Failure of oral anti-Xa to prevent non-bacterial thrombotic endocarditis in cancer: case report and literature review
Mariam Benjelloun, Edith Jottrand, Emmanuel Joly, Attilio Leone, Philippe Van De Borne

TL;DR
A cancer patient on anticoagulant therapy still developed a rare heart condition called Marantic endocarditis, highlighting challenges in managing blood clots in cancer patients.
Contribution
This case report highlights the limitations of direct oral anticoagulants in preventing thrombotic complications in cancer patients with hypercoagulable states.
Findings
A patient with lung cancer on Rivaroxaban developed Marantic endocarditis and severe blood clots despite anticoagulation.
Switching to low molecular weight heparin temporarily stabilized the patient but could not prevent mortality due to rapid cancer progression.
The case suggests that hypercoagulable states in cancer may not be adequately controlled by direct oral anticoagulants.
Abstract
Marantic endocarditis (ME) is a rare but potentially fatal complication of hypercoagulable states, posing a significant diagnostic challenge in oncology. Timely detection and appropriate treatment are essential to prevent complications and improve clinical outcomes. In neoplastic contexts, tumour cells can activate the coagulation cascade, leading to thromboembolic events that serve as critical warning signs. A multidisciplinary approach is vital for effective management of this condition. A 64-year-old woman, recently diagnosed with non-small cell lung carcinoma, was receiving anticoagulation therapy with Rivaroxaban for right iliac-femoral deep vein thrombosis. She developed progressive symptoms, including visual disturbances and dyspnoea. Magnetic resonance imaging of the brain showed ischaemic lesions in the territory of the right posterior cerebral artery and a pulmonary-CT…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
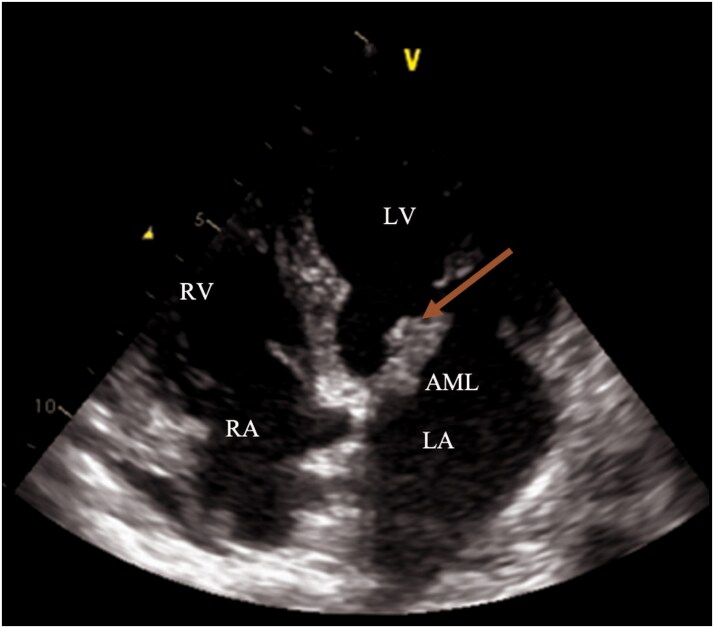 Figure 1
Figure 1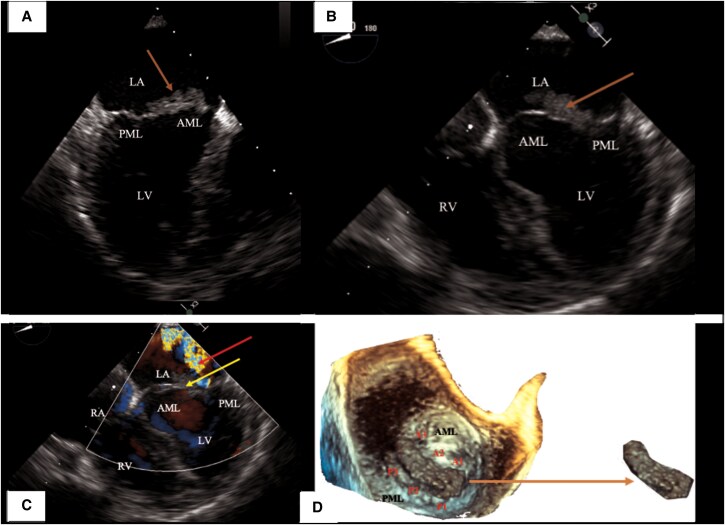 Figure 2
Figure 2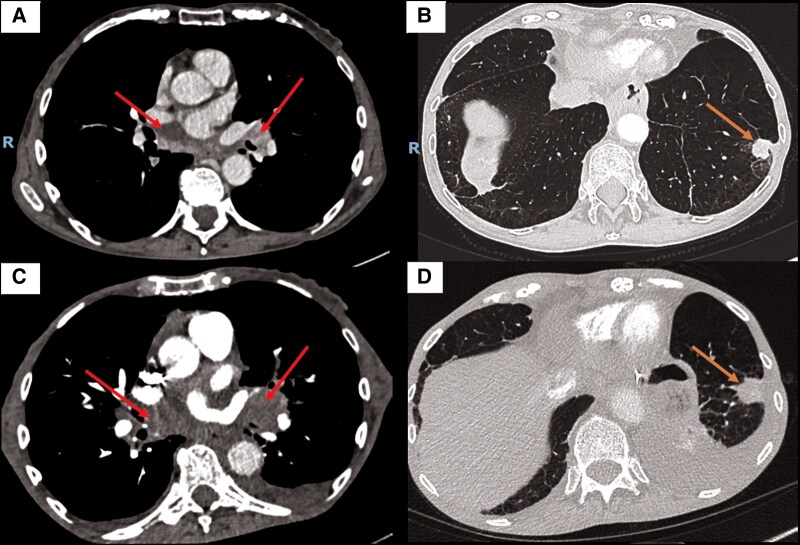 Figure 3
Figure 3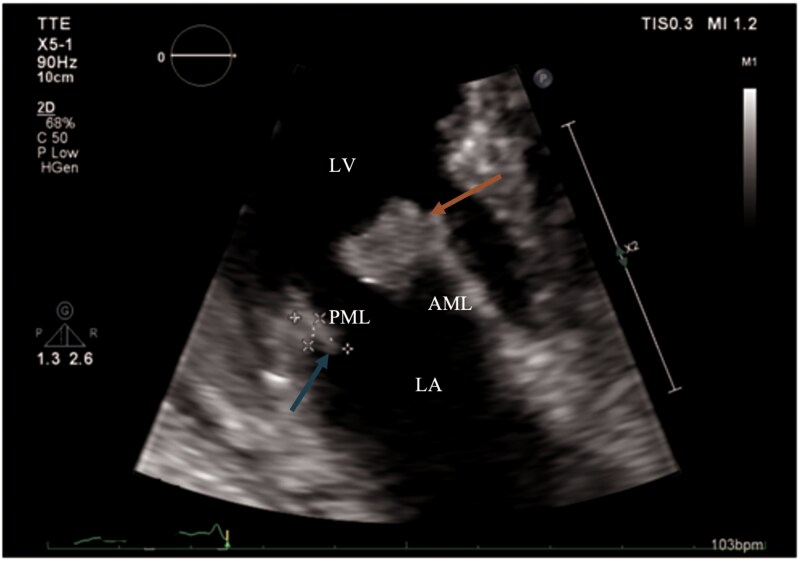 Figure 4
Figure 4| Date | Events |
|---|---|
|
| Right femoral vein thrombosis. Initiation of Rivaroxaban (15 mg twice daily for 21 days, followed by 20 mg once daily). |
|
| Chest angioscanner: Discovery of a spiculated pulmonary nodule in the left lower lobe measuring 23×16 mm with mediastinal and hilar lymphadenopathy. |
|
| Positron Emission Tomography—Computed Tomography (PET-CT) : Revealing the pulmonary lesion with mediastinal and hilar lymphadenopathy. No metastases detected. |
|
| Endobronchial ultrasound (EBUS): Non-small cell carcinoma (NSCLC - TTF1 -; P40 -; PD-L1 + > 50%; EGFR -). No mutations detected in the EGFR gene. No mutations were detected in codon V600 of the BRAF gene. |
|
| Cardio-oncology consultation: Transthoracic echocardiography: Preserved left ventricular ejection fraction (LVEF)—Simpson Bp 60%; no significant valvular disease. |
|
| Pembrolizumab (first cycle) |
|
| Emergency visit: Visual disturbances + dyspnoea. |
|
| Chest CT angiogram: Severe bilateral pulmonary embolism at the segmental level. Stop Rivaroxaban and start low molecular weight heparin. |
|
| Brain MRI: Ischaemic stroke in the territory of the right posterior cerebral artery. |
|
| Transthoracic echocardiogram (TTE): Discovery of a mass extending over the anterior mitral leaflet, measuring 18×7 mm and moderate mitral regurgitation. |
|
| Transoesophageal echocardiogram (TEE): Homogeneous mass extending on the anterior mitral leaflet measuring 21×7 mm associated with moderate mitral regurgitation (SOR 0.25 cm2, VOR 34 mL). |
|
| Heart Team: Diagnosis established: marantic endocarditis in the context of pulmonary neoplasia. |
|
| Chest angioscanner reveals an increase in the left hilar mass, enlargement of the pulmonary nodule, and the presence of multiple embolic images in the third-order branches of the pulmonary arteries bilaterally. |
|
| Follow-up TTE: Further enlargement of the mass extending on the anterior mitral leaflet measuring 18×15 mm + new mass measuring 8.5×4.0 mm on the posterior mitral leaflet. Increased mitral insufficiency. |
|
| Patient's Death At Home Under Palliative Care. |
| Author (year) | Age/sex | Cancer/pathology | Prior treatment (indication) | Initial presentation | Affected valve | Treatment | Outcome |
|---|---|---|---|---|---|---|---|
| F. Pons | Female/65 years | Lung adenocarcinoma (with supraclavicular lymphadenopathy) T1N2M + - no treatment | VKA (DVT) | Stroke | Mitral | UFH, then therapeutic cessation | Deceased |
| F. Pons | Male/63 years | Non-operable lung adenocarcinoma (T1N2M+) treated with radio chemotherapy (cisplatin and Alimta) | VKA (DVT) | NSTEMI, Stroke | Mitral + Aortic | LMWH | Deceased |
| F. Mantovani | Female/65 years | Pancreatic adenocarcinoma | Rivaroxaban (DVT and PE) | Recurrent PE | Mitral + Aortic | UFH then LMWH | Survival |
| Yoshiharu Soga | Male/69 years | Tubular adenocarcinoma of the stomach | Apixaban (DVT) | Stroke | Mitral | UFH then LMWH | Survival |
| Marissa | Female/63 years | Biliary adenocarcinoma | Rivaroxaban (DVT) | Stroke | Mitral + Aortic | Apixaban, then UFH (du to multiple emboli) and then LMWH | Survival |
| Sihan | Male/48 years | antiphospholipid syndrome (APS) | Apixaban (previous PE and DVT after failure of Warfarin and Rivaroxaban) | Stroke | Mitral | UFH + surgical (mitral valve replacement) | Deceased |
| Tosha Hedin | Male/54 years | Oesophageal adenocarcinoma | Rivaroxaban (AF) | – | Mitral | LMWH | Survival |
| Amit K. Mandal | Male/37 years | Antiphospholipid syndrome (APS) | Rivaroxaban (APS—initially on Warfarin) | Heart failure | Mitral + Aortic | VKA | Survival |
| Elias Akiki | Female/70 years | Stage IV lung adenocarcinoma (pleural metastasis, pericardial, mediastinal lymphadenopathy) Treatment: pembrolizumab and pemetrexed (chemotherapy) | Apixaban (AF and PE) | Stroke | Mitral | LMWH | Survival |
| William R Rankin | Female/78 years | Acute myeloid leukaemia | Apixaban (DVT) | Stroke | Mitral + Aortic | LMWH | Survival |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInfective Endocarditis Diagnosis and Management · Cardiac tumors and thrombi · Actinomycetales infections and treatment
Introduction
Non-bacterial thrombotic endocarditis (NBTE) is a rare and often underdiagnosed condition characterized by sterile valvular vegetations, typically associated with malignancy and systemic embolic events. We report the case of a 64-year-old woman with metastatic lung adenocarcinoma who developed NBTE while on rivaroxaban, later complicated by pulmonary embolism and ischaemic stroke. Mitral valve vegetations were identified on imaging and the diagnosis was established based on clinical, imaging, and laboratory findings. Despite a switch to low molecular weight heparin, her condition deteriorated. This case highlights the diagnostic and therapeutic challenges of NBTE in oncology and the need for individualized anticoagulation strategies.
Summary figure
**: **
Case presentation
A 64-year-old woman arrived at the emergency department in March 2023, with visual disturbances and increasing dyspnoea (NYHA grade III). She had a history of non-small-cell lung-carcinoma diagnosed two months prior, treated with Pembrolizumab (first cycle in March 2023), and a right femoral vein thrombosis (3 months earlier) for which she was on Rivaroxaban (15 mg twice daily for 21 days, followed by 20 mg once daily). Cardiac auscultation indicated a regular heart rhythm without murmurs, and clinical examination revealed cachexia with right lower limb paresis. Laboratory tests revealed thrombocytopenia (128 000/mm^3^), elevated D-dimers (35200 ng/mL), and decreased fibrinogen (0,85 g/L) with no signs of inflammation (CRP—C-reactive protein 6,8 mg/L) or organ dysfunction.
A contrast-enhanced brain CT scan was normal, while a pulmonary CT angiogram revealed bilateral pulmonary embolism despite adequate anticoagulation. The patient was admitted to the neurology department for stroke assessment and began treatment with low molecular weight heparin (LMWH). A brain MRI confirmed an ischaemic stroke in the territory of the right posterior cerebral artery and excluded cerebral metastasis.
In this context, a cardiovascular evaluation was requested to investigate a potential embolic source. A transthoracic echocardiogram performed revealed a mass attached to the anterior mitral leaflet (not present in the last echocardiogram conducted three weeks earlier). The mass was located on the ventricular side of the anterior mitral leaflet, measuring 18×7 mm, and was associated with moderate mitral regurgitation (Figure 1). Left ventricular function was preserved and no other masses were identified on the aortic or tricuspid valves.
Transthoracic echocardiography (13 April 2023), four-chamber view. A mass extending on the anterior mitral leaflet is visualized, measuring 18× 7 mm (arrow). Anatomical landmarks: AML, anterior mitral leaflet; LA, left atrium; LV, left ventricle; RV, right ventricle; RA, right atrium.
Therefore, a transoesophageal echocardiogram (Figure 2) found a mobile vegetation measuring 21×7 mm, causing moderate eccentric mitral insufficiency along the lateral edge of the left atrium. Given the context of massive bilateral pulmonary embolism, the possibility of a patent foramen oval causing a paradoxical stroke was considered but the bubble test could not be conducted appropriately due to the patient's lack of cooperation and time constraints.
Transoesophageal echocardiography (TEE) (14 April 2023). (A) TEE zoom view (93°): mass measured 21× 7 mm (orange arrow). (B) TEE view (20°): mass measured at 21× 7 mm (orange arrow). (C) TEE view (20°): mitral regurgitation quantified as moderate by PISA method: SOR (Surface orifice regurgitation) 0.25 cm2, VOR (Volume of regurgitation) 34 mL, red arrow. Mass attached to AML (arrow). (D) TEE anterior view of the mitral valve—3D reconstruction (120°): mass attached to the anterior mitral leaflet (arrow). Anatomical landmarks: AML, anterior mitral leaflet (A1–A3); PML, posterior mitral leaflet (P1–P3); LA, left atrium; LV, left ventricle; RV, right ventricle; RA, right atrium.
The differential diagnosis initially focused on infectious endocarditis; however, negative blood cultures and absence of inflammation made this unlikely. The diagnosis shifted towards marantic endocarditis (ME) or Libman–Sacks endocarditis, suggested by positive ANCA (1/320), hypothesizing that it was induced by immunotherapy. The search for antiphospholipid antibodies revealed a positive lupus anticoagulant, while anti-B2GP1 and anticardiolipin antibodies were negative. Considering the patient's history and the evolving neoplastic context, the hypothesis of ME was retained, and anticoagulation therapy with LMWH continued.
The patient's management was complicated by her refusal of further examinations and chemotherapy, leading to cancer progression (Figure 3). Despite adequate heparin therapy, echocardiography revealed increasing mass on the anterior mitral leaflet and a new mass on the posterior mitral leaflet (Figure 4). Following psychiatric consultation, she expressed a wish to return home, where she passed away shortly afterward.
Chest angioscanner scans in lung (B–D) and mediastinal windows (A–C) from 31 January 2023 to 14 June 2023, showing increased size of the spiculated lesion in the left lower lobe (orange arrow) and progressive mediastinal lymphadenopathy (red arrow).
Transthoracic echocardiography (16 June 2023), three-chamber zoom view: mass on the anterior mitral leaflet (18× 15 mm, arrow) and new mass on the posterior mitral leaflet (8.5× 4.0 mm, arrow). Anatomical landmarks: AML, anterior mitral leaflet; PML, posterior mitral leaflet; LA, left atrium; LV, left ventricle.
Discussion
Non-bacterial thrombotic endocarditis (NBTE) features sterile thrombotic vegetations without microorganisms, inflammation, or valvular damage.^1^ ME is a rare complication in malignancies, particularly lung adenocarcinomas followed by gastric and pancreatic adenocarcinomas, and then breast and genitourinary cancer. A multi-factorial hypercoagulable state often underlies NBTE and may present with signs of disseminated intra-vascular coagulation, as in our patient.
Given systemic emboli and mitral vegetations, infective endocarditis was first suspected. However, absence of fever, inflammatory markers, and persistently negative blood cultures made this unlikely, aligning with ESC guidelines.^2^ Positive ANCA and lupus anticoagulant raised suspicion for Libman–Sacks endocarditis, typically associated with systemic lupus or antiphospholipid syndrome. These immune-mediated lesions preferentially affect the mitral valve and are best visualized on transoesophageal echocardiography. Our patient had no autoimmune history but was receiving pembrolizumab, an ICI known to trigger de novo autoimmunity.^3^ The 2022 ESC guidelines list ICI-related myocarditis and vasculitis among cardiovascular risks (Lyon et al., 2022). Still, no established link exists between ICIs and Libman–Sacks. A possible false-positive lupus anticoagulant result due to rivaroxaban, and absent systemic features, made this diagnosis unlikely. NBTE is the most plausible diagnosis in malignancy patients with systemic emboli, sterile vegetations, and negative cultures.
Initially prescribed for DVT (deep vein thrombosis), rivaroxaban was continued after cancer diagnosis due to clinical stability and patient preference. The Caravaggio trial supports DOACs in cancer-associated thrombosis.^4^ Following the pulmonary embolism, LMWH was initiated in accordance with the 2023 ESC guidelines, which recommend LMWH or UFH for the management of NBTE and advice against the use of DOACs.^2^ Anti-Xa levels were not measured, but dosing and compliance were verified.
A literature review identified only 10 ME cases under anticoagulation (Table 1): mean age 61.2, equal gender distribution, 80% on DOACs, 100% mitral valve involvement, 70% presented with stroke. This highlights both the rarity of ME under anticoagulants and the uncertainty surrounding optimal management.
ME treatment centres on anticoagulation and cancer control. While DOACs like edoxaban and rivaroxaban inhibit factor Xa, they may be ineffective in this context. LMWH remains preferred in NBTE, as per ESC, ASCO, and Chest guidelines.^14^ The case reported by Akiki et al.^12^ supports this approach: NBTE under apixaban resolved after switching to enoxaparin. Venepally et al.^1^ found that progressive cancer was the strongest predictor of mortality, even with appropriate anticoagulation.
Prognosis depends on aetiology and extent. Our patient had advanced lung adenocarcinoma and mediastinal lymphadenopathy, associated with poor survival. Compared with previously reported cases, this presentation appears unusual, as it involved NBTE under rivaroxaban in a patient treated exclusively with pembrolizumab. Unlike Akiki et al., our patient worsened post-LMWH switch and died. This supports previous findings that associate poor outcomes with advanced or progressive disease.^1^
To our knowledge, few reports have considered Libman–Sacks endocarditis in ICI-treated patients without autoimmune disease, making this case noteworthy. This serological profile, possibly influenced by immunotherapy, illustrates a diagnostic complexity not previously addressed.
Though thrombotic events pre-dated pembrolizumab, PD-1 inhibitors may enhance thrombosis risk via endothelial dysfunction and immune activation.^15^ This supports close thrombotic monitoring in oncology patients receiving ICIs.
Given cancer progression and limited response to LMWH, antiplatelet therapy was considered. However, due to bleeding risk and the absence of guideline recommendations, it was not pursued. None of the reviewed cases reported using this strategy.
In conclusion, ME should be suspected in cancer patients with systemic embolism, sterile vegetations, and no infection signs. A comprehensive differential, guideline-based anticoagulation, and multimodal imaging are key. This case underscores the diagnostic and therapeutic uncertainty surrounding NBTE, reinforcing the need for evidence-based recommendations.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Venepally NR, Arsanjani R, Agasthi P, Wang P, Khetarpal BK, Barry T, et al A new insight into nonbacterial thrombotic endocarditis: a systematic review of cases. Anatol J Cardiol 2022;26:743–749.36052565 10.5152/Anatol J Cardiol.2022.1282 PMC 9623215 · doi ↗ · pubmed ↗
- 2Delgado V, Ajmone Marsan N, de Waha S, Bonaros N, Brida M, Burri H, et al 2023 ESC guidelines for the management of endocarditis: developed by the task force on the management of endocarditis of the European Society of Cardiology (ESC) endorsed by the European association for cardio-thoracic surgery (EACTS) and the European association of nuclear medicine (EANM). Eur Heart J 2023;44:3948–4042.37622656
- 3Blakeway EA, Elshimy N, Muinonen-Martin A, Marples M, Mathew B, Mitra A. Cutaneous lupus associated with pembrolizumab therapy for advanced melanoma: a report of three cases. Melanoma Res 2019;29:338–341.30762712 10.1097/CMR.0000000000000587 · doi ↗ · pubmed ↗
- 4Agnelli G, Becattini C, Meyer G, Muñoz A, Huisman MV, Connors JM, et al Apixaban for the treatment of venous thromboembolism associated with cancer. N Engl J Med 2020;382:1599–1607.32223112 10.1056/NEJ Moa 1915103 · doi ↗ · pubmed ↗
- 5Pons F, Poyet R, Daranda E, Prunet B, Jego C, Boret H, et al [Ischemic strokes as a presenting feature of marantic endocarditis despite heparin treatment]. Ann Cardiol Angeiol (Paris) 2011;60:233–235.20723881 10.1016/j.ancard.2010.07.013 · doi ↗ · pubmed ↗
- 6Shoji MK, Kim JH, Bakshi S, Govea N, Marukian N, Wang SJ. Nonbacterial thrombotic endocarditis due to primary gallbladder malignancy with recurrent stroke despite anticoagulation: case report and literature review. J Gen Intern Med 2019;34:1934–1940.31313109 10.1007/s 11606-019-05166-5PMC 6712189 · doi ↗ · pubmed ↗
- 7Mantovani F, Navazio A, Barbieri A, Boriani G. A first described case of cancer-associated non-bacterial thrombotic endocarditis in the era of direct oral anticoagulants. Thromb Res 2017;149:45–47.27888769 10.1016/j.thromres.2016.11.016 · doi ↗ · pubmed ↗
- 8Soga Y, Taira K, Sugimoto A, Kurosawa M, Kira H, Su T, et al Mitral valve nonbacterial thrombotic endocarditis: a rare multi-surgery-tolerant survivor of trousseau’s syndrome. Surg Case Rep 2018;4:104.30159818 10.1186/s 40792-018-0513-5PMC 6115325 · doi ↗ · pubmed ↗