Facilitators and Barriers of Accessibility and Utilization of Healthcare Facilities in India: A Qualitative Metasynthesis
Aviraj KS, Manvi Sagar, Sarit Sharma, Debkumar Pal

TL;DR
This study explores what helps or hinders people in India from accessing healthcare, combining insights from many qualitative studies.
Contribution
The study provides a comprehensive synthesis of facilitators and barriers to healthcare access in India using qualitative metasynthesis.
Findings
Ten overarching themes were identified, including care accessibility and systemic challenges.
Facilitators like facility cleanliness and staff behavior contrast with barriers like financial constraints.
The findings highlight the need for system-wide interventions to improve healthcare access in India.
Abstract
India's healthcare system, a blend of public and private providers, faces deep-rooted inequities that hinder access for many. Rural areas lack adequate resources, while financial constraints prevent countless families from affording private care. This qualitative metasynthesis was conducted to explore and analyze the facilitators and barriers that shape access and utilization to both government-run and private healthcare establishments in India, delving deep into the insights provided by qualitative research methodologies. In March 2024, we systematically searched PubMed, Scopus, Embase, and Google Scholar databases for qualitative studies related to facilitators and barriers of accessing government or private healthcare facilities in India. We included qualitative studies and mixed-method studies that reported themes and subthemes related to facilitators and barriers toward accessing…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
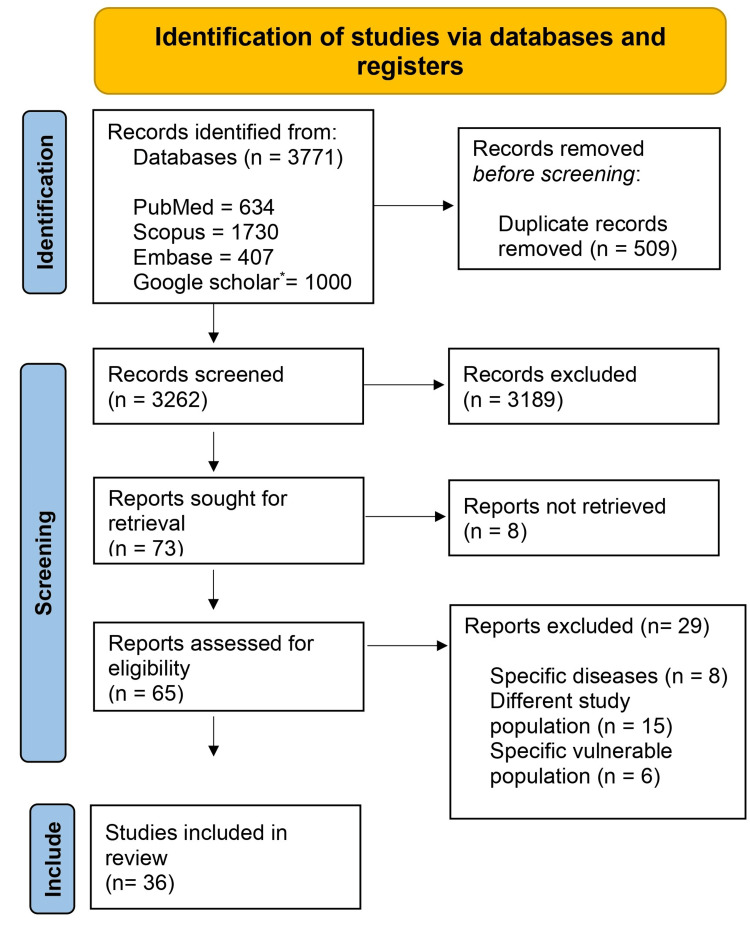 Figure 1
Figure 1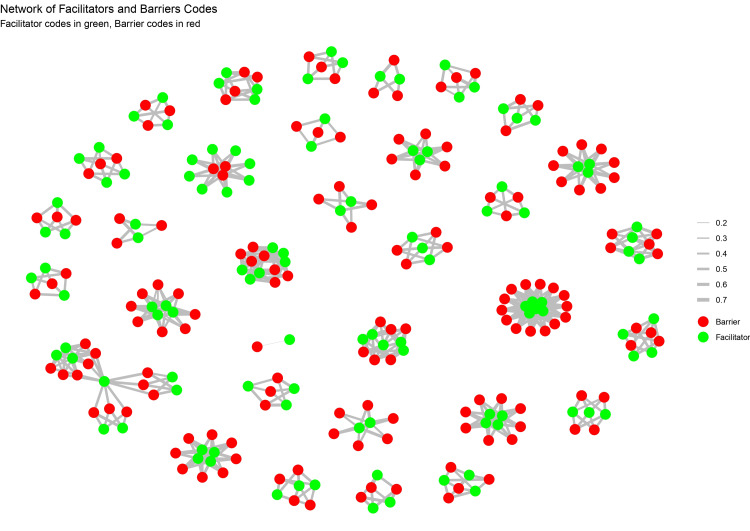 Figure 2
Figure 2 Figure 3
Figure 3| S. No. | Author (First author) | Year of publication | Study area | Study design | Study population | Sample size | Tool for data collection | Type of sampling | Type of analysis |
| (Thematic/content) | |||||||||
| 1 | Bhattacharyya et al. [ | 2015 | Uttar Pradesh, India | Qualitative study | Recently delivered women and healthcare providers | 40 | In-depth interviews | Purposive sampling | Thematic analysis |
| 2 | Varghese et al. [ | 2015 | SadholiKadim block, rural Uttar Pradesh, India | Qualitative study | Caregivers of children with intellectual disabilities | 10 | Semistructured interviews | Convenience and snowball sampling | Thematic analysis |
| 3 | Gawde et al. [ | 2016 | Mumbai, India | Mixed-method study | Migrant women who had delivered in the last two years | 234 | Structured interview schedules, qualitative in-depth interviews | Multistage cluster sampling | Thematic/content analysis |
| 4 | Vidler et al. [ | 2016 | Karnataka, India | Qualitative study | Women of reproductive age, community health workers, and health system representatives | 46 | Focus group discussions and one-to-one interviews | Purposive sampling | Thematic analysis |
| 5 | Merugumala et al. [ | 2017 | Hyderabad, India | Qualitative study | Parents and clinic staff related to the care of hearing-impaired children | 25 | Semistructured interviews | Opportunistic sampling | Thematic analysis |
| 6 | Nielsen et al. [ | 2017 | Tamil Nadu, India | Qualitative study | Pregnant women | 39 | Semistructured interviews and observations at health facilities | Purposive sampling | Content analysis |
| 7 | Vellakkal et al. [ | 2017 | Jharkhand, Madhya Pradesh, Uttar Pradesh (India) | Qualitative study | Eligible women, their spouses, mothers-in-law, and ASHAs (Accredited Social Health Activists) | 112 | In-depth qualitative interviews | Purposive sampling | Thematic analysis |
| 8 | Rath et al. [ | 2018 | India | Qualitative study | Oral cancer patients | 70 | Face-to-face in-depth interviews using a semistructured questionnaire | Convenience sampling | Thematic analysis |
| 9 | Patel et al. [ | 2018 | Bihar, India | Qualitative study | Scheduled Caste (SC) women | 18 | Semistructured interviews | Purposive sampling | Thematic/content using framework analysis |
| 10 | Siddaiah et al. [ | 2018 | Haryana, India | Mixed-method study | Migrant women laborers working in brick kilns | 500 | Surveys/questionnaires | Purposive sampling | Thematic/content analysis |
| 11 | Elias et al. [ | 2018 | Tumkur, Karnataka, India | Mixed-methods study | Households and healthcare workers | 1149 | Household and health facility surveys, focus group discussions (FGDs), and in-depth interviews | Cluster-randomized design for household survey | Thematic analysis |
| 12 | Tripathy et al. [ | 2019 | 6 districts in three states of India | Sequential mixed-methods study | Healthcare providers and persons with diabetes at public health facilities | 30 health facilities, 42 physicians, and 37 patients | Semistructured interviews, hospital records review, and observation checklist | Convenience sampling | Thematic/content analysis |
| 13 | Faruqui et al. [ | 2019 | India | Qualitative study | Caregivers of children with cancer | 39 | In-depth interviews | Purposive sampling | Thematic content analysis |
| 14 | Jayakumar al. [ | 2019 | Bihar and Jharkhand, India | Qualitative study | Female patients with visceral Leishmaniasis, health staff, local health providers, and community elders | 33 | Semistructured in-depth interviews | Purposive sampling | Thematic analysis |
| 15 | Kung et al. [ | 2019 | Surat, India | Qualitative study | Women living with HIV | 40 | In-depth interviews | Purposive sampling | Content analysis |
| 16 | Holloway et al. [ | 2020 | Rural India | Ethnographic qualitative study | Caregivers of sick children attending the pediatric outpatient department | 43 | Unstructured observations, structured observations, and semistructured interviews | Purposive sampling | Thematic analysis |
| 17 | George et al. [ | 2020 | Attapadi, Kerala | Qualitative study | Indigenous community, healthcare providers, and key informants in Attapadi | 47 in-depth interviews, 6 focus group discussions | Interviews, FGDs, and participant observation | Theoretical sampling | Thematic analysis |
| 18 | Raizada et al. [ | 2020 | India | Mixed-method study | Pediatric tuberculosis (TB) patients | 100 | Semistructured questionnaires | Random selection of patients from four Indian cities | Thematic content analysis |
| 19 | Kathrikolly et al. [ | 2020 | Coastal Karnataka, India | Qualitative study | Rural women aged 20-60 years | 44 | FGDs | Purposive sampling | Thematic analysis |
| 20 | Boro and Saikia [ | 2020 | Assam, India | Qualitative study | Tribal men and women aged 25–50 residing in the study setting; health service providers from rural public health facilities | 60 | Semistructured open-ended questionnaire | Snowball sampling | Thematic analysis |
| 21 | Santalahti et al. [ | 2020 | Manipal, Karnataka, India | Qualitative study | Migrant construction workers | 15 | Semistructured interviews | Convenience and purposive sampling | Thematic/content analysis |
| 22 | Wood et al. [ | 2020 | India | Qualitative study | Lay mental health workers (LHWs) and stakeholders | 50 | In-depth interviews | Maximum variation sampling | Thematic analysis |
| 23 | Mukerji and Turan [ | 2020 | Kolkata, India | Qualitative study | Female TB patients | 20 | In-depth interviews | Purposive sampling | Thematic analysis |
| 24 | Faruqui et al. [ | 2020 | India | Qualitative study | Healthcare providers | 27 | Semistructured interviews | Purposive sampling | Thematic/content analysis |
| 25 | Dsouza et al. [ | 2020 | India (Himachal Pradesh, Meghalaya, and Karnataka) | Qualitative study | Women aged 30-59, state/district program managers, and other healthcare staff | 18 | FGDs and in-depth interviews | Convenience sampling | Thematic analysis |
| 26 | Vijayan et al. [ | 2021 | Family Health Center, Mundur, Thrissur district, Kerala, India | Qualitative study | Patients, medical officers, health inspectors, accountants, ASHAs, and community members | 35 | In-depth interviews and focus group discussions | Convenience sampling | Thematic analysis |
| 27 | Kulkarni et al. [ | 2021 | Pune, Maharashtra, India | Qualitative study | Transgenders and commercial sex workers | 24 | In-depth interviews and focus group discussions | Purposive sampling | Thematic analysis |
| 28 | Pati et al. [ | 2021 | Urban primary healthcare centers in Bhubaneswar city, Odisha, India | Qualitative study | Primary care physicians | 17 | Digitally recorded interviews | Purposive and convenience sampling | Thematic analysis |
| 29 | Adsul et al. [ | 2022 | Mysore, India | Qualitative study | Physicians (primary care physicians, obstetricians/gynecologists, oncologists, and pathologists) | 30 | Semistructured interviews | Convenience sampling followed by snowball sampling | Thematic analysis |
| 30 | Wani et al. [ | 2022 | North India | Mixed-method study | Healthcare workers | 113 | Semistructured questionnaire, interviews, and FGDs | Convenience sampling | Thematic analysis |
| 31 | Thiagesan et al. [ | 2022 | Tamil Nadu, India | Qualitative study | Primary healthcare providers | 13 | In-depth interviews | Purposive sampling | Thematic analysis |
| 32 | Mohanraj et al [ | 2022 | Uttar Pradesh (UP) and Madhya Pradesh (MP), India | Qualitative study | Healthcare providers (HCPs), including doctors and community health workers (CHWs) | 23 | Semistructured interviews (SSIs) and FGDs | Purposive sampling | Thematic analysis |
| 33 | Rajbangshi et al. [ | 2022 | India | Qualitative study | Internally displaced Bru women in India | 54 | FGDs and in-depth interviews | Purposive sampling | Thematic/content analysis |
| 34 | Cáceres et al. [ | 2023 | Tening, a block in Peren district, Nagaland, India | Mixed-methods study | Indigenous tribal community (Liangmai Naga tribe) | 166 | Semistructured cross-lingual FGDs, IDIs, and an extensive district-level community-based cross-sectional survey | Purposive sampling | Thematic analysis |
| 35 | Bangar et al. [ | 2023 | Rural sites in Maharashtra, Odisha, MP, and UP | Qualitative study | Men having sex with men (MSM) | 48 | Interviews (key informant interviews (KIIs) and in-depth interviews (IDIs)) and FGDs | Purposive and convenient sampling | Thematic analysis |
| 36 | Saha [ | 2023 | Lakhimpur district, Assam, India | Mixed-methods study | Households in flood-prone areas | 83 | Interview schedules | Random sampling technique | Thematic analysis |
| S. No. | Author (First author) | Year of publication | Themes | Subthemes | Codes |
| 1 | Bhattacharyya et al. [ | 2015 | 1. Accessibility of care | 1. Ease of physical access | 1. Physical proximity to health facilities |
| 2. Cleanliness of facilities | 2. Maintenance of facility hygiene | 2. Regular cleaning routines | |||
| 3. Interpersonal behavior of staff | 3. Respectful treatment by healthcare staff | 3. Staff-patient interactions | |||
| 4. Information sharing | 4. Clarity and frequency of communication with patients | 4. Details of care provided and patient education | |||
| 2 | Varghese et al. [ | 2015 | Attitude and availability of healthcare provider | Availability of local healthcare providers | 1. Kindness of healthcare staff |
| 2. Willingness to treat common diseases | |||||
| 3 | Gawde et al. [ | 2016 | 1. Social support in the home town | 1. Strong social networks back home | 1. Assistance from family and neighbors |
| 2. Familiarity with the healthcare system | 2. Previous positive experiences with healthcare services | 2. Recommendations from friends and neighbors | |||
| 3. Perceived quality of healthcare | 3. Preference for healthcare services in Mumbai due to better infrastructure | 3. Availability of services like ambulance | |||
| 4 | Vidler et al. [ | 2016 | 1. Government programs | 1. Cash incentives for antenatal care visits | 1. Antenatal care attendance |
| 2. Community health workers' encouragement | 2. Institutional deliveries | 2. Delivery in health facilities | |||
| 3. Availability of maternity services | 3. Transport services | 3. Postpartum care for neonates | |||
| 5 | Merugumala et al. [ | 2017 | 1. Community and social support | 1. Peer support among parents | 1. Specific instances of community help |
| 2. Awareness and information sharing | 2. Role of healthcare professionals in education | 2. Educational insights | |||
| 3. Accessibility of healthcare services | 3. Charitable services providing free access | 3. Financial aid instances | |||
| 6 | Nielsen et al. [ | 2017 | 1. Awareness and knowledge about GDM | 1. Community outreach programs | 1. Health education sessions |
| 2. Support systems | 2. Influence of family, especially husband's support | 2. Family involvement in healthcare | |||
| 3. Accessibility of Healthcare Services | 3. Role of healthcare providers in educating patients | 3. Doctor-patient communication | |||
| 4. Availability of screening facilities close to home | 4. Ease of access to health facilities | ||||
| 7 | Vellakkal et al. [ | 2017 | 1. Awareness and support | 1. Awareness among women and family | 1. Education on the benefits of institutional delivery |
| 2. ASHA (Accredited Social Health Activists) role | 2. ASHA's support and services | 2. ASHA's assistance in registration and transport | |||
| 3. Institutional trust | 3. Trust in healthcare facilities | 3. Preference for hospital due to perceived safety | |||
| 8 | Rath et al. [ | 2018 | 1. Awareness and knowledge | 1. Role of mass media and education | 1. Influence of educational programs |
| 2. Social influence and support | 2. Family and community encouragement | 2. Support from family members for seeking care | |||
| 3. Personal health concerns | 3. Recognition of symptom severity | 3. Patients' realization of the seriousness of symptoms | |||
| 4. Accessibility to healthcare services | 4. Availability of local healthcare facilities | 4. Ease of access to local clinics or hospitals | |||
| 9 | Patel et al. [ | 2018 | 1. Government interventions | 1. Introduction of ASHAs and free health services | 1. ASHA involvement |
| 2. Cultural shifts in health practices | 2. Acceptance of institutional deliveries | 2. Free service utilization | |||
| 3. Information dissemination and support services | 3. Role of government schemes like Janani Shishu Suraksha Karyakram (JSSK) | 3. Institutional delivery preference | |||
| 10 | Siddaiah et al. [ | 2018 | 1. Awareness and knowledge about maternal health services | 1. Understanding of local health systems | Absence of knowledge gaps, awareness levels, and use of government health benefits |
| 2. Accessibility of public health services | 2. Engagement with public health initiatives | ||||
| 3. Utilization of government schemes | |||||
| 11 | Elias et al. [ | 2018 | 1. Community engagement and awareness | 1. Educational programs on non-communicable diseases (NCDs) | 1. Initiatives for program awareness |
| 2. Accessibility of healthcare services | 2. Proximity of healthcare facilities | 2. Patient satisfaction with healthcare proximity | |||
| 12 | Tripathy et al. [ | 2019 | 1. Availability of resources | 1. Availability of drugs and laboratory investigations | 1. Availability of diagnostic tools |
| 2. Health system infrastructure | 2. Tertiary and secondary care facilities' role | 2. Provision of medications | |||
| 3. Presence of specialized consultations and diagnostic capabilities | |||||
| 13 | Faruqui et al. [ | 2019 | 1. Community and family support network | 1. Emotional and practical support from extended family and community | 1. Moral and emotional encouragement |
| 2. Access to information and healthcare awareness | 2. Clarity and understanding of cancer diagnosis and treatment processes | 2. Acquiring and sharing knowledge about child’s condition and care options | |||
| 14 | Jayakumar al. [ | 2019 | 1. Awareness of disease | 1. Health education campaigns | 1. Effective community outreach |
| 2. Community engagement | 2. Role of local health workers | 2. Community advice for seeking care | |||
| 3. Government intervention | 3. Insurance coverage campaign | 3. Government health campaigns | |||
| 15 | Kung et al. [ | 2019 | 1. Awareness and knowledge about cervical cancer and screening | 1. Understanding of cervical cancer risks and screening benefits | 1. Seeking information |
| 2. Motivation for health maintenance | 2. Health consciousness and proactive attitude | 2. Prioritizing health | |||
| 3. Family and social support | 3. Spousal encouragement and family involvement | 3. Support from husband and other family members | |||
| 16 | Holloway et al. [ | 2020 | Diagnostic acceptability | 1. Trust in healthcare | 1. Caregivers' trust in physicians' expertise |
| 2. Understanding and value of diagnostics | 2. Perception of hospital as a high-quality, cost-effective facility | ||||
| 3. Recognition of diagnostics for accurate illness identification | |||||
| 4. Appreciation of diagnostics for targeted treatment | |||||
| 17 | George et al. [ | 2020 | 1. Government interventions | 1. Financial protection schemes | 1. Free healthcare services and reimbursement of indirect costs |
| 2. Community engagement | 2. Healthcare infrastructure improvement | 2. Upgraded health facilities and specialist appointments | |||
| 3. Inclusion in decision-making | 3. Village chief consultations and community health committees | ||||
| 18 | Raizada et al. [ | 2020 | 1. Proactive family support | 1. Willingness to seek care | 1. Family's determination for treatment |
| 2. Availability of diagnostic tools | 2. Knowledge of TB management | 2. Awareness of TB symptoms | |||
| 3. Public health interventions and policies | 3. Accessibility to free diagnostic testing | 3. Use of public sector facilities for testing | |||
| 19 | Kathrikolly et al. [ | 2020 | 1. Health concerns of women | 1. Self-care activities | 1. Awareness of breast cancer and screening |
| 2. Factors motivating the uptake of screening facilities | 2. Awareness camps | 2. Influence of female healthcare providers | |||
| 3. Perception of cancer prevention and control initiatives | 3. Government-led initiatives | 3. Community-based information dissemination strategies | |||
| 4. Information dissemination | 4. Mass media and interactive methods for information sharing | 4. Involvement of men in promoting women’s health | |||
| 5. Role of men in women’s health | 5. Educating men on women's health | ||||
| 20 | Santalahti et al. [ | 2020 | 1. Awareness and education | 1. Role of healthcare workers | 1. Knowledge about breast cancer |
| 2. Supportive healthcare providers | 2. Community-based health programs | 2. Trust in female doctors and nurses | |||
| 3. Community engagement | 3. Effectiveness of health camps | ||||
| 21 | Wood et al. [ | 2020 | 1. Community engagement | 1. Community trust | 1. Instances of positive community interactions |
| 2. Training and support | 2. Comprehensive training | 2. Supportive family anecdotes | |||
| 3. Personal growth | 3. Peer support | 3. Effective training experiences | |||
| 4. Self-efficacy | 4. Positive patient outcomes | ||||
| 22 | Mukerji et al. [ | 2020 | 1. Supportive clinic environment | 1. Positive staff-patient interaction | 1. Staff encouragement |
| 2. Free medication provision | 2. Financial relief through no-cost TB treatment | 2. Absence of treatment fees | |||
| 23 | Faruqui et al. [ | 2020 | 1. Integrated healthcare infrastructure | 1. Enhanced facility resources | 1. Availability of specialized equipment |
| 2. Comprehensive training programs | 2. Professional development and education | 2. Skill enhancement initiatives | |||
| 3. Multidisciplinary care approach | 3. Collaboration across specialties | 3. Team-based patient management | |||
| 24 | Dsouza et al. [ | 2020 | 1. Awareness and education | 1. Community engagement and outreach programs | 1. Health education sessions |
| 2. Accessibility of services | 2. Mobile health units and local health camps | 2. Availability of nearby health facilities | |||
| 3. Social support and encouragement | 3. Role of family and community leaders in promoting healthcare utilization | 3. Encouragement from family members | |||
| 25 | Vijayan et al. [ | 2021 | 1. Good staff behavior | 1. Enhanced patient-healthcare provider relationship | 1. Patient-staff interaction |
| 2. Evening outpatient services | 2. Increased healthcare access for working people and school children | 2. Operational hours | |||
| 3. Specialty clinics | 3. Benefits to the geriatric population | 3. Geriatric services | |||
| 4. Improved infrastructure | 4. Patient satisfaction with the health center's environment | 4. Infrastructure quality | |||
| 5. Accessibility | 5. Convenience of accessing the health center | 5. Accessibility and parking | |||
| 6. Subsidized laboratory services | 6. Motivation for staff | 6. Laboratory affordability | |||
| 7. Local self-government involvement | 7. Governmental support | ||||
| 8. Rewards | 8. Performance incentives | ||||
| 26 | Kulkarni et al. [ | 2021 | 1. Awareness and knowledge | 1. Understanding of eye care needs | 1. Recognition of visual impairment |
| 2. Community support | 2. NGO and social worker involvement | 2. Knowledge of available treatments | |||
| 3. Healthcare provider efforts | 3. Sensitivity and inclusivity | 3. Assistance in accessing healthcare | |||
| 4. Advocacy and guidance | |||||
| 5. Efforts to provide gender-neutral facilities | |||||
| 6. Empathetic treatment by some healthcare providers | |||||
| 27 | Pati et al. [ | 2021 | 1. Health system support | 1. Availability of NCD awareness campaigns | 1. Periodic follow-ups by health workers |
| 2. Professional development and training | 2. Support from pharmaceutical companies | 2. Provision of updated treatment modalities | |||
| 3. Community engagement and awareness | 3. Formal training in diabetes management | 3. Confidence in handling diabetes with comorbidities | |||
| 4. Peer learning and networking | 4. Use of seminars and workshops for knowledge enhancement | ||||
| 5. Role of community health workers | 5. Active engagement in treatment plans | ||||
| 6. Patient education campaigns | 6. Increased patient attentiveness to treatment | ||||
| 28 | Adsul et al. [ | 2022 | 1. Community engagement | 1. Culturally-tailored education | 1. Peer-led educational programs |
| 2. Provider training | 2. Utilization of community health workers | 2. Integration with women's social groups | |||
| 3. Health literacy enhancement | 3. Physician training programs | 3. Physician readiness for screening procedures | |||
| 29 | Wani et al. [ | 2022 | 1. Supportive institutional policies | 1. Availability of a dedicated palliative care unit | 1. Institutional support |
| 2. Training and education | 2. Regular training programs | 2. Professional development | |||
| 3. Policy amendments | |||||
| 30 | Thiagesan et al. [ | 2022 | 1. Innovative care approaches | 1. Local health innovations | 1. Use of physical activity adaptations |
| 2. Community and peer support | 2. Formation of peer support groups | 2. Peer education and support activities | |||
| 3. Cross-program resource utilization | 3. Integration of health services | ||||
| 31 | Mohanraj et al. [ | 2022 | 1. Strengthening public health infrastructure | 1. Improved availability and quality of public health facilities | 1. Infrastructure improvements |
| 2. Enhancing community health literacy | 2. Enhanced trust in government healthcare services | 2. Trust in public health services | |||
| 3. Effective utilization of community health workers | 3. Increased awareness about childhood pneumonia symptoms and treatment | 3. Awareness programs | |||
| 4. Education on the importance of seeking timely and appropriate care | 4. Training programs for community health workers | ||||
| 5. Regular training and skill enhancement of community health workers | 5. Community health workers support mechanisms | ||||
| 6. Support and supervision for community health workers | |||||
| 32 | Rajbangshi et al. [ | 2022 | 1. Community health worker engagement | 1. Role of ASHAs in healthcare delivery | 1. ASHAs assisting with institutional deliveries |
| 2. Awareness of health services | 2. Knowledge of reproductive health options | 2. Awareness of temporary contraceptive methods | |||
| 3. Positive attitudes toward seeking care | 3. Knowledge about medical abortion | ||||
| 4. Willingness to use reproductive and maternal health (RMH) services | |||||
| 33 | Cáceres et al. [ | 2023 | 1. Availability of healthcare services | 1. Proximity of healthcare facilities | 1. Nearby health centers |
| 2. Community support | 2. Role of family and neighbors | 2. Family encouragement | |||
| 3. Awareness programs | 3. Government health campaigns | 3. Health education sessions | |||
| 34 | Bangar et al. [ | 2023 | 1. Community engagement and sensitization | 1. Role of community liaison officers | 1. Empathetic healthcare providers |
| 2. Provision of specialized healthcare services | 2. Need for MSM-specific health workers | 2. Peer counseling | |||
| 3. Confidentiality and privacy in healthcare | 3. Safe spaces for health discussions | 3. Discreet health service locations | |||
| 35 | Saha et al. [ | 2023 | 1. Availability of boat clinics | 1. Mobile health clinics as essential services | 1. Use of boat clinics for healthcare |
| 2. Community resilience and adaptation | 2. Community support systems | 2. Community-led health initiatives |
| Theme | Description |
| Information sharing | Communication and health education |
| Cleanliness of facilities | Maintaining clean healthcare environments |
| Staff-patient interactions and empathy | Positive interactions, empathy, and compassionate care |
| Physical accessibility and proximity | Geographical accessibility to healthcare facilities and proximity to patients’ residences |
| Patient education and awareness | Educating patients about conditions, treatments, and available healthcare services |
| Knowledge of treatment options | Awareness of different treatment modalities and options |
| Gender-sensitive facilities | Facilities designed for diverse genders and inclusivity |
| Assistance programs and community support | Community-based assistance, support networks, and outreach programs |
| Advocacy and guidance | Efforts to bridge gaps in healthcare access through advocacy |
| Visual impairment considerations | Addressing the needs of visually impaired individuals within healthcare settings |
| Patient-centered care and trust-building | Shared decision-making, trust-building, and patient empowerment |
| Facilitator themes | Verbatim quotes |
| Accessibility of care [ | Accessibility of care encompasses the availability of healthcare services considering geographical, financial, and logistical factors. Studies stress the importance of proximity to healthcare facilities, particularly for low-income groups favoring government facilities. Local facility access is recognized as a facilitator. Qualitative research in central Kerala highlighted ease of access and ample parking as key factors influencing healthcare utilization [ |
| Interpersonal behavior of staff [ | Empathetic treatment and positive staff-patient interactions emerged as prominent facilitators in healthcare access and utilization. Studies highlighted instances where healthcare providers showed understanding and empathy, fostering trust and comfort. Promoting such positive interactions is crucial for motivating community members to utilize family health center services, as found in a qualitative study conducted in central Kerala [ |
| Cleanliness of facilities [ | Reflects the critical nature of cleanliness and sanitation in healthcare settings for infection control and patient safety. It points to the fundamental role of hygiene in patient care and the prevention of hospital-acquired infections. In a study, cleanliness was pointed out as a major challenge both by users and providers of healthcare, and if addressed, could easily facilitate healthcare access and utilization [ |
| Community support [ | Advocacy and guidance: The role of community support networks in facilitating healthcare access and utilization emerged in some studies. Community leaders or organizations might help navigate healthcare systems, particularly in rural areas. In a study [ |
| Efforts to provide gender-neutral facilities and recognition of visual impairment [ | Points to the specific acknowledgment and accommodation of visual disabilities in healthcare settings. It emphasizes the need for tailored healthcare services that address the unique challenges faced by visually impaired patients. Some studies highlighted efforts by private facilities to create gender-neutral restrooms or waiting areas, facilitating access for individuals with diverse gender identities. For instance, the comment of a 60-year-old transgender person was considered a barrier to healthcare utilization: “There are only male or female wards in the hospital. Where do people like me stay? Other patients would abuse me. Therefore, I am avoiding cataract surgery.” In this study [ |
| Information sharing [ | In the analysis, it was consistently observed that details of care provided and patient education played crucial roles. Clear communication regarding treatment options, procedures, and discharge instructions emerged as significant facilitators in ensuring access to healthcare services. Notably, users emphasized the importance of receiving timely and comprehensive information from healthcare providers, particularly regarding tests and their schedules [ |
| Healthcare provider efforts [ | Assistance in accessing healthcare emerged as a dominant facilitator code, highlighting the importance of logistical support in overcoming barriers. This underscores the value of transportation, financial aid, and appointment scheduling help. |
| Knowledge of available treatments [ | Awareness of treatment options is pivotal for patients, underscoring the necessity of clear communication between healthcare providers and patients. Instances in government healthcare settings where providers exhibit sufficient knowledge of available treatments facilitate access to appropriate care within the public healthcare system. Health system support [ |
| S. No. | Author (First author) | Year of publication | Themes | Subthemes | Codes |
| 1 | Bhattacharyya et al. [ | 2015 | 1. Inadequate infrastructure | 1. Insufficient facilities and equipment | 1. Specific infrastructural deficits |
| 2. Supply shortages | 2. Irregular availability of water, electricity, and medicines | 2. Items frequently out of stock | |||
| 3. Staffing issues | 3. Shortage of gynecologists and anesthetists | 3. Specific staffing gaps | |||
| 4. Privacy concerns | 4. Difficulty in maintaining patient confidentiality | 4. Examples of privacy violations | |||
| 5. Lack of post-delivery counseling | 5. Inadequate training in post-delivery care | 5. Lack of counseling sessions | |||
| 6. Management of referral cases | 6. Challenges in handling emergency referrals | 6. Case studies of referral management | |||
| 7. Nonfunctional blood banks | 7. Operational issues in blood banks | 7. Instances of blood bank failures | |||
| 8. Lack of incentives for staff | 8. Demotivation among healthcare workers due to inadequate rewards | 8. Expressions of staff dissatisfaction | |||
| 2 | Varghese et al. [ | 2015 | 1. Financial | 1. High treatment costs | 1. Cost of treatment |
| 2. Structural | 2. Unawareness of government aid | 2. Inaccessibility of specialists | |||
| 3. Cognitive | 3. Poor availability of healthcare providers | 3. Long distances | |||
| 4. Poor transportation difficulties | 4. Misunderstanding of the condition | ||||
| 5. Lack of referrals | 5. Lack of preventive care | ||||
| 6. Lack of caregiver knowledge | 6. Inadequate training | ||||
| 7. Inadequate provider education | |||||
| 3 | Gawde et al. [ | 2016 | 1. Sociocultural factors | 1. Lack of felt need for healthcare | 1. Preference for home delivery due to cost and cultural practices |
| 2. Economic constraints | 2. High living and healthcare costs in Mumbai | 2. Difficulties in navigating the urban healthcare system | |||
| 3. Structural barriers | 3. Inadequate health infrastructure | 3. Limited access to government programs for migrants | |||
| 4. Health system challenges | 4. Cumbersome administrative procedures | 4. Lack of migrant-friendly healthcare policies | |||
| 4 | Vidler et al. [ | 2016 | 1. Limited autonomy | 1. Cultural beliefs | 1. Decision-making power of women |
| 2. Poor access to transport | 2. Availability and cost of transport | 2. Access and affordability of transport | |||
| 3. Perceived poor quality of healthcare facilities | 3. Maintenance of health facilities | 3. Satisfaction with health services | |||
| 4. Financial constraints | 4. Costs related to healthcare | 4. Direct and indirect costs of care | |||
| 5 | Merugumala et al. [ | 2017 | 1. Cultural beliefs | 1. Influence of elders | 1. Specific beliefs of family elders |
| 2. Socioeconomic challenges | 2. Financial constraints | 2. Instances of financial hardship | |||
| 3. Healthcare system limitations | 3. Transportation difficulties | 3. Travel difficulties to healthcare centers | |||
| 6 | Nielsen et al. [ | 2017 | 1. Healthcare system challenges | 1. Inadequate healthcare facilities | 1. Lack of resources at health centers |
| 2. Sociocultural factors | 2. Stigma and societal norms affecting health-seeking behavior | 2. Social stigma related to GDM | |||
| 3. Personal barriers | 3. Personal constraints like time and financial issues | 3. Work and family commitments | |||
| 4. Economic constraints | |||||
| 5. Out-of-pocket expenses | |||||
| 6. Long wait time at clinics | |||||
| 7 | Vellakkal et al. [ | 2017 | 1. Sociocultural norms | 1. Cultural preference for home delivery | 1. Belief in natural childbirth |
| 2. System and environmental limitations | 2. Distance to facilities and poor quality of care | 2. Negative past experiences with healthcare facilities | |||
| 3. Financial and opportunity costs | 3. High costs of hospital delivery versus the cash incentive | 3. Perceived lower benefit of the cash incentive compared to the costs and efforts involved | |||
| 8 | Rath et al. [ | 2018 | 1. Ignorance and negligence | 1. Lack of symptom recognition | 1. Disregarding early symptoms as minor issues |
| 2. Financial constraints | 2. Economic difficulties in affording treatment | 2. Inability to pay for medical expenses | |||
| 3. Health system challenges | 3. Inefficiency and delays in the healthcare system | 3. Experiences of misdiagnosis or delayed diagnosis | |||
| 4. Cultural beliefs and stigma | 4. Fear of stigma | 4. Concerns about being stigmatized due to illness | |||
| 9 | Patel et al. [ | 2018 | 1. Inadequate health services infrastructure | 1. Insufficient ASHA (Accredited Social Health Activists) coverage and unauthorized charges | 1. Limited health workforce |
| 2. Financial constraints | 2. Costs related to transport and unofficial payments | 2. Financial burdens and unofficial costs | |||
| 3. Information and awareness gaps | 3. Lack of knowledge about available services and emergency care | 3. Emergency care awareness and information deficiency | |||
| 10 | Siddaiah et al. [ | 2018 | 1. Misconceptions and mistrust about the public health system | 1. Influence of substandard private healthcare at brick kilns | Mistrust, misinformation, inaccessibility, systemic apathy, and partial insurance coverage |
| 2. Barriers to Universal Health Coverage | 2. Systemic issues in public healthcare | ||||
| 3. Socioeconomic and logistical challenges | 3. Geographical and time-related constraints | ||||
| 11 | Elias et al. [ | 2018 | 1. Systemic healthcare deficiencies | 1. Inadequate healthcare infrastructure | 1. Reports of healthcare worker shortages |
| 2. Financial constraints | 2. High out-of-pocket expenditures | 2. Burden of medical costs on families | |||
| 3. Social and cultural barriers | 3. Stigma and discrimination in healthcare settings | 3. Negative perceptions of programs | |||
| 12 | Tripathy et al. [ | 2019 | 1. Systemic and structural challenges | 1. Insufficient resources at primary level | 1. Lack of diagnostic tools at primary health centers |
| 2. Operational and management issues | 2. Patient overload and lack of training | 2. Overcrowding at tertiary facilities | |||
| 3. Patient-centered care challenges | 3. Accessibility and follow-up | 3. Lack of specialized diabetic care training for primary healthcare providers | |||
| 4. Difficulty in patient follow-up due to system limitations | |||||
| 5. Lack of patient education and counseling services | |||||
| 13 | Faruqui et al. [ | 2019 | 1. Healthcare system limitations | 1. Complex referral systems and inadequate medical facilities | 1. Navigating multiple medical appointments and tests |
| 2. Economic hardships | 2. Financial burdens due to treatment and associated costs | 2. Struggles with funding treatment and associated travel | |||
| 3. Emotional distress and mental health concerns | 3. Psychological impact on families and caregivers | 3. Stress, anxiety, and helplessness experienced by caregivers | |||
| 14 | Jayakumar al., [ | 2019 | 1. Sociocultural norms | 1. Gender roles in healthcare decisions | 1. Need for male accompaniment |
| 2. Economic constraints | 2. Financial barriers to seeking treatment | 2. Cost of private healthcare | |||
| 3. Healthcare accessibility | 3. Distance to healthcare facilities | 3. Travel difficulties | |||
| 4. Perception of care quality | 4. Distrust in government hospitals | 4. Long wait times at government facilities | |||
| 15 | Kung et al. [ | 2019 | 1. Lack of knowledge and awareness | 1. Misunderstanding about cervical cancer and its screening | 1. Information gap |
| 2. Fear and apprehension toward screening | 2. Fear of screening procedure and results | 2. Anxiety about medical procedures | |||
| 3. Limited family and social support | 3. Lack of encouragement or assistance from family | 3. Absence or indifference of family support | |||
| 16 | Holloway et al. [ | 2020 | Barriers to diagnostic utilization | 1. Navigational challenges | 1. Inadequate infrastructure for diagnostics |
| 2. Delays and necessity for return visits | 2. Lack of point-of-care testing | ||||
| 3. Cost of diagnostic tests | 3. Economic feasibility concerns for patients and hospitals | ||||
| 4. Additional expenses (travel and lost wages) | 4. Economic barriers for the poorest families | ||||
| 5. Balancing healthcare needs with work and household responsibilities | |||||
| 6. Navigational challenges for uneducated or illiterate caregivers | |||||
| 7. Perceptions about the necessity of diagnostics | |||||
| 8. Prioritizing symptomatic treatment over diagnostic tests | |||||
| 17 | George et al. [ | 2020 | 1. Knowledge and awareness gaps | 1. Marginalization of indigenous practices | 1. Disregard for traditional medicine and lack of culturally respectful care |
| 2. Centralization of healthcare | 2. Fear and mistrust | 2. Fear of hospitalization and mistrust in modern healthcare | |||
| 3. Discrimination and Stigma | 3. Accessibility challenges | 3. Travel difficulties and overcrowded central hospitals | |||
| 4. Limited community empowerment | 4. Bias in healthcare provision | 4. Discriminatory attitudes and unconscious bias | |||
| 5. Socioeconomic challenges | 5. Exclusion from policy making | 5. Lack of genuine involvement and tokenistic inclusion | |||
| 6. Land rights and livelihood | 6. Loss of traditional lands and impact on nutrition and health | ||||
| 18 | Raizada et al. [ | 2020 | 1. Diagnostic delays | 1. Complexity of TB diagnosis in children | 1. Multiple healthcare provider visits before diagnosis |
| 2. Socioeconomic challenges | 2. Costs associated with healthcare seeking | 2. Financial burden of TB treatment | |||
| 3. Stigma and social isolation | 3. Fear of social ostracization | 3. Families hiding the TB diagnosis to avoid stigma | |||
| 19 | Kathrikolly et al. [ | 2020 | 1. Sociocultural constraints | 1. Cultural inhibitions | 1. Fear and stigma related to cancer |
| 2. Economic challenges | 2. Financial burden | 2. Financial constraints for screening | |||
| 3. Health system limitations | 3. Infrastructure gaps | 3. Accessibility issues of mammogram centers | |||
| 4. Presence of male health workers as a deterrent | |||||
| 20 | Boro et al. [ | 2020 | 1. Affordability | 1. Direct and indirect costs | 1. Economic hardship |
| 2. Quality of care | 2. Availability of healthcare providers | 2. High treatment costs | |||
| 3. Infrastructure and accessibility | 3. Interpersonal care quality | 3. Transportation costs | |||
| 4. Cultural and educational influences | 4. Medicine and equipment availability | 4. Doctor availability | |||
| 5. Traditional medicine preference | 5. Long waiting times | ||||
| 6. Educational limitations | 6. Disrespectful treatment | ||||
| 7. Geographical barriers | 7. Lack of essential drugs | ||||
| 8. Government and institutional support | 8. Diagnostic services | ||||
| 9. Educational gaps | |||||
| 10. Distance challenges | |||||
| 11. Overburdened facilities | |||||
| 12. Noncompliance and misconceptions | |||||
| 21 | Santalahti et al. [ | 2020 | 1. Financial constraints | 1. Unsteady employment | 1. Daily wage dependency |
| 2. Structural and accessibility issues | 2. High medical costs | 2. Lack of savings, debt for medical expenses | |||
| 3. Social and cultural barriers | 3. Lack of awareness about health services | 3. Unfamiliarity with healthcare system | |||
| 4. Policy and documentation challenges | 4. Distance to health facilities | 4. Transportation challenges | |||
| 5. Work-related limitations | 5. Discrimination in healthcare settings | 5. Prejudice against migrants | |||
| 6. Language barriers | 6. Communication difficulties due to language | ||||
| 7. Low education levels leading to unawareness or misconceptions | 7. Inability to present identification | ||||
| 8. Lack of proper documentation | 8. Exclusion from government health schemes | ||||
| 9. Inflexible work hours | 9. No time off for medical visits | ||||
| 22 | Wood et al. [ | 2020 | 1. Stigma | 1. Societal stigma toward mental health | 1. Instances of community resistance |
| 2. Resource limitations | 2. Lack of resources and support | 2. Challenges in patient engagement | |||
| 3. Role ambiguity | 3. Lack of professional recognition | 3. Feelings of isolation and burnout among healthcare workers | |||
| 23 | Mukerji et al. [ | 2020 | 1. Systemic healthcare challenges | 1. Inadequate healthcare infrastructure | 1. Overcrowded clinics |
| 2. Sociocultural factors | 2. Stigma and privacy concerns | 2. Fear of social exclusion | |||
| 3. Economic constraints | 3. Direct and indirect costs of treatment | 3. Transportation and nutritional costs | |||
| 24 | Faruqui et al. [ | 2020 | 1. Systemic healthcare limitations | 1. Inadequate public health facilities | 1. Resource scarcity in public hospitals |
| 2. Socioeconomic constraints | 2. Financial burden on families | 2. Out-of-pocket expenses for treatment | |||
| 3. Cultural and societal influences | 3. Stigma and lack of awareness | 3. Misconceptions about cancer treatment | |||
| 25 | Dsouza et al. [ | 2020 | 1. Sociocultural stigmas and beliefs | 1. Cultural resistance to modern healthcare | 1. Misconceptions about diseases and treatments |
| 2. Systemic and organizational challenges | 2. Inadequate health infrastructure and staffing | 2. Long waiting times and lack of privacy | |||
| 3. Individual perceptions and fear | 3. Fear of diagnosis and treatment | 3. Anxiety regarding medical procedures | |||
| 26 | Vijayan et al. [ | 2021 | 1. Staff shortage and workload | 1. Operational challenges due to staff shortage | 1. Staffing issues |
| 2. Lack of awareness among the population | 2. Public unawareness of certain health services | 2. Public knowledge gaps | |||
| 3. Shortage of medicines | 3. Disruptions in medicine supply affecting chronic disease management | 3. Medicine availability | |||
| 27 | Kulkarni et al. [ | 2021 | 1. Social stigma and discrimination | 1. Societal attitudes | 1. Stigmatization in public facilities |
| 2. Financial challenges | 2. Economic hardships | 2. Fear of discrimination from healthcare providers | |||
| 3. Mental health concerns | 3. Psychological barriers | 3. Need to hide identity | |||
| 4. Systemic and structural issues | 4. Healthcare system limitations | 4. Poverty | |||
| 5. Personal beliefs and attitudes | 5. Individual perceptions | 5. Lack of stable income | |||
| 6. Financial prioritization away from health | |||||
| 7. Depression | |||||
| 8. Emotional distress | |||||
| 9. Impact on health-seeking behavior | |||||
| 10. Lack of gender-neutral facilities | |||||
| 11. Language barriers | |||||
| 12. Legal and documentation challenges | |||||
| 13. Myths and superstitions | |||||
| 14. Fear of seeking healthcare | |||||
| 28 | Pati et al. [ | 2021 | 1. Systemic challenges | 1. Infrastructure and logistics | 1. Irregular medicine supply |
| 2. Physician-related barriers | 2. Management of records and documentation | 2. Poor laboratory services | |||
| 3. Patient-related factors | 3. Lack of formal training and skills | 3. Lack of skilled support staff | |||
| 4. High patient density and inadequate time | 4. Overreliance on self-education through the internet and pharmaceutical companies | ||||
| 5. Socioeconomic status | 5. Communication difficulties with patients | ||||
| 6. Treatment adherence | 6. Mistrust in government-supplied medicines | ||||
| 7. Noncompliance with treatment plans due to traditional beliefs | |||||
| 29 | Adsul et al. [ | 2022 | 1. Cultural stigma | 1. Sociocultural barriers to discussing gynecologic health | 1. Women’s health as a low priority |
| 2. Resource limitations | 2. Women’s autonomy in healthcare decisions | 2. Inadequate training for cervical cancer screening among physicians | |||
| 3. Lack of awareness | 3. Costs related to healthcare access | 3. Misconceptions about screening | |||
| 4. Community myths and fears about cancer | |||||
| 30 | Wani et al. [ | 2022 | 1. Resource constraints | 1. Inadequate staffing | 1. Untrained staff |
| 2. Lack of awareness | 2. Limited awareness among healthcare workers | 2. Knowledge gap | |||
| 3. Medicine shortage | |||||
| 31 | Thiagesan et al. [ | 2022 | 1. Accessibility challenges | 1. Poor physical access to healthcare facilities | 1. Dependency on others for daily activities |
| 2. Treatment compliance difficulties | 2. Difficulties in adopting recommended dietary and physical activity changes | 2. Inaccessibility of higher-level healthcare facilities for annual screenings | |||
| 3. Lack of tailored health guidelines | 3. Lack of standardized guidelines for diabetes management in persons with disabilities | 3. Healthcare providers' reliance on medication prescription due to the inability to offer comprehensive care | |||
| 32 | Mohanraj et al. [ | 2022 | 1. Inadequate health infrastructure | 1. Lack of essential drugs and medical equipment | 1. Equipment and drug shortages |
| 2. Community practices and perceptions | 2. Insufficient healthcare personnel | 2. Staff shortages | |||
| 3. Skill deficits among health workers | 3. Delayed care-seeking behavior | 3. Poor community awareness | |||
| 4. Preference for local unqualified providers due to accessibility and trust issues | 4. Reliance on unqualified providers | ||||
| 5. Insufficient knowledge and skills among CHWs and paramedical staff | 5. Lack of training for community health workers | ||||
| 6. Lack of regular updates and refresher training for health workers | 6. Supervision gaps for health workers | ||||
| 33 | Rajbangshi et al. [ | 2022 | 1. Limited healthcare accessibility | 1. Transportation difficulties to health facilities | 1. High cost of private transportation for medical care |
| 2. Financial constraints | 2. Cost of medical care and lack of funds | 2. Inability to afford health services costs | |||
| 3. Knowledge and awareness gaps | 3. Lack of awareness about comprehensive health services | 3. Lack of knowledge about government health schemes and broader contraceptive options | |||
| 4. Discrimination and cultural barriers | 4. Language and cultural disconnect with healthcare providers | 4. Language barriers impeding communication with healthcare workers | |||
| 5. Challenges in healthcare provider attitudes | 5. Perceived discrimination by healthcare providers | ||||
| 6. Reluctance of health providers to serve displaced populations | |||||
| 7. Poor reach of public health insurance schemes in displaced communities | |||||
| 8. Challenges in opening bank accounts for receiving health scheme benefits | |||||
| 34 | Cáceres et al. [ | 2023 | 1. Economic constraints | 1. Affordability of services | 1. Cost of care |
| 2. Sociocultural factors | 2. Gender norms | 2. Women's autonomy | |||
| 3. Systemic issues | 3. Staff attitudes | 3. Discrimination by healthcare workers | |||
| 35 | Bangar et al. [ | 2023 | 1. Societal stigma and discrimination | 1. Fear of exposure and societal backlash | 1. Non-recognition of MSM identity in healthcare |
| 2. Invisibility of MSM in healthcare | 2. Inadequate healthcare services for MSM | 2. Inadequate information and education on HIV | |||
| 3. Lack of awareness and misconceptions about HIV | 3. Denial of self-risk for HIV among MSM | 3. Cultural and homophobic barriers | |||
| 4. Programmatic gaps in healthcare services | 4. Poor quality of government health facilities | 4. Dissatisfaction with government healthcare services | |||
| 36 | Saha et al. [ | 2023 | 1. Lack of transportation facilities | 1. Damaged roads and absence of reliable transport | 1. Road damage and isolation |
| 2. Nonfunctional subcenters | 2. Subcenters lacking basic facilities and healthcare personnel | 2. Inadequate healthcare facilities | |||
| 3. Financial constraints | 3. Economic hardships affecting healthcare access | 3. Economic inability to afford care | |||
| 4. Poor infrastructure and inaccessibility during floods | 4. Increased health risks due to flood conditions | 4. Waterborne diseases and lack of sanitation |
| Barrier themes | Verbatim quotes |
| Specific staffing gaps [ | This identified barrier code points to the lack of specialized healthcare personnel in certain areas, affecting service quality and patient outcomes. It indicates a need for targeted training and recruitment strategies. In a study [ |
| Specific infrastructural deficits [ | Identifies physical inadequacies within healthcare facilities that can impede service delivery. It emphasizes the need for investment in healthcare infrastructure to provide a conducive environment for patient care. In a study [ |
| Lack of counseling sessions [ | Reveals a gap in providing mental health support and patient counseling, which is integral to comprehensive healthcare. It suggests a need for integrating mental health services into routine care. Participants from rural areas in a study[ |
| Medicine availability and items frequently out of stock [ | The highest frequency of occurrence indicates a critical issue with essential medicine supply, highlighting challenges in procurement, distribution, and inventory management in healthcare facilities. Logistical hurdles in maintaining medical supplies hinder healthcare provision, necessitating improved supply chain management. Physicians in Odisha emphasized medicine unavailability as a significant barrier [ |
| Public knowledge gaps [ | Indicates a lack of health literacy and awareness among the public, which can lead to delays in seeking care or mismanagement of health conditions. It stresses the need for public health education initiatives. An example of the lack of awareness (about HIV) in a study [ |
| Staffing issues [ | Reflects systemic problems related to the workforce in healthcare, such as inadequate staff numbers, training, or burnout. It indicates that addressing human resource challenges is vital for healthcare delivery. In one of the studies [ |
| Case studies of referral management [ | Notable issues in patient transfers between care levels highlight the necessity for improved coordination and communication within the healthcare system. Lack of coordination between lower and higher care levels was evident, with patients often referred without lower-level management. Inefficient referral mechanisms contributed to excessive patient loads at higher care levels. One of the doctors in the study [ |
| Expressions of staff dissatisfaction [ | This code emphasizes workplace challenges contributing to demotivation and turnover among healthcare workers. It underscores the importance of better working conditions and job satisfaction to uphold service quality, including addressing privacy violations such as inadequate examination spaces and the presence of male providers in maternity wards [ |
| Instances of blood bank failures [ | This highlights critical deficiencies in blood supply management, with potentially life-threatening consequences. It stresses the necessity of robust systems for blood collection, testing, storage, and distribution. A qualitative study [ |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHealthcare Systems and Reforms · Global Maternal and Child Health · Global Health Care Issues
Introduction and background
Access to quality healthcare is a fundamental right, encompassing timely access to personalized services for optimal health outcomes [1]. With the adoption of the 2030 Sustainable Development Goals (SDGs), achieving Universal Health Coverage (UHC) became a global target, aiming for comprehensive healthcare access regardless of financial constraints [2].
India's healthcare reality is marked by a complex interplay of public and private sectors, collectively serving the diverse needs of the nation [3]. Government-run facilities aim to provide affordable care, while the private sector offers a spectrum of services, albeit often at varying costs [4]. Primary health centers, community health centers, and district hospitals are predominantly managed by the government, whereas the private sector, constituting 62% of India's health infrastructure, spans from high-end facilities to community clinics [5].
Despite strides, challenges persist, especially in rural areas where infrastructure, personnel, and medicine supply pose hurdles. Moreover, while the private sector fosters innovation, financial barriers limit access for many [6].
Significant differences in availability, accessibility, and utilization are revealed by India's healthcare system, which has a complex triple structure comprising government, private, and voluntary health agencies [7]. Overcrowding, outdated infrastructure, and staff shortages that erode patient trust are common problems in the state-run public sector, which is frequently beset by management deficiencies, manpower shortages, and a lack of accountability [7].
On the other hand, the private sector, which is favored by about 70% of the population, is mainly unregulated, leading to high fees and significant out-of-pocket (OOP) costs [8]. Interestingly, there are almost twice as many private hospitals in India as there are public ones. The glaring urban-rural divide makes these problems worse. About 80% of healthcare professionals and roughly 75% of health infrastructure are concentrated in urban areas, which is why the majority of people living in rural areas are underserved [9]. They are forced to travel long and difficult distances. India does not meet its own government standards as it has 16% fewer primary health centers and roughly 50% fewer community health centers than required. These draw attention to important gaps in the accessibility and availability of high-quality healthcare [9].
Understanding factors influencing healthcare-seeking behaviors is crucial for crafting responsive systems. This research delves into facilitators and barriers to accessing and utilizing government or private healthcare in India, aiming to inform policy formulation and service enhancement. By synthesizing insights from qualitative studies, it seeks to unravel complexities beyond statistical trends and foster a healthcare landscape that caters to India's diverse needs. We aimed to explore the facilitators and barriers to accessing and utilizing government or private healthcare in India from the available literature using a metasynthesis approach.
Review
Methodology
Study Design
We conducted this metasynthesis to generate evidence on facilitators and barriers in accessing and utilizing government or private healthcare services in India. We prospectively registered the protocol for this review with the International Prospective Register of Systematic Reviews (PROSPERO; Identifier: CRD42024530024).
Databases and Search Strategy
We developed database-specific search strategies for identifying records from PubMed, Scopus, Embase, and Google Scholar (Appendices). We used keywords such as "facilitators," "utilization," "barriers," "India," and appropriate Boolean operators. The "PECOS" (Population, Exposure, Comparator, and Outcome) structure was used to formulate a research question: "What are the primary facilitators and barriers of accessing government or private healthcare facilities in India, as identified through qualitative studies?”
Inclusion and Exclusion Criteria
*Inclusion criteria: *We included qualitative studies or mixed-method studies that reported facilitators and/or barriers related to accessibility and/or utilization of government and/or private healthcare facilities in India. We included studies published in the period of 2013-2023 in the English language.
*Exclusion criteria: *We excluded studies with only a quantitative analysis, studies conducted outside India, and studies that reported the utilization and/or accessibility of a specific type of healthcare service, such as noncommunicable disease, human immunodeficiency virus (HIV), and anemia.
Identification and Selection of Studies
We rigorously identified and removed duplicate articles from our included studies manually. Titles and abstracts were screened for relevance by two independent reviewers. Full-text reviews were then conducted by two independent reviewers. Adjudication was done by one of the senior researchers in case of conflicts.
Risk of Bias Assessment
We used the Critical Appraisal Skills Programme (CASP) Qualitative Checklist to assess the quality of the included studies regarding potential bias (Appendices). Two independent reviewers assessed quality of each of the studies. Any disagreements were resolved through adjudication by another reviewer [10].
Data Extraction
Two researchers independently extracted relevant data using a predesigned Microsoft Excel sheet (Microsoft Corp., Redmond, WA). We extracted the themes, subthemes, and codes related to barriers and facilitators from the included studies. Two reviewers independently extracted the data using a structured data extraction format, followed by verification by another reviewer.
Data Cleaning and Integrity Check
We took a really close look at our dataset to make sure it was complete and accurate. We did not find any missing information, which means the data is high-quality and reliable. This thorough check ensures we can use it for our detailed analysis without needing to fill in any gaps or make corrections.
Data Analysis
Content analysis was conducted using R software (R Foundation for Statistical Computing, Vienna, Austria), identifying the common themes reported in the included studies. Text mining techniques were used to scrutinize word frequencies and co-occurrences. We identified quotes related to the common themes. We generated word clouds based on themes, subthemes, and codes related to barriers and facilitators using NVivo software (Lumivero, Burlington, Massachusetts). The interrelationship between facilitators and barriers influencing healthcare access and utilization was depicted using a network graph, constructed using R software, applying the tidyverse, dplyr, igraph, and ggraph packages. Codes related to facilitators and barriers alongside weights representing the relative prominence or frequency of each thematic linkage were processed to create two essential components: a nodes dataset, containing unique facilitator and barrier codes with attributes identifying their type, and an edges dataset, defining the thematic relationships and their weights.
A Fruchterman-Reingold force-directed layout was applied to the graph to minimize node overlap, ensuring clear clustering of related themes. Nodes were color-coded, with facilitators rendered in soft green and barriers in soft red, while edge thickness and opacity were scaled according to the strength of association. A Sankey diagram was generated to illustrate the directional flow between facilitators and barriers identified in the metasynthesis. Using networkD3 and htmlwidgets in R, facilitators were aligned on the left side of the visualization (depicted in blue), while barriers were aligned on the right side (depicted in red). Links, or ribbons, connected facilitators to barriers, with link width proportional to the weight of their thematic connection. While the network graph shows relationships and clustering, the Sankey diagram emphasizes directionality of thematic influence by establishing a directional flow, visualizing prominence, and identifying recurrent facilitator and barrier interactions.
Results
Search Strategy and Study Selection
A comprehensive electronic database search across PubMed, Embase, Google Scholar, and Scopus initially yielded 3771 articles. Manual searches were conducted on reference lists of pertinent articles and systematic reviews to enhance the search strategy. After removing duplicates and screening titles/abstracts, 73 articles were selected for full-text review. Of these, 36 qualitative studies met eligibility criteria for inclusion in the systematic review. The PRISMA flowchart illustrates the study selection process (Figure 1).
PRISMA flow diagram showing the study selection procedure Only the first 1000 articles were selected.*
Baseline Characteristics of Included Studies
Each of the included studies utilized qualitative research methodologies to examine the facilitators and barriers related to accessing and utilizing healthcare facilities in India. Qualitative methods included interviews [11-39], focus group discussions [13-15,26,34,35,37,40-42], surveys [43], semistructured questionnaires [43-45], and participant observations [11-13,22]. Various sampling techniques were employed in this systematic review to capture diverse perspectives and experiences of individuals accessing healthcare services. Sampling methods ranged from purposive sampling [11,17,19,20,22,25,28,29,30-38,42,43,45], where participants were selected based on specific criteria relevant to the research question, to snowball sampling [18,24,46], where participants were recruited through referrals from initial participants. Additionally, convenience sampling was utilized, selecting participants based on their accessibility and willingness to participate. Participants encompassed a broad spectrum of demographics, including individuals from urban and rural settings, diverse socioeconomic backgrounds, different age groups, and various ethnic or cultural identities. The included studies spanned diverse regions in India, reflecting differences in healthcare infrastructure, government and private facilities, cultural norms, and socioeconomic factors (Table 1).
Key Findings
Facilitators of accessing and utilizing government and private healthcare facilities in India: Notable themes include care accessibility, facility cleanliness, information sharing, and staff behavior. The frequency of specific subthemes like communication clarity and physical access ease underscored their significance in patient care and healthcare delivery, indicating their critical role in service utilization (Table 2).
Predominant Themes and Codes
The analysis revealed 10 central themes impacting healthcare access and utilization (Table 3).
Verbatim quotes (along with brief explanations) representing various facilitators are presented under the most frequently occurring codes and prominent themes (Table 4).
The key codes are depicted in the word cloud. The main words getting repeated are "awareness," "treatment," "encouragement," etc. (Appendices).
Barriers to Accessing and Utilizing Government and Private Healthcare Facilities in India
Barriers uncovered that influenced individuals' ability to access and utilize healthcare services included a shortage of manpower and equipment, poor transport, and cultural norms (Table 5).
Predominant Themes and Codes
The study pinpointed key barriers to healthcare utilization in India, with systemic challenges being the most prevalent, followed by physician-related and patient-related barriers. Verbatim quotes along with brief explanations representing various barriers are presented under the most frequently occurring and prominent codes identified during the detailed analysis (Table 6).
The keywords identified from codes related to barriers in accessing healthcare are depicted in the word cloud. The main words getting repeated are "lack," "cost," "knowledge," etc. (Appendices).
Metasynthesis: Network Analysis
Facilitators such as improved awareness of health entitlements were closely linked to barriers such as confusion around eligibility or operational hurdles. These overlaps highlight a critical point: progress in one area, such as spreading information, may fall short if broader systemic challenges, like administrative efficiency or policy clarity, are not addressed at the same time (Figure 2).
Network diagram showing the interaction between facilitators and barriers (themes and subthemes)
Metasynthesis: Sankey Plot
The left column of the diagram represents prominent facilitator themes such as accessibility of care, health system support, community engagement, professional development, and availability of resources. These were derived from consistent patterns noted across the dataset, wherein respondents emphasized the presence of infrastructure, supportive staff, and localized outreach efforts as critical enablers of access. The right column depicts major barrier themes, including financial constraints, cultural norms, mistrust in providers, systemic inadequacies, and logistical gaps - barriers that emerged recurrently within interviews, focus groups, and ethnographic observations reported in the included studies (Figure 3).
Sankey plot showing interaction between facilitators and barrier themes
Discussion
This systematic review delves into healthcare access and utilization in India, identifying critical facilitators such as staff-patient interactions, information sharing, cleanliness, and accessibility. Positive interactions and informed decision-making are pivotal for improving healthcare utilization, necessitating targeted policies to enhance these aspects comprehensively. This review also identified geographically accessibility, difficult transportation options, and a lack of communication and staff training as barriers to healthcare access and utilization in India.
Different lower-middle-income countries face similar challenges in healthcare utilization, where the infrastructure development and presence of trained human resources for health act as key hindrances to healthcare service accessibility and utilization [47,48]. The progress of different countries toward achieving "Health for All" has ensured a certain progress in overcoming those barriers [49].
The interventions are already working by enhancing communication skills training for healthcare providers to ensure clear and patient-centered information sharing. There is also a requirement for community engagement by means of strengthening community outreach programs and collaborating with local leaders to improve healthcare awareness and navigation assistance. It should be coupled with financial accessibility in the form of expanding health insurance coverage and subsidy programs, especially for low-income populations [50,51].
The review proposes several recommendations based on network analysis, such as health literacy investment by implementing health literacy initiatives, particularly community-specific ones, to empower patients, promote healthcare system engagement, and dispel misconceptions. There should be an analysis of patient barriers to suggest improvements in referral processes, infrastructure, or targeted healthcare provider training. There should be integrated interventions addressing the complexity of healthcare access through holistic solutions, considering both staff shortages and patient mistrust due to inadequate health education.
Acknowledging the limitations of qualitative studies, future research employing mixed-methods approaches and diverse geographical coverage is recommended to provide a comprehensive understanding of access disparities. Additionally, evaluating the impact of recent government healthcare initiatives, such as Ayushman Bharat, through similar techniques could offer valuable insights into policy effectiveness.
Conclusions
This review navigates the multifaceted landscape of healthcare access in India, emphasizing the need for comprehensive strategies to address identified themes. This review identified critical facilitators such as staff-patient interactions, information sharing, cleanliness, and accessibility. This identified geographically accessibility, difficult transportation options, and a lack of communication and staff training as barriers to healthcare access and utilization in India.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Access to Health Care in America Access to Health Care in America. Washington (DC) Institute of Medicine (US) Committee on Monitoring Access to Personal Health Care Services 22Washington (DC)National Academies Press (US)2358901993 https://www.ncbi.nlm.nih.gov/books/NBK 235890/
- 2Universal health coverage (UHC) 5 2024 22024 https://www.who.int/news-room/fact-sheets/detail/universal-health-coverage-(uhc)
- 3The transformation of the Indian healthcare system Cureus Kumar A 015202310.7759/cureus.39079 PMC 1029203237378105 · doi ↗ · pubmed ↗
- 4Comparative performance of private and public healthcare systems in low- and middle-income countries: a systematic review P Lo S Med Basu S Andrews J Kishore S Panjabi R Stuckler D 09201210.1371/journal.pmed.1001244 PMC 337860922723748 · doi ↗ · pubmed ↗
- 5Private healthcare in India: boons and banes 5 2024 Institut Montaigne[Internet 2022 https://www.institutmontaigne.org/en/expressions/private-healthcare-india-boons-and-banes
- 6Challenges to healthcare in India - the five A's Indian J Community Med Kasthuri A 1411434320183029407510.4103/ijcm.IJCM_194_18PMC 6166510 · doi ↗ · pubmed ↗
- 7Women's healthcare access: assessing the household, logistic and facility-level barriers in India BMC Health Serv Res Pradhan MR De P 3232520254001677510.1186/s 12913-025-12463-9PMC 11866841 · doi ↗ · pubmed ↗
- 8Barriers and facilitators to accessing health services: a qualitative study amongst people with disabilities in Cameroon and India Int J Environ Res Public Health Zuurmond M Mactaggart I Kannuri N Murthy G Oye JE Polack S 11261620193093481310.3390/ijerph 16071126 PMC 6480147 · doi ↗ · pubmed ↗