Diagnostic Performance of Magnifying Endoscopy With Crystal Violet Staining for Superficial Non‐ampullary Duodenal Epithelial Tumors: A Single‐center Prospective Study
Tomo Kumei, Yosuke Toya, Shun Yamada, Makoto Eizuka, Shunichi Yanai, Masaki Endo, Ryo Sugimoto, Noriyuki Uesugi, Tamotsu Sugai, Naoki Yanagawa, Fumiaki Takahashi, Takayuki Matsumoto

TL;DR
This study shows that using magnifying endoscopy with crystal violet staining improves the accuracy of diagnosing certain duodenal tumors compared to traditional methods.
Contribution
The study introduces a new algorithm using magnifying endoscopy with crystal violet staining for diagnosing superficial non-ampullary duodenal tumors.
Findings
The ME-CV algorithm showed significantly higher sensitivity (62.5%) compared to WLE (43.8%) in distinguishing tumor categories.
The ME-CV algorithm had a higher negative predictive value (90.2%) compared to WLE (87.3%).
Inter-observer agreement was good for both the WLE scoring system and the ME-CV algorithm.
Abstract
We previously reported a potential diagnostic algorithm for superficial non‐ampullary duodenal epithelial tumors (SNADETs) using white‐light magnifying endoscopy with crystal violet staining (ME‐CV). This study aimed to determine the diagnostic performance of the scheme and compare it with the conventional white‐light endoscopy (WLE) scoring system in a prospectively accumulated cohort. This was a single‐center prospective cohort study conducted over a 3‐year period. The primary endpoint was the diagnostic performance of ME‐CV in distinguishing Vienna classification (VCL) category 4/5 (C4/5) from category 3 (C3) SNADETs, including the positive predictive value (PPV) and negative predictive value (NPV), as evaluated by two expert endoscopists. We compared the diagnostic performance of the WLE and ME‐CV algorithms. Fifty patients with SNADETs were enrolled. The inter‐observer agreement…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
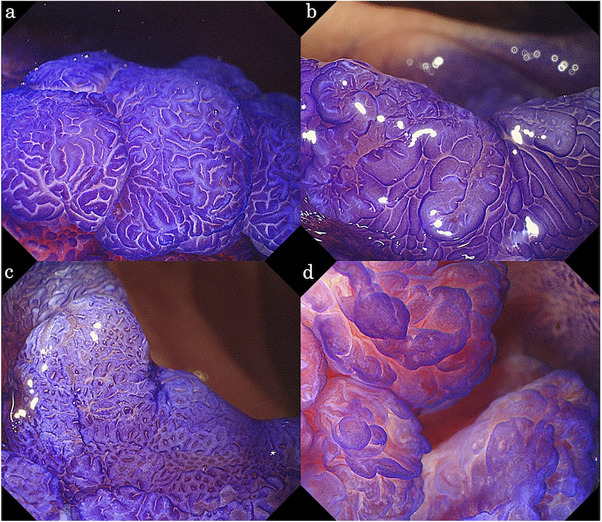 FIGURE 1
FIGURE 1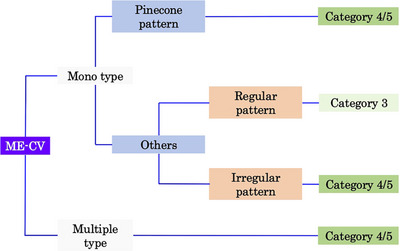 FIGURE 2
FIGURE 2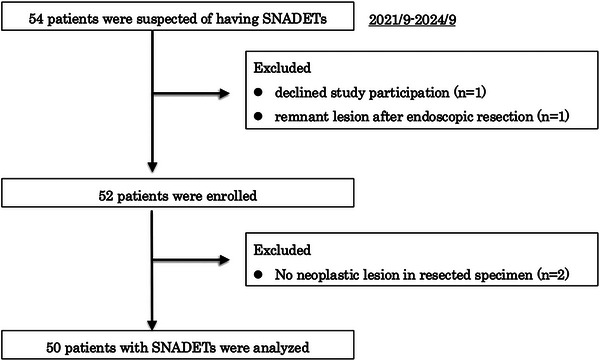 FIGURE 3
FIGURE 3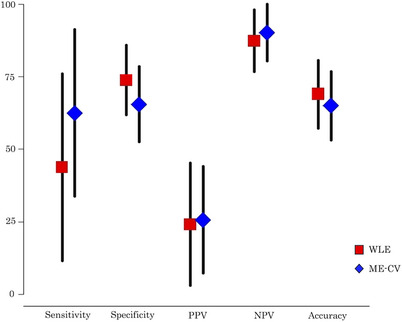 FIGURE 4
FIGURE 4| Endoscopic finding | Score | ||
|---|---|---|---|
| 0 | 1 | 2 | |
| Lesion diameter | <10 mm | ≥10 mm | |
| Color | White | Isochromatic | Red |
| Macroscopic type | Is, Ip, IIa without depression | Any type with depression or mixed type | |
| Nodularity | Uniform | Heterogeneous or none | |
| Variable | |
|---|---|
| Age, years, median (IQR) | 70 (60–75) |
| Sex, | |
| Male | 32 (64.0) |
| Female | 18 (36.0) |
| Tumor location, | |
| Oral side of the papilla of Vater | 33 (66.0) |
| Anal side of the papilla of Vater | 17 (34.0) |
| Tumor size, mm, median (IQR) | 8.5 (5.8–14.0) |
| Macroscopic appearance, | |
| Elevated type | 41 (82.0) |
| Depressed or Mixed type | 9 (18.0) |
| Therapeutic method, | |
| Endoscopic resection (EMR or ESD) | 48 (96.0) |
| Surgery | 2 (4.0) |
| VCL, | |
| Category 3 | 42 (84.0) |
| Category 4/5 | 8 (16.0) |
| Mucin phenotype, | |
| Gastric type | 8 (16.0) |
| Gastrointestinal type | 17 (34.0) |
| Intestinal type | 25 (50.0) |
| WLE scoring system | ME‐CV | |||||
|---|---|---|---|---|---|---|
| Expert 1 | C3 | C4/5 | total | C3 | C4/5 | total |
| VCL | ||||||
| C3 | 30 | 12 | 42 | 24 | 18 | 42 |
| C4/5 | 4 | 4 | 8 | 3 | 5 | 8 |
| total | 34 | 16 | 50 | 27 | 23 | 50 |
| Modality | Sensitivity% (95% CI) |
| Specificity% (95% CI) |
|
|
|
|
| Accuracy% (95% CI) |
|
|---|---|---|---|---|---|---|---|---|---|---|
| WLE | 43.8 (11.6–75.9) | 0.029 | 73.8 (61.8–85.8) | 0.18 | 24.1 (3.1–45.2) | 0.78 | 87.3 (76.7–98.0) | 0.20 | 69.0 (57.3–80.7) | 0.48 |
| ME‐CV | 62.5 (33.8–91.2) | 65.5 (52.5–78.5) | 25.6 (7.3–44.0) | 90.2 (80.5–99.9) | 65.0 (53.2–76.8) |
| Modality | Sensitivity% (95% CI) |
|
|
|
|
| NPV % (95% CI) |
| Accuracy% (95%CI) |
|
|---|---|---|---|---|---|---|---|---|---|---|
| WLE (non‐expert) | 43.8 (16.7–70.8) | 1.0 | 69.1 (56.7–81.4) | 0.31 | 21.2 (3.6–38.8) | 0.63 | 86.6 (75.9–97.2) | 0.77 | 65.0 (53.5–76.5) | 0.37 |
| WLE (expert) | 43.8 (11.6–75.9) | 73.8 (61.8–85.8) | 24.1 (3.1–45.2) | 87.3 (76.7–98.0) | 69.0 (57.3–80.7) | |||||
|
ME‐CV (non‐expert) | 68.8 (39.1–98.4) | 0.29 | 59.5 (49.0–70.1) | 0.36 | 24.4 (7.7–41.2) | 0.76 | 90.9 (80.7–101.1) | 0.68 | 61.0 (50.9–71.1) | 0.48 |
|
ME‐CV (expert) | 62.5 (33.8–91.2) | 65.5 (52.5–78.5) | 25.6 (7.3–44.0) | 90.2 (80.5–99.9) | 65.0 (53.2–76.8) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGastrointestinal Tumor Research and Treatment · Gastric Cancer Management and Outcomes · Pancreatic and Hepatic Oncology Research
Introduction
1
Superficial nonampullary duodenal tumors (SNADETs) are relatively rare [1]. However, it has recently been reported that the incidence of duodenal cancer in Japan is higher than that in Western countries [2]. More recently, the first Japanese guideline for the treatment of duodenal cancer has been published [3]. The guideline recommends endoscopic treatment for adenomas or duodenal cancers that are restricted to the mucosal layer. However, they do not mention the choice of the method of endoscopic resection (ER), presumably because of insufficient evidence in relation to SNADETs.
The efficacy and safety of novel ER methods for SNADETs, such as cold snare polypectomy (CSP) [4, 5] and underwater endoscopic mucosal resection (UEMR) [6, 7], have been reported. A recent randomized controlled trial demonstrated that UEMR was superior to CSP with respect to vertical resectability [8], suggesting that UEMR should be chosen for lesions with suspected submucosal involvement, whereas CSP is preferable for most small SNADETs. For large SNADETs, the treatment options include piecemeal EMR, endoscopic submucosal dissection (ESD), and surgical resection. Although ESD has high en bloc resection rates and favorable local resectability, it remains technically challenging [9, 10]. Accordingly, treatment strategies are currently determined at each institution based on factors such as lesion size and histological atypia.
Therefore, the preoperative endoscopic diagnosis of SNADETs, particularly the distinction of high‐grade adenoma/carcinoma (Vienna classification [VCL] category 4/5, [VCL C4/5]) from low‐grade adenoma (VCL category 3, [VCL C3]) [9, 11] is inevitable for the selection of an appropriate treatment method. However, a widely accepted algorithm for the endoscopic diagnosis of SNADETs has not yet been established [12].
We previously analyzed the findings obtained by magnifying endoscopy with crystal violet staining (ME‐CV) for SNADETs and proposed a diagnostic algorithm applicable to the distinction of VCL C4/5 from VCL C3 [13, 14, 15]. However, there seems to be a need for a prospective study to confirm the algorithm because our previous studies were retrospective. Furthermore, no prospective study has examined the accuracy of the endoscopic diagnosis of SNADETs. Therefore, we conducted a prospective cohort study to clarify the diagnostic performance of ME‐CV for SNADETs in comparison to white‐light endoscopy (WLE).
Methods
2
Study Design
2.1
This was a prospective cohort study conducted at Iwate Medical University from September 2021 to September 2024. The study protocol was approved by the Institutional Review Board of Iwate Medical University (No. MH2021‐077) and registered in the University Hospital Medical Network Clinical Trials Registry (UMIN000044679).
Patients
2.2
Consecutive patients referred to our hospital for the treatment of SNADETs or those diagnosed with SNADETs at our hospital during the study period were assessed for eligibility. The inclusion criteria were as follows: 1) patients suspected of having SNADETs by endoscopy, 2) ≥20 years of age at the time of enrollment, and 3) fully informed written consent for participation in the study (the patient or their surrogate). Bioptic confirmation of SNADETs was not an inclusion criterion. The exclusion criteria were 1) a diagnosis of familial adenomatous polyposis, 2) a remnant lesion after ER, and 3) patients deemed inappropriate for enrollment by the attending physician for other reasons. All patients provided their written informed consent to participate in the study.
Evaluation for Endoscopic Image of SNADETs
2.3
Each SNADET was observed under WLE conditions and subsequently evaluated using ME‐CV (GIF‐H290Z, Olympus, Tokyo, Japan). Tumor size was measured using an endoscopic measuring forceps (M2‐3U; Olympus, Tokyo, Japan). The ME‐CV findings were obtained in accordance with our previous reports. After spraying 0.05% crystal violet solution, endoscopic images were obtained at various magnifications with a maximum magnification of ×85. All endoscopic procedures were performed by an expert endoscopist (Yosuke Toya) and were recorded as videos for subsequent review. The endoscopic videos were reviewed in a blinded post hoc review by two experts (Shun Yamada and Masaki Endo) and two non‐experts (Tomo Kumei and Shun Yamada), with all prospectively collected cases, according to the study protocol.
The WLE images were assessed using the scoring system proposed by Kakushima et al. [16]. The system consists of endoscopic lesion size, color, macroscopic type, and nodularity (Table 1). A total score of ≥3 points was set as the cut‐off value for predicting VCL C4/5. The ME‐CV images were evaluated using a diagnostic algorithm for SNADETs. We have previously reported that the surface features of SNADETs under ME‐CV can be classified into convoluted, leaf‐like, reticular/sulciolar, and pinecone patterns (Figure 1) [13, 14]. Surface ME‐CV patterns were classified into pinecone, irregular, multiplicity, and monotonous patterns. The pinecone, irregular, and multiplicity patterns were regarded as suggestive of VCL C4/5, and the monotonous pattern as VCL C3 (Figure 2) [15].
**TABLE 1: White light endoscopy scoring system.[
14
]**
Endoscopic images of magnifying endoscopy with crystal violet staining (ME‐CV). (a) Convoluted pattern. (b) Leaf‐like pattern. (c) Reticular/sulciolar pattern. (d) Pinecone pattern.
The magnifying endoscopy with crystal violet staining (ME‐CV) algorithm for superficial non‐ampullary duodenal epithelial tumors (SNADETs). Monotypes with a pinecone pattern according to the ME‐CV were classified as Vienna classification category 4/5. Except for the pinecone pattern, monotypes with a regular pattern were classified as category 3. Monotypes with irregular and multiple‐type surface patterns were classified as category 4/5.
Pathological Examinations
2.4
All lesions were removed via ER or surgery and processed for pathological evaluations. Each lesion was graded histologically according to the VCL as C3 (low‐grade adenoma/dysplasia) or C4/5 (mucosal high‐grade neoplasia/submucosal carcinoma invasion) [9]. Immunohistochemical examinations were conducted using an autoimmunostaining system (Dako EnVision System, Denmark). Based on our previous report [14], the gastric type was defined as a phenotype positive for gastric markers only (MUC5AC and MUC6). Similarly, the intestinal type was defined as a phenotype that was positive for intestinal markers only (MUC2 and CD10). Tumors positive for both gastric and intestinal markers were regarded as a gastrointestinal type. All histological evaluations were performed by at least two of the four participating pathologists (Ryo Sugimoto, Noriyuki Uesugi, Tamotsu Sugai, and Naoki Yanagawa). Each pathologist independently assessed the specimens, and the final diagnoses were determined through discussion until a consensus was reached.
Outcomes
2.5
The primary endpoint was the diagnostic performance of the ME‐CV algorithm, including the positive predictive value (PPV) and negative predictive value (NPV), evaluated by two expert endoscopists. The expert endoscopists were board‐certified members of the Japanese Gastroenterological Endoscopy Society. The secondary endpoints included a comparison of the diagnostic performance, including sensitivity, specificity, PPV, NPV, and accuracy, between the WLE scoring system and the ME‐CV algorithm, a comparison of the diagnostic performance between the expert endoscopists and the non‐expert endoscopists, and the interobserver agreement for the WLE scoring system and the ME‐CV algorithm. In addition, we calculated the diagnostic performance of the combined use of WLE and ME‐CV, classifying lesions as VCL 4/5 when both methods indicated VCL 4/5.
Sample Size
2.6
Our previous study revealed that the diagnostic performances of the ME‐CV algorithm for distinguishing VCL C3 from C4/5 were as follows: sensitivity, 63.6%; specificity, 85.2%; PPV, 63.6%; NPV, 85.1% [14]. Assuming a PPV of 70% and a 30% prevalence of VCL C4/5, the required sample size was calculated using a normal approximation to ensure that the lower limit of the one‐sided 95% confidence interval (CI) for the PPV exceeded 50%. Consequently, the target sample size for this study was set at 50.
Statistical Analysis
2.7
Continuous variables were expressed as the median and interquartile range (IQR), and categorical variables were expressed as the number (%). The diagnostic performance of the WLE scoring system and ME‐CV algorithm, along with comparisons of the diagnostic performance among endoscopic methods and between experts and non‐experts, was analyzed using generalized estimating equations. In each analysis, p‐values of <0.05 were considered statistically significant. To evaluate the reproducibility of the endoscopic findings, the inter‐observer agreement for each lesion was calculated using a kappa analysis. All statistical data were analyzed using SAS (ver. 9.4; SAS Institute Inc., Cary, NC, USA). All statistical analyses were performed by an independent biostatistician (Fumiaki Takahashi).
Results
3
During the study period, 54 patients suspected of having SNADETs were recruited. After the exclusion of one patient who declined study participation and another with a remnant lesion after ER, 52 patients were enrolled. Two additional patients were excluded due to the absence of a neoplastic lesion in the resected specimen, leaving 50 patients for the final analyses (Figure 3).
Patient flow in this study.
The clinical characteristics of the patients are shown in Table 2. The median age was 70 years, with a male predominance (64.0%). The lesions were more frequently located on the oral side of the papilla of Vater (66.0%), with a median tumor size of 8.5 mm. A total of 41 lesions (82.0%) were of the elevated type, and most (96%) were treated with ER. Based on the VCL, 42 lesions (84%) were classified as VCL C3, and eight lesions (16.0%) were classified as VCL C4/5. Immunohistochemistry revealed 8 gastric type lesions (16.0%), 17 gastrointestinal type lesions (34.0%), and 25 intestinal type lesions (50%).
Table 3 shows the diagnostic values of the WLE and ME‐CV algorithms for the expert and non‐expert endoscopists. The PPV and NPV of the ME‐CV algorithm by the expert endoscopists were 25.6% and 90.2%, respectively. The diagnostic performance of the WLE and the ME‐CV algorithms by the expert endoscopists is summarized in Figure 4 and Table 4. The sensitivity, specificity, PPV, NPV, and accuracy of the WLE scoring system were 43.8%, 73.8%, 24.1%, 87.3%, and 69.0%, respectively. The sensitivity, specificity, and accuracy of the ME‐CV algorithm were 62.5%, 65.5%, and 65.0%, respectively. When the diagnostic performance was compared between the WLE scoring system and the ME‐CV algorithm, the sensitivity was significantly higher in the latter than in the former (43.8% vs 62.5%; p = 0.029), whereas other diagnostic test results did not differ between the two procedures.
Diagnostic performance of the white light endoscopy (WLE) scoring system and the magnifying endoscopy with crystal violet staining (ME‐CV) algorithm by expert endoscopists.
Table 5 shows the diagnostic performance of the WLE and the ME‐CV algorithms for the expert and non‐expert endoscopists. The diagnostic test results for both procedures did not differ between expert and non‐expert endoscopists.
For experts, diagnostic accuracy differed between WLE and the combined use of WLE and ME‐CV. The diagnosis of VCL 4/5 by a combination of both WLE and ME‐CV showed higher specificity (80.9% vs 73.8%; p = 0.027), PPV (30.4% vs 24.1%; p = 0.03), and accuracy (75.0% vs 69%; p = 0.009) in comparison to WLE alone (Table S1).
The inter‐observer agreement between the two expert endoscopists was found to be good in the WLE scoring system (kappa value: 0.66) and in the ME‐CV algorithm (kappa value: 0.63). In contrast, the agreements between the non‐experts remained moderate (kappa value: 0.51 for the WLE scoring system, and 0.22 for the ME‐CV algorithm).
Discussion
4
A standard method for the endoscopic diagnosis of SNADETs remains to be fully established. Furthermore, most studies to date have reported on the value of endoscopy for the prediction of the histological grade of atypia in SNADETs and are retrospective in nature. To the best of our knowledge, this is the first prospective study to assess the diagnostic test value of ME‐CV in SNADETs. Our results demonstrated that the ME‐CV algorithm had significantly higher sensitivity than the WLE scoring system for distinguishing VCL C4/5 from VCL C3 SNADETs.
Several studies have reported on the use of magnifying image‐enhanced endoscopy (IEE) to diagnose the histological grade of SNADETs [12]. As an image‐enhancement tool, most reports have applied narrow‐band imaging (ME‐NBI) to target SNADETs, and the diagnostic test results ranged from 76% to 95.8% for sensitivity, from 53.4% to 97.4% for specificity, and from 65.1% to 96.8% for accuracy [17, 18, 19, 20]. In previous studies, an irregular micro surface pattern (MSP) or a combination of MSPs, rather than an irregular microvascular pattern (MVP), was preferentially used to indicate VCL C4/5. The lower diagnostic value of MVP has been explained by the obscured visualization of vasculature under NBI due to the prominent white opaque substance (WOS) in SNADETs^12^. Therefore, it seems reasonable to focus on the MSP for the diagnosis of SNADETs. Although less convenient than IEE, we believe that ME‐CV is another useful procedure to focus on the MSP of SNADETs. While previous studies have reported high overall diagnostic performance with ME‐NBI when compared to our ME‐CV results, such a difference may partly be a consequence of variations among study designs and the limited number of subjects in our study. A prospective head‐to‐head comparison between ME‐CV and ME‐NBI is warranted to clarify their relative diagnostic value.
We found that our ME‐CV algorithm was characterized by significantly higher sensitivity than the WLE scoring system for distinguishing VLC4/5 from VCL C3 in SNADETs. In contrast, there were no significant differences in the specificity, PPV, or NPV. This finding highlights a potential trade‐off in diagnostic yield. Although ME‐CV provides higher sensitivity than WLE and may help to reduce missed diagnoses of VLC4/5, its relatively lower specificity could increase the risk of false‐positive findings. Such a trend may result in unnecessary additional biopsies or ERs, raising the possibility of overtreatment. Therefore, the clinical application of ME‐CV should carefully balance these advantages and limitations.
A recent meta‐analysis reported that summary estimates of sensitivity, specificity, and area under the curve (AUC) for the endoscopic diagnosis of VCL4/5 were 80%, 80%, and 0.859, respectively, for WLE and 72%, 76%, and 0.811 for ME‐NBI [21]. These findings suggest that WLE may have comprehensive diagnostic potential for identifying severe atypia in SNADETs. In addition, a meta‐analysis showed that the combination of WLE and ME‐NBI yielded the highest sensitivity, specificity, and AUC values (88%, 87%, and 0.929, respectively) for the diagnosis of VCL4/5. Our results also showed a trend towards better diagnostic performance when the WLE and ME‐CV were combined, although this study was not designed to evaluate the diagnostic performance of the combination. Further investigation is warranted to establish and evaluate endoscopic diagnostic approaches that combine WLE and ME‐CV.
Our results did not show a significant difference in the diagnostic performance between the expert and the non‐expert groups for either WLE or ME‐CV. However, the kappa value for ME‐CV was extremely low in the non‐expert group (0.22). This observation suggests that the ME‐CV algorithm requires a certain level of proficiency and learning for the magnifying observation of gastric and colorectal lesions. Further studies are warranted to evaluate the impact of the learning curve on the accuracy of the ME‐CV algorithm in the diagnosis of SNADETs.
The present study had several limitations. First, it was a single‐center study. Since the attending endoscopists had experience in observing ME‐CV findings prior to the present study, they might have too much experience to generalize our findings worldwide. Second, the PPVs for both WLE and ME‐CV in this study were much lower than those reported in a previous retrospective study. This may be partly explained by the smaller number of VCL C4/5 SNADETs than initially anticipated. In addition, the small number of VCL 4/5 lesions may represent a potential limitation in terms of the statistical power. Thus, it is necessary to validate our findings in a larger‐scale, multicenter, prospective study. Third, the number of cases in each subgroup of the mucin phenotype was too small to conduct a reliable statistical analysis of the diagnostic performance. Finally, and most importantly, it should be noted that CV is recognized as a potent carcinogen in mammalian cells [22]. However, there is currently no evidence to suggest that exposure to extremely small topical amounts of CV increases the risk of malignant neoplasms.
In conclusion, the ME‐CV algorithm had significantly higher sensitivity than the WLE scoring system for distinguishing VCL4/5 from VCL C3 in SNADETs. Our ME‐CV algorithm may contribute to the diagnosis of VCL C4/5 lesions and the selection of an appropriate ER for SNADETs.
Author Contributions
Tomo Kumei: conceptualization, data curation, investigation, and writing ‐ original draft preparation. Yosuke Toya: conceptualization, data curation, formal analysis, investigation, methodology, and writing ‐ original draft preparation. Shun Yamada: data curation and writing ‐ review & editing. Makoto Eizuka: data curation and writing ‐ review & editing. Shunichi Yanai: data curation and writing ‐ review & editing. Masaki Endo: conceptualization and writing ‐ review & editing. Ryo Sugimoto: investigation and writing ‐ review & editing. Noriyuki Uesugi: investigation and writing ‐ review & editing. Tamotsu Sugai: investigation and writing ‐ review & editing. Naoki Yanagawa: investigation and writing ‐ review & editing. Fumiaki Takahashi: formal analysis and writing ‐ review & editing. Takayuki Matsumoto: supervision and writing ‐ review & editing. All authors have read and approved the final version of the manuscript.
Conflicts of Interest
Yosuke Toya is the associate editor of DEN Open. Takayuki Matsumoto is a faculty member at the Japanese Society of Gastrointestinal Endoscopy. Fumiaki Takahashi is the associate editor of Digestive Endoscopy. The other authors declare no conflicts of interest.
Ethics Statement
Approval of the research protocol by an institutional review board: The study protocol was approved by the institutional review board of Iwate Medical University (No. MH2021‐077).
Consent
All patients provided written informed consent for study participation.
Clinical Trial Registration
This study was registered with the University Hospital Medical Network Clinical Trials Registry (UMIN000044679).
Supporting information
Table S1: Diagnostic performance of the combination of the WLE scoring system and the ME‐CV algorithm by expert endoscopists.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1M. Endo , Y. Abiko , S. Oana , et al., “Usefulness of Endoscopic Treatment for Duodenal Adenoma,” Digestive Endoscopy 22 (2010): 360–365.21175499 10.1111/j.1443-1661.2010.01014.x · doi ↗ · pubmed ↗
- 2N. Kakushima , D. Ohki , Y. Miura , et al., “The Incidence of Nonampullary Duodenal Cancer in Japan 2016–2020: Analysis of a National Cancer Registry,” Journal of Gastroenterology and Hepatology 39 (2024): 2672–2676.39377433 10.1111/jgh.16766 PMC 11660200 · doi ↗ · pubmed ↗
- 3K. Nakagawa , M. Sho , M. Fujishiro , et al., “Clinical Practice Guidelines for Duodenal Cancer 2021,” Journal of Gastroenterology 57 (2022): 927–941.36260172 10.1007/s 00535-022-01919-y PMC 9663352 · doi ↗ · pubmed ↗
- 4K. Takizawa , N. Kakushima , M. Tanaka , et al., “Cold Snare Polypectomy for Superficial Nonampullary Duodenal Epithelial Tumor: A Prospective Clinical Trial (pilot study),” Surgical Endoscopy 36 (2022): 5217–5223.34859300 10.1007/s 00464-021-08899-9 · doi ↗ · pubmed ↗
- 5K. Okimoto , D. Maruoka , T. Matsumura , et al., “Long‐term Outcomes of Cold Snare Polypectomy for Superficial Non‐ampullary Duodenal Epithelial Tumors,” Journal of Gastroenterology and Hepatology 37 (2022): 75–80.34409657 10.1111/jgh.15666 · doi ↗ · pubmed ↗
- 6Y. Toya , M. Endo , M. Yamazato , et al., “Resectability of Underwater Endoscopic Mucosal Resection for Duodenal Tumor: A Single‐center, Retrospective Pilot Study,” Journal of Gastroenterology and Hepatology 36 (2021): 3191–3195.34318532 10.1111/jgh.15638 · doi ↗ · pubmed ↗
- 7Y. Yamasaki , N. Uedo , T. Akamatsu , et al., “Nonrecurrence Rate of Underwater EMR for ≤20‐mm Nonampullary Duodenal Adenomas: A Multicenter Prospective Study (D‐UEMR Study),” Clinical Gastroenterology and Hepatology 20 (2022): 1010–1018.34217879 10.1016/j.cgh.2021.06.043 · doi ↗ · pubmed ↗
- 8K. Miyazaki , A. Nakayama , M. Sasaki , et al., “Resectability of Small Duodenal Tumors: A Randomized Controlled Trial Comparing Underwater Endoscopic Mucosal Resection and Cold Snare Polypectomy,” American Journal of Gastroenterology 119 (2024): 856–863.38131610 10.14309/ajg.0000000000002634 · doi ↗ · pubmed ↗