Systematic review | Investigating the evidence that IONM in the subspinal nerve affects the prevalence of postoperative shoulder diseases and the prediction of functional outcomes. | Medline, Scopus and Cochrane databases | 2012–1995 | 3 studies | Yes | — | No | — |
| [ | Intramedullary spinal tumor surgery | Systematic review & meta‐analysis | Evaluation of the diagnostic value of IONM in identifying postoperative injuries in IMSCT | PubMed, MEDLINE December 31, 2015 and June 30, 2016) | 2016–1993 | 15 retrospective cohort studies, 4 prospective cohort studies, and two case‐control studies | Yes | American Academy of Neurology Evidence Classification System | Yes | Bivariate model and random effects |
| [ | Cervical surgery | Systematic review | Reviewing the evidence of the use of norm‐monitoring technology as a diagnostic tool to evaluate nerve function during surgery for cervical spondylotic myelopathy. | National Library of Medicine (from 1996 through 2005) | Not specified | No | No | No | No | |
| [ | Lumbar cervical, and thoracic surgery | Systematic review | Determining the sensitivity and characteristics of neuromonitoring to identify neurological injuries during spine surgery and evaluating the ability of this technique to improve clinical outcomes for patients during procedures. | MEDLINE, EMBASE, and Cochrane Collaborative Library (between 1990 and March 2009) | 2009–1986 | 32 retrospective cohort studies | Yes |
Grading of Recommendations Assessment, Development, and Evaluation (GRADE) criteria | No | No |
| Author | Included studies for meta‐analysis | Overall pooled sample size | INOM modalities | Outcome measurement | The number and type of studies included | Sensitivity | Specificity | Other measures |
|---|---|---|---|---|---|---|---|---|
| [ | 5 | 103 | SSEPs, MEPs, NMJB, free‐running EMG, and EEG |
Sensitivity specificity Positive Predictive Value Negative Predictive Value | 4 + 1 single center cohort | IONM overall pooled diagnostic value: 77.9% (95% CI 62.1%–88.3%), | IONM overall pooled diagnostic value :91.1% (95% CI 82.2%–95.8%), |
Positive Predictive Value: 56.7% (95% CI 27.7%–81.7%), Negative Predictive Value: 95.7% (95% CI 88.5%–98.5%) |
| [ | 15 | 37 | IONM (SEP, MEP, and mIONM. SEP) |
Sensitivity specificity negative Likelihood Ratio Positive Likelihood Ratio Diagnostic Odds Ratio |
31 qualitative analyses 15 studies in quantitative analysis |
MEPs 0.838 [95% CI, 0.703–0.919] SSEP 0.808 [95% CI, 0.679–0.893] MIONM 0.835 [95% CI, 0.695–0.919] |
MEPs: 0.829 [95% CI, 0.536–0.843] SSEP: 0.714 [95% CI, 0.668–0.921] MIONM: 0579 [95% CI, 0.441–0.736] |
MEPs: 4.901 SSEP:2.825 MIONM:2.072
MEPs: 0.195 SSEP:0.269 MIONM:0.276
MEPs: 29.717 SSEP:12.077 MIONM:7.507 |
| [ | 17 | 806 | MEPs, SSEPs, dorsal column mapping, |
Sensitivity pooled sensitivity specificity pooled specificity pooled DOR |
21 qualitative study analysis/17 meta‐analysis study 15 retrospective cohort studies, 4 prospective cohort studies, and two case‐control studies |
MEPs: individual studies range 75% to 99%, pooled: 90% [95% CI, 84%–94%] SSEP individual studies range:70% to 95% Pooled: of 85% (95% CI, 75–91) |
MEPs individual studies range: 27% to 97% pooled: 82% (95% CI, 70%–90%) SSEP: individual studies range:61% to 96% Pooled: 61% to 96% |
Pooled DOR MEPS 55.7 (95% CI, 26.3–119 Pooled DOR SSEP 14.3 (95% CI, 5.47–37.3) MEPS the pooled area under the hsROC curve MEP:91.8% SSEP: 86.3% |
| Author | Publication year | Included studies for meta‐analysis | Overall pooled sample size | INOM modalities | Outcome measurement | The number and Type of studies included | Sensitivity | Specificity | Other measures |
|---|---|---|---|---|---|---|---|---|---|
| Thirumala et al. | 2017 | 12 | 2102 patients with idiopathic scoliosis | TcMEP | Incidence of neurological deficits, sensitivity, specificity | Prospective, or retrospective cohort reviews | 91% [95% CI 34%–100% | 96% [95% CI 92%–98% | Diagnostic odds ratio:250 [95% CI 11–5767] AUV: 0.98. |
| Thirumala et al. | 2016 | 7 | 2,052 patients with idiopathic scoliosis | SSEP and TcMEP | Sensitivity, specificity, and DOR | Pooled: 82.6% (95% CI: 56.7%–94.5%), | Pooled: 94.4% (95% CI: 85.1%–98.0%), |
DOR: 106.16 (95% CI: 24.952 – 451.667), AUC: 0.928, diagnostic odds ratio | |
| Thirumala et al. | 2016 | 15 | 4763 procedures on idiopathic patients | SSEP | Sensitivity and specificity of somatosensory evoked potentials to predict neurological deficits | Prospective, or retrospective cohort reviews | 84%, [95% CI 59%–95%] | Pooled:98%, [95%CI 97%–99%] |
Diagnostic odds ratio: 340 (95% Cl 125–926) AUC: 0.0.99 |
| Holdefer, R. N. | 2020 | 21 | 5055 spine deformity surgeries. | MEPs, or MEPs and SEPs | Probability of a MEP deterioration which recovered by the end of the surgery, P(RSC), and the conditional probability of no new postoperative deficit given an RSC, P(NND | RSC), stratified by category of an intraoperative adverse event associated with the MEP deterioration | Cohort | — | — |
Probability of no new motor deficit, P(NND): ( P(RSC) for an alert associated with correction: 0.76 for osteotomies (0.48, for hypotension (0.92, P(NND | RSC) for correction: 0.94 for positioning:(0.82) for osteotomies: (0.86) for hypotension:(1.0) odds predictor of no new motor deficits 25.2, |
- —The authors received no specific funding for this work.
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMeningioma and schwannoma management · Intraoperative Neuromonitoring and Anesthetic Effects · Cardiac, Anesthesia and Surgical Outcomes
Introduction
1
Intraoperative neurophysiological monitoring (IONM) has become a crucial component in numerous surgical procedures since the commercial development of IONM devices in the early 1980s. Technological advancements in the past 15 years have led to the evolution of monitoring techniques, expanding its potential applications and increasing its popularity [1]. IONM involves the use of neurophysiological recording techniques to detect changes in the functional state of nerve tissues during surgery, with the underlying principle being that electrical activity changes occur before permanent nerve damage occurs [2].
Research has demonstrated that IONM provides important surgical support by identifying neural structures and reducing the risk of permanent nerve damage during surgery, thus improving patient safety. Various methods are employed in IONM, each with its own specific application [2, 3]. These techniques have been found to significantly reduce postoperative injuries without introducing additional risks, ultimately reducing healthcare costs. Evidence has shown that IONM utilizes a range of techniques, such as evoked motor potentials (MEPs), sensory evoked potentials (SSEPs), electroencephalography (EEG), electromyography (EMG), auditory evoked potentials (AEP), and vision evoked potentials (VEPs), to prevent and minimize damage to the patient's nervous system, while also aiding surgeons and anesthesiologist [1, 4, 5, 6, 7, 8]. IONM techniques are widely used in spinal surgery, certain brain surgeries, carotid endarterectomy, aortic aneurysms, ENT surgeries such as acoustic neuroma (vestibular schwannoma), parotidectomy, and nerve surgeries [9].
In recent years, several systematic reviews and meta‐analyses evaluating the safety and cost‐effectiveness of IONM have been published [10, 11, 12, 13, 14]. However, discrepancies in the conclusions of these studies have created confusion surrounding clinical decision‐making and the appropriate policies related to IONM. While systematic reviews and meta‐analyses are considered the best evidence for evaluating treatment effectiveness and developing clinical guidelines, only high‐quality systematic reviews should be utilized as the basis for making decisions. Unfortunately, there is currently no comprehensive overview of the effects of IONM in various surgeries, further emphasizing the need for further research.
A study by Ney et al. demonstrated that the use of IONM in spinal procedures reduces the relative risk of neurological complications by 49% and estimated the cost of preventing a nerve injury to be 63,387 [[10](#hsr271370-bib-0010)]. In contrast, Traynelis et al. found that using IONM did not lead to significant cost savings exceeding 1 million [15]. Wang et al.'s economic evaluation study concluded that IONM is cost‐effective for preventing permanent recurrent laryngeal nerve (RLN) injuries [16], while Sanabria et al.'s study indicated that routine use of IONM in thyroidectomy with low risk of recurrent laryngeal nerve injury is not cost‐effective in the Colombian health system [17]. Given the discrepancies in results, potential biases in studies, and the increasing use of IONM as a potential standard of care, particularly in thyroid surgeries, there is a critical need for a systematic review evaluating the safety and effectiveness of this technology in various surgeries [13, 18]. Furthermore, evaluating the quality of studies is of utmost importance.
Therefore, the present study aims to review the safety and effectiveness evidence of intraoperative neuromonitoring technology across various surgical procedures, while also assessing the quality of the studies.
Methods
2
We conducted and reported an umbrella review on intraoperative neuromonitoring technology, focusing on its safety and clinical efficacy following the guidelines outlined in the book “A Systematic Review to Support Evidence‐Based Medicine” and the principles of the PRISMA statement [19, 20].
Information Sources
2.1
To collect the necessary data for this study, we conducted searches in various databases including PubMed, Scopus, Web of Science Core Collection, Embase, Cochrane Reviews, and Google Scholar without any time restrictions. We also employed specific search strategies for each database, utilizing a combination of relevant keywords and medical subject headings (MeSH). Additionally, we recorded all extracted studies in Endnote (version X8; Thomson Reuters). The final search for this study was performed on February 6, 2021. The search strategies for each database are presented in Table 1.
Eligibility Criteria
2.2
Population: Patients undergoing spinal surgery, brain surgeries, carotid endarterectomy, aortic aneurysm repair, ENT surgeries (e.g., acoustic neuroma, parotidectomy), and neurosurgery.
Intervention and comparator: Studies comparing neuromonitoring technology with visual nerve identification or studies not utilizing the technology to diagnose and prevent nerve damage.
Type of outcomes: Studies reporting at least one or more of the following outcomes:
- Clinical effectiveness and safety.
- Reduction in the risk of injury and neurological complications during surgery.
- Diagnostic accuracy (sensitivity and specificity).
Type of studies: Systematic reviews and meta‐analyses.
Linguistic limitations: Only full‐text studies in English were included.
Exclusion Criteria
2.3
We excluded review studies, editorials, letters to editors, abstracts, unpublished gray texts such as dissertations and theses, and animal studies. Studies published in languages other than English were also excluded. Additionally, duplicate studies that reported the same results in multiple articles were excluded.
Review Process
2.4
After collecting the extracted articles and removing duplicates, we reviewed the titles of all articles and excluded those that did not align with the objectives of the study. Next, we screened the abstracts and full‐texts of the articles, excluding those that did not meet the inclusion criteria and had little relevance to the study objectives. The reasons for exclusion were documented. The entire systematic review process was conducted independently by two authors of the study, and any disagreements between them were resolved by involving a third party.
Quality Assessment
2.5
We utilized the JBI Critical Appraisal Checklist for Systematic Reviews and Research Syntheses to assess the quality of included systematic review and meta‐analysis studies [20]. This tool, which includes 11 questions and four answer options (YES, No, Unclear, Not applicable) for each question, was used to assess the risk of bias. Two authors of the study independently performed the quality assessment of the included studies, with any discrepancies being resolved by a third party.
Data Extraction
2.6
We entered the extracted data into a form and data table specifically developed for this study. To ensure the adequacy and effectiveness of this form, we piloted it using data from five articles. The form included the following information: authors' names, publication year, study type (systematic review/meta‐analysis), searched databases, time range of included studies, patient population, treatment indication, number and type of included studies, quality assessment, quality assessment tools, statistical models for meta‐analysis, and outcomes (e.g., risk/odds ratio). Two authors of the study independently performed data extraction for each included study, with supervision from a third party.
Data Analysis
2.7
Due to significant heterogeneity among the included studies in terms of design and statistical cut off, no data reanalysis (i.e., meta‐analysis) was conducted. Instead, we employed a narrative synthesis of the findings based on JBI recommendations for umbrella reviews [20]. The findings were organized in descriptive tables, which included key characteristics of the methodology and key findings.
Results
3
Overview of Included Studies
3.1
A total of 726 studies were extracted from databases and other sources. After removing duplicates, 349 articles remained. Subsequently, 60 studies were screened and 12 articles were excluded based on the inclusion/exclusion criteria. Ultimately, 48 studies were included in the analysis of this study (Figure 1).
Flow diagram of the searches and inclusion process.
Figure 2 provides an overview of the included studies that used intraoperative neuromonitoring (IONM) in various surgeries. These surgeries include thyroidectomy (n = 15) [13, 14, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33], aneurysm surgery (n = 5) [9, 34, 35, 36, 37], carotid endarterectomy (n = 3) [38, 39, 40], glioma surgery (n = 2) [41, 42], facial nerve surgery (n = 1) [43], thoracic/cardiac/noncardiac surgeries (n = 1) [44], monitoring of brain status during anesthesia [45], acute brain injury (ABI) (n = 1) [46], foster posterior surgery (n = 1) [43] and spinal surgery (n = 18) [40, 47, 48, 49, 50, 51, 52, 53, 54, 55, 56, 57, 58, 59, 60, 61, 62, 63].
An overview of the included studies in terms of using IONM in various surgeries.
Quality Assessment of Studies
3.2
Figure 3 presents the results of the quality assessment of the included studies. The findings indicate that while the studies were properly designed and collected appropriate data, most of them were found to be weak in terms of three criteria: independent quality assessment conducted by multiple judges, evaluation of publication bias, and provision of policy and practical recommendations (Appendix 1).
Results of quality assessment.
Effectiveness of IONM in Different Surgeries
3.3
Thyroid Surgery (Thyroidectomy)
3.3.1
Fifteen studies on thyroidectomy were published between 2011 and 2019 [13, 14, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33]. Among these studies, five reported statistically significant results in favor of using IONM for temporary recurrent laryngeal nerve paralysis [14, 25, 30, 31, 32], while only two studies demonstrated significant results for permanent paralysis [24, 30]. Other studies did not show statistically significant results for these indicators [13, 23, 26, 29, 33] (Table 2 and Appendix 2).
Cerebral Aneurysm Surgery, Thoracoabdominal, and Aortic Aneurysm Surgery (DTA and TAAAR)
3.3.2
Studies conducted between 2015 and 2020 indicated that using IONM in these surgeries influenced outcomes such as the incidence of new neurological defects, diagnosis, clinical attacks like delayed cerebral ischemia, mortality, morbidity, and prognosis of postoperative neurological defects [9, 34, 35, 36, 37]. However, there is no consensus on the use of motor evoked potentials (MEPs), and current evidence does not strongly support their use. Nonetheless, using MEPs during DTA and TAAAR is considered safe with minimal side effects [9] (Table 3 and Appendix 3).
Carotid Endarterectomy
3.3.3
Results from studies conducted between 2015 and 2018 revealed that the outcomes of using IONM in carotid endarterectomy include sensitivity, diagnostic risk ratio [39, 64], stroke risk prediction [38], and the potential of changes in somatosensory evoked potentials (SSEP) to predict stroke in the 30‐day postoperative period [38]. Multimodal monitoring with changes in electroencephalography (EEG) or SSEP as warning criteria showed higher sensitivity compared to EEG or SSEP alone [39]. EEG monitoring was found to be a strong predictor of strokes in carotid endarterectomy (Table 4).
Glioma Surgery
3.3.4
Two studies conducted in 2015 and 2020 on glioma surgery assessed clinical outcomes such as postoperative complications, functional status, survival without disease progression, and extent of resection (EOR) [41, 42]. One study reported that the rate of primary postoperative failure after awake surgery with DES was higher than general anesthesia. However, the rate of persistent postoperative failure was lower in the awake DES subgroup. Also, no significant relationship was observed among the rate of postoperative failure, NIOM, intraoperative navigation, year of the study, and tumor histology [41].
Observational studies evaluating IONM in glioma surgery have shown an improvement in EOR for both low‐ and high‐grade glioma (Table 5). Results of the only controlled prospective study showed that in IONM‐assisted surgery, the level of EOR for tumors in eloquent areas was not significantly different from the EOR for tumors in non‐eloquent areas. Overall, results confirmed that there was no reliable evidence regarding the use of IONM in glioma surgery [42].
Facial Nerve (FN) Surgery
3.3.5
There is limited evidence regarding the use of IONM in FN surgery. While IONM may improve surgical outcomes by reducing morbidity, there is a lack of randomized controlled trials in this area. The lack of standardization in electrode assembly and excitation parameters prevents definitive conclusions about the best method. Additionally, studies comparing different criteria or multimodal monitoring and their impact on FN anatomical and functional preservation are lacking [43] (Appendixes 4, 5, and Table 2).
Chest/Cardiac/Noncardiac Surgeries
3.3.6
Studies in this area focused on outcomes such as unwanted alertness during anesthesia, postoperative delirium, postoperative neurological disorders, and long‐term mortality. Anesthesia with bispectral index (BIS) or AEP was associated with a significant reduction in the risk of postoperative delirium and long‐term cognitive decline [44].
Monitoring Brain Status During Anesthesia, Acute Brain Injury (ABI)
3.3.7
IONM in these surgeries aims to manage anesthesia using processed EEG and its impact on unwanted consciousness, postoperative delirium, postoperative neurological disorders, and long‐term mortality. Results showed that BIS‐based anesthesia reduced the risk of consciousness when intravenous anesthesia was used. The depth of anesthesia based on EEG monitoring had no effect on long‐term mortality. EEG should be considered in patients with ABI and unexplained persistent altered consciousness or coma in the ICU without acute cerebral complications [45].
Posterior Fossa Surgery
3.3.8
The focus of studies in this area was on the neural circuits involved in Cerebellar mutism syndrome. Comparison of preoperative and postoperative transcranial magnetic stimulation of the cerebellum may predict the onset of CM syndrome. However, there is limited data on neurophysiology during cerebellar surgery, presenting an opportunity for further research and hypothesis testing using IONM [65] (Appendixes 4, 5, and Table 6).
Spinal Surgery
3.3.9
Studies conducted between 2006 and 2020 in the field of spinal surgery examined the diagnostic value and therapeutic neuromonitoring techniques. Diagnostic evaluations focused on indicators such as sensitivity, specificity, true positive, false positive, true negative, false negative, and diagnostic odds ratio. Therapeutic evaluations assessed the risk of surgery‐related neurological damage and impairment, using indicators such as incidence rate and odds ratio. The majority of studies investigated deformity correction [40, 50, 51, 56, 66], removal of spinal cord tumors [47, 48, 49] and cervical surgery [53, 54, 55, 57, 59, 62, 63]. Also, some studies have extended the scope of review and meta‐analysis to spinal surgery in general [54, 58, 59, 60, 61, 63]. An appropriate warning criterion is challenging to define [61], and the clinical value of neuromonitoring remains uncertain [59] (Appendixes 6, 7, and Table 7).
Discussion
4
The objective of this study was to assess the safety and clinical efficacy of intraoperative neuromonitoring (IONM) in various surgical procedures. Over the years, the use of neuromonitoring technology to prevent and minimize surgery‐related injuries and neurological complications has increased. This study reviewed 15 systematic review and meta‐analysis studies on the application of IONM in thyroidectomy. However, due to the heterogeneity among these studies, there were inconsistencies in the results.
Overall, the results of these studies showed that IONM was clinically effective in reducing the risk of temporary RLN paralysis and the overall risk of RLN paralysis after thyroidectomy. However, there was no advantage in reducing the risk of definitive RLN paralysis after thyroidectomy. The findings of this study also indicated that IONM had advantages in reoperations and high‐risk patients. It facilitated the diagnosis of RLN and External Branch of the Superior Laryngeal Nerve (EBSLN), confirmed their functional integrity, identified the site of nerve damage, and provided functional feedback postoperatively. IONM was also successful in reducing bilateral laryngeal paralysis by improving immunity in patients undergoing surgery [67].
Additionally, the results of studies demonstrated that IONM was a reliable tool for anatomical identification and functional monitoring of laryngeal nerve branches. It also had psychological effects on patients, increasing satisfaction and trust in physicians, which in turn affected the success of the surgery. However, one major challenge of using IONM was the need for significant training. Conventional laryngeal nerve detection techniques should not be abandoned, as IONM may not always be available and its cost requires careful evaluation [68]. Further prospective randomized studies are needed to confidently generalize the effectiveness and cost‐effectiveness of IONM.
The results of five systematic review and meta‐analysis studies on the use of IONM in cerebral aneurysm surgery showed that it led to fewer neurological defects during surgery, but there was no statistically significant difference in long‐term follow‐up between the neuromonitoring and control groups. While there is no consensus on the usefulness of IONM in cerebral aneurysms, the studies confirmed that neuromonitoring during motor evoked potentials (MEPs) was a safe procedure with few side effects.
Another important factor in using IONM in patients who have undergone carotid endarterectomy is that they are more likely to have a stroke within 24 h before and 30 days after surgery due to SSEP changes. Also, results showed that an increase in the predicted risk of stroke was associated with drastic changes in SSEP [38, 41]. Therefore, the absence of SSEP compared to changes in SSEP will lead to a higher risk of stroke after surgery; and in general, continuous changes in SSEP than transient changes in SSEP indicates a higher risk of stroke after surgery. However, these findings were more significant when the analyses were considered for two periods of 24 h after and before the surgery. This may also indicate the need for varying degrees of perfusion. However, these results have been expressed while heterogeneity has been high in the studies (I ^2^ > 20%) [39]. Reasons for heterogeneity in these studies included nonuniform reporting of outcome data, differences in follow‐up periods, and differences in area details and severity of stroke due to different protocols and standards. Therefore, the interpretation and generalization of the results of these studies should be taken cautiously [38]. Also, in terms of sensitivity of IONM in carotid endarterectomy surgery, simultaneous changes of both EEG or SSEP methods as warning criteria were more sensitive than EEG and SSEP alone. EEG monitoring has a high sensitivity in predicting stroke during surgery (perioperative stroke). Despite the qualitative evaluation of studies using the QUADAS‐2 tool, there have been limitations such as diffusion bias, differences in study design, bias in data collection and interpretation, and methodological differences between the studies [39, 64].
There is currently no reliable evidence on the use of IONM in glioma surgery. In a meta‐analysis study conducted in 2020, there was no significant relationship between the rate of postoperative failure and the amount of intraoperative neurophysiological monitoring. Also, in IONM‐assisted surgeries, the level of EOR for tumors in eloquent areas was not significantly different from EOR for tumors in non‐eloquent areas [41, 42]. In facial nerve surgery, intraoperative neuromonitoring may improve surgical outcomes, but there is a lack of randomized controlled trials and studies comparing different monitoring criteria [43].
In cardiac/noncardiac/thoracic surgeries, BIS or AEP anesthesia was found to reduce the risk of postoperative delirium and long‐term cognitive decline. To reduce the risk of POD, there is no difference between the ability of anesthesia with BIS and AEP. In addition, there was significant heterogeneity between studies in patients undergoing heart and chest surgery; however, no heterogeneity was observed in patients undergoing noncardiac surgery [44]. On the management of anesthesia by processed EEG and its effect on the level of unwanted consciousness with reminders during anesthesia, postoperative delirium, postoperative neurological disorders, and long‐term postoperative mortality, findings of reviewed studies showed that BIS‐based anesthesia does not reduce the risk of consciousness; however, BIS‐based anesthesia significantly reduces the risk of consciousness in patients receiving intravenous anesthesia. EEG or BIS monitoring reduced the risk of delirium, but there was significant heterogeneity (I ^2^ = 70.8%). Also, there was a significant increase in the risk of postoperative neurological disorders with BIS monitoring. Deep and light anesthesia based on EEG monitoring had no effect on long‐term mortality; also, significant heterogeneity was observed in studies [45]. Regarding the role of IONM in ABI, results showed that EEG should be unexplained and persistent in all patients with ABI and altered consciousness, as well as in patients with intensive care (ICU) coma without the acute brain complication. Also, more studies are needed in this field [46]. Additional studies are needed to evaluate the role of IONM in ABI, posterior fossa surgery, and spinal surgery [65].
In spinal surgery, MEP was found to be more sensitive and specific than SSEP in detecting nerve damage. Combined use of MEP and SSEP provided more valuable information compared to individual use. However, there were differing opinions on the optimal use of these technologies. For example, results of Azad et al.'s study showed that patients with MEP changes were 56 times more likely to have postoperative defects [49]. Also, the efficiency of single and combined use of MEP and SSEP was examined in other studies. For example, Thirumala et al. Fehlings et al. and Di Martino et al. reported the advantages of combined use of MEP and SSEP compared to the use of these technologies individually as a valid diagnostic tool in measuring nerve damage [51, 54, 55]. However, Ajiboye et al. reported that using the technology individually has a better effect compared to combined use [52]. Also, Rijs et al. suggested that large prospective studies are needed to gain more knowledge about the value of combined use of MEP and SSEP [48].
Overall, neuromonitoring technologies were found to be useful in identifying nerve damage in various surgical procedures. However, due to heterogeneity and lack of strong clinical evidence, further research is needed to accurately determine the clinical value of neuromonitoring and define appropriate warning criteria [59].
Limitations
5
The limitations of this study include the lack of strong evidence and the nonrandom nature of the included studies, which limit the generalizability of the conclusions. The challenges surrounding the use of neuromonitoring technology also pose limitations [59, 61]. Additionally, the quality of the included studies in the meta‐analyses was not evaluated, and the reliance on existing meta‐analyses rather than original data studies may impact the conclusions. The possibility of overlap between the studies included in the meta‐analyses was not examined, which could affect the results. The qualitative synthesis of the study results also makes it difficult to establish a causative relationship. Furthermore, the lack of sufficient evidence in some surgeries makes it challenging to draw conclusions about the effectiveness of IONM.
Conclusion
6
In conclusion, further prospective studies, large randomized controlled trials, and economic evaluation studies are needed to definitively assess the effectiveness and safety of IONM. The heterogeneity in study types and thresholds for warning criteria, as well as the uncertain benefits of preventing new neurological defects, necessitate further research in this area.
Author Contributions
Aziz Rezapour: conceptualization, methodology, writing – original draft, supervision, project administration. Naser Derakhshani: conceptualization, writing – review and editing, methodology, data curation; resources. Seyedeh Narges Pouyan: writing – original draft, writing – review and editing; visualization. Vahid Alipour: writing – original draft, methodology, resources, data curation. Seyed Jafar Ehsanzadeh: writing – original draft, writing – review and editing, data curation. Arash Zare‐Sadeghi: conceptualization, methodology, data curation, resources. Jalal Arabloo: conceptualization, writing – original draft, writing – review and editing, methodology, project administration, data curation.
Ethics Statement
The study was approved by the Ethics Committee of the Iran University of Medical Sciences (IR.IUMS.REC.1399.1233). Consent forms was not applicable for this study. The article does not require any human/animal subjects to acquire such approval.
Consent
The authors have nothing to report.
Conflicts of Interest
The authors declare no conflicts of interest.
Transparency Statement
The lead author Jalal Arabloo affirms that this manuscript is an honest, accurate, and transparent account of the study being reported; that no important aspects of the study have been omitted; and that any discrepancies from the study as planned (and, if relevant, registered) have been explained.
Supporting information
appendix file 1.
appendix file 2.
appendix file 3.
appendix file 4.
appendix file 5.
appendix file 6.
appendix file 7.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1S.‐M. Kim , S. H. Kim , D.‐W. Seo , and K.‐W. Lee , “Intraoperative Neurophysiologic Monitoring: Basic Principles and Recent Update,” Journal of Korean Medical Science 28, no. 9 (2013): 1261–1269.24015028 10.3346/jkms.2013.28.9.1261 PMC 3763097 · doi ↗ · pubmed ↗
- 2N. A. Shlobin , E. Raz , M. Shapiro , et al., “Spinal Neurovascular Complications With Anterior Thoracolumbar Spine Surgery: A Systematic Review and Review of Thoracolumbar Vascular Anatomy,” Neurosurgical Focus 49, no. 3 (2020): E 9.10.3171/2020.6.FOCUS 2037332871559 · doi ↗ · pubmed ↗
- 3M. Eager , A. Shimer , F. R. Jahangiri , F. Shen , and V. Arlet , “Intraoperative Neurophysiological Monitoring (IONM): Lessons Learned From 32 Case Events in 2069 Spine Cases,” American Journal of Electroneurodiagnostic Technology 51, no. 4 (2011): 247–263.22303776 · pubmed ↗
- 4A. Charalampidis , F. Jiang , J. R. F. Wilson , J. H. Badhiwala , D. S. Brodke , and M. G. Fehlings , “The Use of Intraoperative Neurophysiological Monitoring in Spine Surgery,” supplement, Global Spine Journal 10, no. 1S (2020): 104S–114S.31934514 10.1177/2192568219859314 PMC 6947672 · doi ↗ · pubmed ↗
- 5M. R. Weinzierl , P. Reinacher , J. M. Gilsbach , and V. Rohde , “Combined Motor and Somatosensory Evoked Potentials for Intraoperative Monitoring: Intra‐ and Postoperative Data in a Series of 69 Operations,” Neurosurgical Review 30, no. 2 (2007): 109–116.17221265 10.1007/s 10143-006-0061-5 · doi ↗ · pubmed ↗
- 6L. C. Jameson , D. J. Janik , and T. B. Sloan , “Electrophysiologic Monitoring in Neurosurgery,” Anesthesiology clinics 25, no. 3 (2007): 605–630.17884710 10.1016/j.anclin.2007.05.004 · doi ↗ · pubmed ↗
- 7M. A. Sloan , “Prevention of Ischemic Neurologic Injury With Intraoperative Monitoring of Selected Cardiovascular and Cerebrovascular Procedures: Roles of Electroencephalography, Somatosensory Evoked Potentials, Transcranial Doppler, and Near‐Infrared Spectroscopy,” Neurologic Clinics 24, no. 4 (2006): 631–645.16935192 10.1016/j.ncl.2006.05.002 · doi ↗ · pubmed ↗
- 8M. Banoub , J. E. Tetzlaff , and A. Schubert , “Pharmacologic and Physiologic Influences Affecting Sensory Evoked Potentials: Implications for Perioperative Monitoring,” Anesthesiology 99, no. 3 (2003): 716–737.12960558 10.1097/00000542-200309000-00029 · doi ↗ · pubmed ↗