Frequency of Seroconversion in Aquaporin‐4 Antibody Testing: Insights From Real‐World Data
Tatchaporn Ongphichetmetha, Mengke Du, Nisa Vorasoot, Sean J. Pittock, Jeffrey A. Cohen, Amy Kunchok

TL;DR
The study finds that seroconversion to AQP4-IgG is rare after initial negative testing, especially with modern cell-based assays.
Contribution
The study provides real-world data on the low yield of repeat AQP4-IgG testing after initial negative results using modern assays.
Findings
Seroconversion occurred in 4.3% of patients initially tested with tissue IFA.
No seroconversion was observed in patients initially tested with cell-based assays (CBA).
Repeat testing is low yield unless prior testing used older methods like IFA.
Abstract
Clinicians often repeat aquaporin‐4‐immunoglobulin G (AQP4‐IgG) testing in case of possible seroconversion. Compared with older, less sensitive immunofluorescence assays (IFA), cell‐based assays (CBA) offer higher sensitivity. This study assessed the frequency of seroconversion in a retrospective Cleveland Clinic cohort (2006–2024) of 451 patients with an initial negative AQP4‐IgG result who underwent serial testing. Seroconversion occurred in 4.3% (7/170) of patients initially tested by tissue IFA, but in none (0/263) of those tested by CBA. The lack of AQP4‐IgG seroconversion after a negative CBA, with only rare cases after a negative IFA, suggests that repeat AQP4‐IgG testing is low yield unless prior testing used older methods such as IFA.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
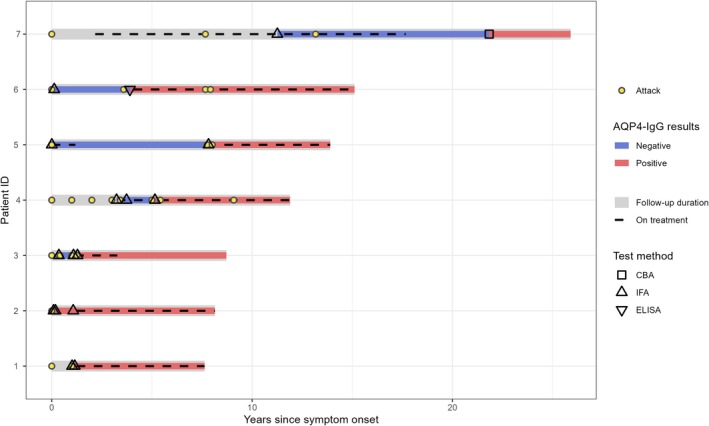 FIGURE 1
FIGURE 1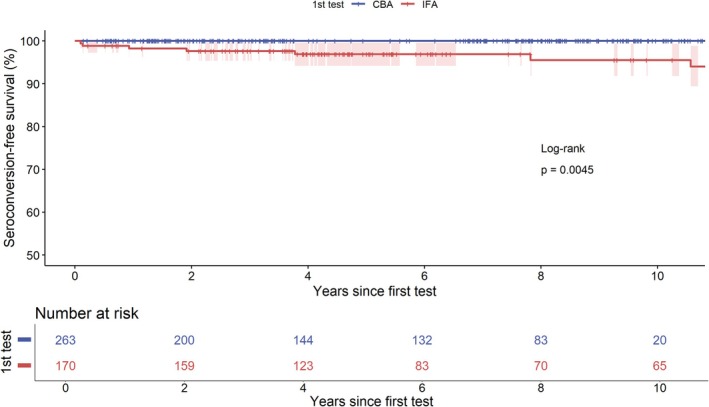 FIGURE 2
FIGURE 2| Characteristic | All patients ( | Seroconverted group ( | Persistently seronegative group ( |
|
|---|---|---|---|---|
| Age at the first test, years | 41.3 (14.5) | 45.8 (12.4) | 41.2 (14.6) | 0.407 |
| Female, | 330 (73.2%) | 7 (100%) | 323 (72.7%) | 0.197 |
| Initial presentation, | ||||
| Optic neuropathy | 143 (31.7%) | 3 (42.9%) | 140 (31.5%) | 0.845 |
| Unilateral optic neuropathy | 127 | 3 | 124 | |
| Bilateral optic neuropathy | 16 | 0 | 16 | |
| Myelopathy | 193 (42.8%) | 3 (42.9%) | 190 (42.8%) | |
| Short segment myelopathy | 130 | 1 | 129 | |
| Long segment myelopathy | 63 | 2 | 61 | |
| Supratentorial syndrome | 38 (8.4%) | 0 (0%) | 38 (8.6%) | |
| Infratentorial syndrome | 36 (8.0%) | 1 (14.2%) | 35 (7.9%) | |
| Optic neuropathy with myelopathy | 5 (1.1%) | 0 (0%) | 5 (1.1%) | |
| Optic neuropathy with infratentorial syndrome | 2 (0.4%) | 0 (0%) | 2 (0.5%) | |
| Others | 34 (7.5%) | 0 (0%) | 34 (7.7%) | |
| Final diagnosis, | ||||
| Multiple sclerosis | 173 (38.4%) | 0 (0%) | 173 (39.0%) | < 0.001 |
| NMOSD | 19 (4.2%) | 7 (100%) | 12 (2.7%) | |
| MOGAD | 12 (2.7%) | 0 (0%) | 12 (2.7%) | |
| ADEM | 5 (1.1%) | 0 (0%) | 5 (1.1%) | |
| Isolated optic neuritis | 57 (12.6%) | 0 (0%) | 57 (12.8%) | |
| Isolated myelitis | 69 (15.3%) | 0 (0%) | 69 (15.5%) | |
| Isolated supratentorial syndrome | 5 (1.1%) | 0 (0%) | 5 (1.1%) | |
| Isolated infratentorial syndrome | 5 (1.1%) | 0 (0%) | 5 (1.1%) | |
| Combined IIDs | 10 (2.2%) | 0 (0%) | 10 (2.3%) | |
| Other inflammatory conditions | 35 (7.8%) | 0 (0%) | 35 (7.9%) | |
| Other noninflammatory conditions | 61 (13.5%) | 0 (0%) | 61 (13.7%) | |
| Total follow‐up time, years | 6.38 (IQR 2.95–9.53, range 0.15–18.46) | 8.7 (IQR 8.2–14.3) | 6.2 (IQR 2.9–9.5) | 0.031 |
| Times of repeated test | 2 (range 2–6) | 2 (IQR 2–3) | 2 (IQR 2–6) | 0.262 |
| Methods of the first test, | ||||
| CBA | 263 (58.3%) | 0 (0%) | 263 (59.2%) | 0.006 |
| IFA | 170 (38.7%) | 7 (100%) | 163 (36.7%) | |
| ELISA | 4 (0.9%) | 0 (0%) | 4 (0.9%) | |
| IFA plus ELISA | 14 (3.1%) | 0 (0%) | 14 (3.2%) | |
| Patient number | Sex | Age at first testing, years | First clinical presentation | Number of tests | Duration after first symptom onset, days | Test results (with titer if available) | Test method | Recent or current immunotherapy | Disease course | Tested ±30 days of symptom onset | Final diagnosis |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | F | 35 | ON | 1 | 908 | Negative | IFA | Azathioprine and prednisolone | Relapsing–remitting (recurrent ON and myelitis) | No | AQP4‐IgG+ NMOSD |
| 2 | 1090 | Negative | IFA | Azathioprine | No | ||||||
| 3 | 1608 | Positive | IFA | None | No | ||||||
| 2 | F | 53 | ON | 1 | 130 | Negative | IFA | None | Relapsing–remitting (recurrent ON and myelitis) | No | AQP4‐IgG+ NMOSD |
| 2 | 397 | Negative | IFA | None | Yes | ||||||
| 3 | 469 | Positive | IFA | Rituximab (last dose 2 weeks prior), recent IVMP, and PLEX (1 month prior) | Yes | ||||||
| 3 | F | 65 | Acute myelitis | 1 | 35 | Negative | IFA | IVMP (1 dose) | Monophasic | No | AQP4‐IgG+ NMOSD |
| 2 | 70 | Positive | IFA | Recent IVMP (1 week prior) | No | ||||||
| 3 | 393 | Positive | IFA | None | No | ||||||
| 4 | F | 46 | Acute myelitis | 1 | 27 | Negative | IFA | None | Relapsing–remitting (recurrent ON and myelitis) | Yes | AQP4‐IgG+ NMOSD |
| 2 | 2884 | Positive (1:40) | IFA | Azathioprine and oral prednisolone | Yes | ||||||
| 5 | F | 38 | ON | 1 | 19 | Negative | IFA | IVMP (3 doses) | Relapsing–remitting (recurrent ON) | No | AQP4‐IgG+ NMOSD |
| 2 | 1399 | Positive (22.8) | IFA + ELISA | Recent IVMP | No | ||||||
| 6 | F | 52 | ON | 1 | 4113 | Negative | IFA | Azathioprine | Relapsing–remitting (recurrent ON and myelitis) | No | AQP4‐IgG+ NMOSD |
| 2 | 7975 | Positive (1:100) | CBA (fixed) | None | No | ||||||
| 7 | F | 29 | Acute brainstem syndrome | 1 | 24 | Negative | IFA | None | Relapsing–remitting (recurrent brainstem syndrome) | Yes | AQP4‐IgG+ NMOSD |
| 2 | 71 | Positive (1:20) | IFA | Recent IVMP (1 month prior) with prednisolone | No |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSingle-cell and spatial transcriptomics · Cystic Fibrosis Research Advances · Myasthenia Gravis and Thymoma
Introduction
1
The frequency of aquaporin‐4 immunoglobulin G (AQP4‐IgG) seroconversion (negative to positive) in clinical practice is not well understood. Despite this, clinicians often retest seronegative patients out of concern for potential seroconversion, which may add cost and inconvenience for patients. In a laboratory cohort, seroconversion occurred in 0.6% of patients who underwent ≥ 2 AQP4‐IgG tests using cell‐based assay (CBA) methods [1]. This study had a large sample size but limited clinical data and did not examine older test methods. Early AQP4‐IgG testing was done using tissue‐based indirect immunofluorescence assays (IFA), which have low sensitivity (40%–65%) [2, 3, 4, 5]. Later, enzyme‐linked immunosorbent assays (ELISA) offered higher sensitivity (50%–94%) but lower specificity [6]. Currently, the gold standard is CBA, with highest sensitivities (> 85%) reported for live compared with fixed CBA [3, 7].
There are a few studies of seroconversion in clinical cohorts with small sample sizes. A prospective neuromyelitis optica spectrum disorder (NMOSD) cohort study reported a 20.8% (5/24) seroconversion rate [8], while another found 59% (13/22) [9]. We hypothesize that this variation may stem from differences in historical testing methods, including lower‐sensitivity older methods. Other factors influencing false negatives may include the timing relative to disease onset, prior treatments such as immunosuppressive therapies, plasma exchange, or high‐dose steroids, which may reduce titers to undetectable levels [1, 10].
This study aimed to assess the frequency of AQP4‐IgG seroconversion in a large clinical cohort of patients with a suspicion of NMOSD or other central nervous system inflammatory demyelinating diseases, using multiple testing methods.
Methods
2
Study Participants and Design
2.1
This retrospective cohort study included all patients with ≥ 2 serum AQP4‐IgG tests using various methods and clinical data identified from the Cleveland Clinic electronic records between 2006 and 2024. Patients with a negative result on their first serum AQP4‐IgG test were included. The clinical indication for AQP4‐IgG testing could not be determined retrospectively in all patients; however, at our institution, AQP4‐IgG testing is ordered almost exclusively by neurologists for patients with suspected demyelinating disease.
AQP4‐IgG Testing
2.2
Serum was tested by several methods: (1) CBA; (2) IFA; (3) ELISA; and (4) screening with IFA followed by confirmation with ELISA, with positivity reported only when both tests were positive. Seroconversion was defined as a change in serum AQP4‐IgG status from negative to positive. The last available test result was considered final.
In this study, approximately 78% of AQP4‐IgG tests were performed at Mayo Clinic, 20% at Associated Regional and University Pathologists (ARUP), and 2% at Quest and LabCorp combined. Mayo Clinic testing has evolved from earlier methods like IFA and ELISA to live CBA by Fluorescence‐Activated Cell Sorting (FACS) since 2016, with IFA no longer used in isolation. Other laboratories previously used ELISA, and many currently use fixed CBA. Since 2020, all AQP4‐IgG testing ordered at Cleveland Clinic has been completed at Mayo Clinic by live CBA. Including all historical testing methods allowed us to assess seroconversion rates across assays and reflect real‐world clinical practice.
Statistical Analyses
2.3
Kaplan–Meier curves examined the probability of seroconversion during the follow‐up period, and the log‐rank test compared the probability of survival based on the initial assay (CBA versus IFA). Differences in clinical and laboratory data between patients with and without seroconversion were analyzed using the bootstrap test or Fisher's exact test, as appropriate. Analyses were performed in R version 4.4.2 [11].
Results
3
A total of 451 individuals with ≥ 2 serum AQP4‐IgG tests, whose first test was negative, were included (Figure S1). The mean age was 41 years (standard deviation, SD = 15), and 330 (73%) were female. The median clinical follow‐up period was 6.4 years (interquartile range, IQR 2.95–9.53). The median serological follow‐up period was 1.4 years (IQR 0.45–4.75). The first negative test was performed by CBA in 263 (58.3%) individuals, IFA in 170 (38.7%), ELISA in 4 (0.9%), and both IFA and ELISA in 14 (3.1%) (Table 1). The median number of AQP4‐IgG tests per patient was 2 (range 2–6). Of the 451 individuals, 377 (84%) had 2 tests, and 74 (16%) had ≥ 3 tests.
Seroconversion
3.1
Seroconversion by any test type was identified in 7/451 (1.6%) of individuals. After excluding patients tested for very low probability clinical presentations (e.g., dizziness), the seroconversion rate was 7/417 (1.7%). The probability of seroconversion was significantly greater in patients initially tested by IFA 7/170 (4.3%) compared to those initially tested by CBA (0/263 [0%]) (p = 0.0045).
All seven seroconverted patients were initially tested by IFA before 2018, and five returned positive on their second test (3 by IFA, 1 by IFA plus ELISA, and 1 by CBA). Two patients had a negative second IFA test, followed by a positive third IFA test (Figure 1, Table 2).
Temporal course of AQP4‐IgG seroconverters: tests, attacks, and therapies. Abbreviations: AQP4‐IgG, aquaporin‐4 immunoglobulin G; CBA, cell‐based assays; ELISA, enzyme‐linked immunosorbent assays; IFA, tissue‐based indirect immunofluorescence assays.
Clinical Features of Seroconverters
3.2
The mean age of these seven patients was 46 years (SD = 12), and all were female. Of the seven seroconverted individuals, four fulfilled the 2015 Diagnostic Criteria for seronegative NMOSD without AQP4‐IgG (prior to seroconversion) (Figure 1, Table 2). Four patients received immunosuppressants prior to the first negative test, including azathioprine (two patients) and intravenous methylprednisolone (two patients).
Seroconversion was most common in patients presenting with myelitis and/or optic neuritis (6/7 [86%]). No patients with a clinical diagnosis of multiple sclerosis (MS) or acute disseminated encephalomyelitis (ADEM) seroconverted to positive. Seroconversion during an attack was observed in two patients. The median time from the first AQP4‐IgG test to seroconversion was 23.3 months (IQR 6.5–70.6) (Figure 2).
Time to AQP4‐IgG seroconversion after initial negative test with either CBA or IFA. Abbreviations: CBA, cell‐based assays; IFA, tissue‐based indirect immunofluorescence assays.
Discussion
4
In this clinical cohort, AQP4‐IgG seroconversion occurred in 4.3% (7/170) of patients initially tested by IFA, but in 0/263 patients initially tested by CBA. No patient seroconverted after a negative CBA, similar to prior laboratory data (0.6% rate) [1]. These findings suggest that repeat testing is low yield after a negative CBA, but may be warranted for patients previously tested with older assays such as IFA.
The sensitivity of the initial AQP4‐IgG testing method may impact AQP4‐IgG seroconversion. All seven seroconverters were initially tested by IFA (4% of those first tested by IFA). This suggests that the initial negative results could have been false negatives due to the limited sensitivity of IFA. As several studies have reported the low sensitivity of serum AQP4‐IgG testing by IFA [2, 3, 4, 5, 12], patients with an initial IFA test and high clinical suspicion should be considered for retesting with CBA.
Beyond assay sensitivity, disease activity may influence titers of AQP4‐IgG, though prior studies to date have been conflicting regarding this [10, 13]. We observed that two patients had an attack at the time of their seroconversion. Immunosuppressive treatments have also been postulated to influence titers of AQP4‐IgG [1], and we observed that four seroconverters tested negative while receiving azathioprine and corticosteroids, consistent with other reports [1, 14]. However, the role of immunosuppression on serostatus change is not fully understood.
All patients who seroconverted had core clinical features of NMOSD. No patients with a diagnosis of MS or ADEM seroconverted, highlighting both the specificity of AQP4‐IgG and suggesting the low utility of serially testing patients without NMOSD features.
This study has several limitations. First, the initial and repeat testing were determined by treating physicians and not standardized, so not all patients underwent CBA as the final diagnostic test, potentially missing some seroconversions. The specific type of CBA (live vs. fixed) was not specified for all historical tests, though no patient tested by CBA seroconverted. Additionally, the relatively short median serological follow‐up (1.4 years) may have limited the detection of late seroconversion. Strengths of this study include a median clinical follow‐up exceeding 6 years and the availability of comprehensive clinical data.
No AQP4‐IgG seroconversions occurred after a negative CBA in this clinical cohort. Few seroconversions were seen only in patients initially tested with older, less sensitive IFA. Repeat testing with CBA should therefore be reserved for patients with a high clinical suspicion of NMOSD and a prior negative IFA result, as repeating CBA after an initial negative CBA is likely to be low yield.
Author Contributions
T.O., and A.K., contributed to the conception and design of the manuscript; T.O., M.D., N.V., S.J.P., J.A.C., and A.K. contributed to drafting the manuscript and preparing the figures.
Conflicts of Interest
T.O., M.D., and N.V. have nothing to report. S.J.P. reported personal fees from Alexion/AstraZeneca (all fees paid to Mayo Clinic), personal fees from Horizon/Amgen (all fees paid to Mayo Clinic), and grants from Roche/Genentech (cytokine testing) outside the submitted work; in addition, Dr. Pittock had a patent for 9891219B2, application 12‐573942, “Methods for Treating Neuromyelitis Optica [NMO] by Administration of Eculizumab to an Individual That is Aquaporin‐4 [AQP4]‐IgG Autoantibody Positive” (he has received royalties). J.A.C. has received personal compensation for consulting for Astoria, Bristol‐Myers Squibb, Convelo, and Viatris, and Chairing a DSMB for Celltrion. A.K. has received personal compensation for consulting for EMD Serono and Alexion.
Supporting information
Table S1. Number of repeat tests after the initial negative result, categorized by initial testing method. Figure S1. Study flow diagram.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1M. Majed , C. Valencia Sanchez , J. L. Bennett , et al., “Alterations in Aquaporin‐4‐Ig G Serostatus in 986 Patients: A Laboratory‐Based Longitudinal Analysis,” Annals of Neurology 94, no. 4 (2023): 727–735.37314750 10.1002/ana.26722 PMC 11804127 · doi ↗ · pubmed ↗
- 2K. H. Chan , J. S. Kwan , P. W. Ho , J. W. M. Ho , A. C. Y. Chu , and D. B. Ramsden , “Aquaporin‐4 Autoantibodies in Neuromyelitis Optica Spectrum Disorders: Comparison Between Tissue‐Based and Cell‐Based Indirect Immunofluorescence Assays,” Journal of Neuroinflammation 7 (2010): 50.20822515 10.1186/1742-2094-7-50PMC 2941752 · doi ↗ · pubmed ↗
- 3P. Waters , M. Reindl , A. Saiz , et al., “Multicentre Comparison of a Diagnostic Assay: Aquaporin‐4 Antibodies in Neuromyelitis Optica,” Journal of Neurology, Neurosurgery, and Psychiatry 87, no. 9 (2016): 1005–1015.27113605 10.1136/jnnp-2015-312601 PMC 5013123 · doi ↗ · pubmed ↗
- 4P. J. Waters , A. Mc Keon , M. I. Leite , et al., “Serologic Diagnosis of NMO: A Multicenter Comparison of Aquaporin‐4‐Ig G Assays,” Neurology 78, no. 9 (2012): 665–671, discussion 669.22302543 10.1212/WNL.0b 013e 318248 dec 1PMC 3286228 · doi ↗ · pubmed ↗
- 5K. Prain , M. Woodhall , A. Vincent , et al., “AQP 4 Antibody Assay Sensitivity Comparison in the Era of the 2015 Diagnostic Criteria for NMOSD,” Frontiers in Neurology 10 (2019): 1028.31636597 10.3389/fneur.2019.01028 PMC 6787171 · doi ↗ · pubmed ↗
- 6S. Hayakawa , M. Mori , A. Okuta , et al., “Neuromyelitis Optica and Anti‐Aquaporin‐4 Antibodies Measured by an Enzyme‐Linked Immunosorbent Assay,” Journal of Neuroimmunology 196, no. 1–2 (2008): 181–187.18462810 10.1016/j.jneuroim.2008.03.009 · doi ↗ · pubmed ↗
- 7Y. Said , A. Filippatou , C. Tran , et al., “Real‐World Clinical Experience With Serum MOG and AQP 4 Antibody Testing by Live Versus Fixed Cell‐Based Assay,” Annals of Clinical and Translational Neurology 12 (2025): 556–564.39901660 10.1002/acn 3.52310 PMC 11920744 · doi ↗ · pubmed ↗
- 8X. Zhang , X. Liu , H. Yu , B. Deng , Y. Zhang , and X. Chen , “Longitudinal Evaluation of Clinical Characteristics of Chinese Neuromyelitis Optica Spectrum Disorder Patients With Different AQP 4‐Ig G Serostatus,” Multiple Sclerosis and Related Disorders 62 (2022): 103786.35429818 10.1016/j.msard.2022.103786 · doi ↗ · pubmed ↗