Delayed diagnosis of ventricular lead malposition in the left ventricle via a patent foramen ovale
Georgia Goranitou, Nikitas Saroukos, Eleni Kalkandi, Paraskevi Georgiou, Skevos Sideris

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
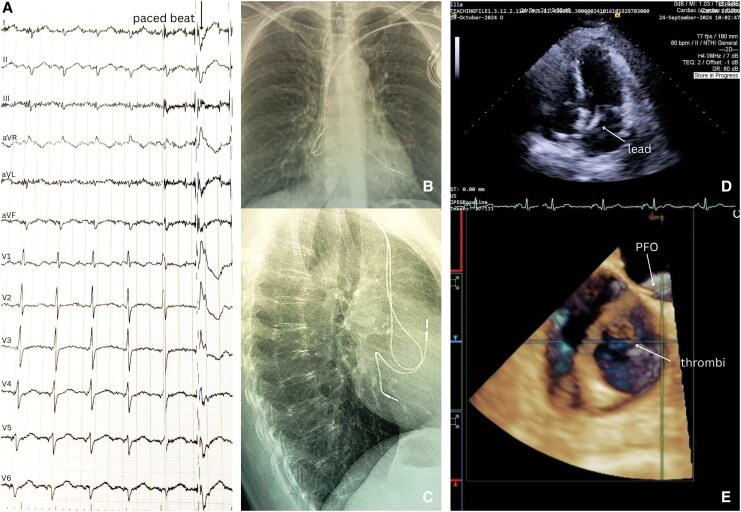 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac Structural Anomalies and Repair · Cardiac pacing and defibrillation studies · Orthopaedic implants and arthroplasty
Case description
A 55-year-old woman with systemic lupus erythematosus and a dual-chamber pacemaker (implanted 6 years earlier for sick sinus syndrome) presented with dizziness and gait unsteadiness. Neurological examination and brain CT angiography were unremarkable. The patient was in sinus rhythm. Device interrogation showed normal pacemaker function, but the 12-lead paced electrocardiogrram exhibited right bundle branch block (RBBB) morphology with delayed precordial transition at lead V_5_, suggesting ventricular lead malposition in the left ventricle (LV)^1,2^ (Figure 1A).
The posteroanterior chest radiography (PA X-ray) revealed an abnormally high and leftward position of the ventricular lead, while the lateral view showed a posterior trajectory (Figure 1B and C). Transthoracic echocardiography (TTE) demonstrated the ventricular lead traversing the interatrial septum, crossing the mitral valve, and anchoring in the LV inferoseptal wall (Figure 1D). Transoesophageal echocardiography (TEE) confirmed passage through a patent foramen ovale with two adherent thrombi (Figure 1D). Positron emission tomography/computed tomography excluded infection.
Diagnostic findings of ventricular lead malposition in the left ventricle. (A) Twelve-lead electrocardiogram: sinus rhythm with a ventricular paced beat (arrow) showing right bundle branch block morphology with late precordial transition at lead V5. (B) Posteroanterior chest X-ray: abnormal superior-leftward ventricular lead course. (C) Lateral chest X-ray: posterior ventricular lead trajectory, suggesting LV position. (D) 2D transthoracic echocardiography (apical four-chamber view): ventricular lead (arrow) traversing interatrial septum, crossing mitral valve, and anchored in LV inferoseptum. (E) 3D transoesophageal echocardiography (bicaval view): ventricular lead crossing a patent foramen ovale (arrow) with attached thrombi (arrow).
The patient was started on acenocoumarol (target INR 2.5–3.0). After 4 weeks, both atrial and ventricular leads were percutaneously extracted, and a new pacemaker was implanted contralaterally without complications. Anticoagulation continued for 1-month post-procedure. At 4-month follow-up, she remained asymptomatic.
This case illustrates the need for (i) heightened awareness of delayed lead malposition presentations, (ii) systematic evaluation of paced QRS morphology (e.g. RBBB pattern) integrated with multimodal imaging (X-ray, TTE, TEE) in pacemaker recipients with neurologic symptoms, and (iii) immediate intervention upon stroke identification to mitigate further thromboembolic risk.
Consent: Written informed consent was obtained from the patient for publication of this case report and any accompanying images, in line with the Committee on Publication Ethics (COPE) guidelines.
Funding: No funding was received for this manuscript.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Tzeis S, Andrikopoulos G, Weigand S, Grebmer C, Semmler V, Brkic A, et al Right bundle branch block-like pattern during uncomplicated right ventricular pacing and the effect of pacing site. Am J Cardiol 2016;117:935–939.26796192 10.1016/j.amjcard.2015.12.028 · doi ↗ · pubmed ↗
- 2Barold SS, Giudici MC. Renewed interest in the significance of the tall R wave in ECG lead V 1 during right ventricular pacing. Expert Rev Med Devices 2016;13:611–613.27347615 10.1080/17434440.2016.1195258 · doi ↗ · pubmed ↗