Only the strong survive: therapeutic selective pressure drives medulloblastoma leptomeningeal metastasis
Francis Y. He, Adrienne Boire

TL;DR
Radiation therapy for medulloblastoma can cause inflammation and spread of cancer to the leptomeninges, but dexamethasone can reduce this effect.
Contribution
The study reveals that radiation-induced inflammation and blood-brain barrier breakdown drive metastasis, and dexamethasone can mitigate this process.
Findings
Radiation therapy increases myeloid cell infiltration and cytokine levels, promoting leptomeningeal metastasis.
Dexamethasone cotreatment reduces cytokines and preserves blood-brain barrier integrity, limiting metastasis.
Targeting inflammation can decrease the overall disease burden in medulloblastoma patients.
Abstract
Medulloblastoma (MB) is the most common malignant tumor in the central nervous system in childhood and regularly metastasizes to the leptomeninges following radiation therapy. Using patient‐derived medulloblastoma models and genetically engineered mouse models, Nör et al. observed enhanced inflammation and infiltration of myeloid cells within the brain following irradiation. The authors identified inflammatory cytokines and the resulting breakdown of blood–brain barriers as the main culprits of MB leptomeningeal metastasis. This study demonstrated that targeting inflammation through the use of dexamethasone effectively reduced systemic inflammatory cytokines and the resulting radiation‐induced leptomeningeal metastasis. Radiation therapy induces cancer cell death and immune cell infiltration, mainly monocytes, macrophages, and dendritic cells. Elevated serum cytokine levels and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
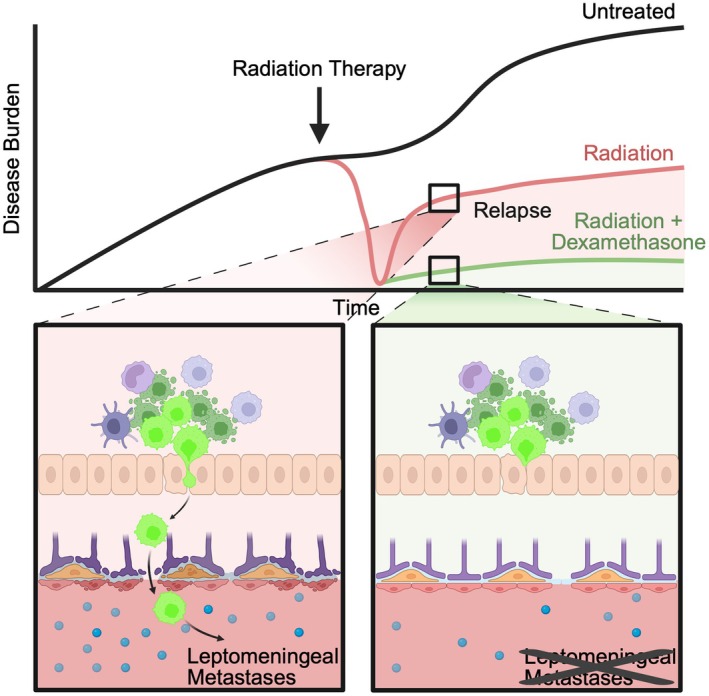 Figure 1
Figure 1 Figure 2
Figure 2- —National Cancer Institute10.13039/100000054
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGlioma Diagnosis and Treatment · Neuroblastoma Research and Treatments · Microtubule and mitosis dynamics
Radiation therapy (RT) has long been a cornerstone of medulloblastoma treatment, introduced to prong survival after surgical resection to counteract local recurrence and metastasis to the leptomeninges, (the pia, arachnoid, and cerebrospinal fluid, CSF). However, irradiation of the central nervous system (CNS) carries substantial side effects and remains a major cause of neurocognitive morbidity in medulloblastoma survivors [1]. Recent work from Nör et al. investigates the unintended consequences of radiation therapy, mechanistically linking this treatment to subsequent leptomeningeal metastasis (LM) [2]. The provocative work raises a critical question in cancer care: Does radiation therapy for medulloblastoma treatment uphold the principle of “do no harm,” or does the treatment select for more aggressive disease?
Surgical resection and radiation remain first line of treatment for medulloblastoma. The authors first evaluated prognosis across multiple clinical trials combining radiation therapy with cytotoxic chemotherapy. Surprisingly, radiation therapy correlated with a significant increase in LM incidence. This was investigated mechanistically in an experimental series employing patient‐derived xenograft models, establishing the causal relationship between RT and the development of LM. Addressing the next question of how this might occur, the authors established how RT reshapes the tumor microenvironment. Within 5 h post irradiation, the cancer cells undergo apoptosis, and bulk RNA‐seq reveals enrichment in immune‐related pathways, particularly those associated with the innate immune response. Complementary single cell RNA‐seq and Cytometry by Time‐Of‐Flight (CyToF) analyses uncovered enrichment in immune cell subpopulations, particularly myeloid populations including monocytes, macrophages, and dendritic cells.
The team next turned their attention to the endothelial compartment. Radiation was found to disrupt tight junction integrity and increase blood–brain barrier (BBB) permeability. Notably, RT also increased the number of circulating tumor cells (CTCs) in peripheral blood in flank xenograft models and elevated serum inflammatory markers (Fig. 1). Previous work by the group reported the presence of CTCs from medulloblastoma into the periphery. These cells, competent to metastasize back into the leptomeninges, rely on the monocyte attractant cytokine CCL2 [3]. Again, the authors find that myeloid‐derived inflammatory cytokines play an instrumental role in leptomeningeal spread. Postulating that radiation‐provoked inflammation might exacerbate metastasis by inducing inflammation, the authors induced inflammation using lipopolysaccharide (LPS), which remarkably phenocopied the prometastatic effects of RT, promoting LM. Conversely, treatment with dexamethasone, a steroid commonly used in the clinical setting, reduced inflammation and blocked LM (Fig. 1).
Medulloblastoma metastasis represents a complex, whole organism process encompassing the tumor‐cell intrinsic features, the local cerebellar microenvironment, the leptomeningeal space, and the systemic circulation. While Nör et al. shed light on the inflammatory consequences of RT, important questions remain. Importantly, can we leverage the potential benefit of immune therapy (provoking inflammation in the space) without incurring increased risk of leptomeningeal spread? Addressing this question will require granular characterization of the antitumor response in the space in comparison with the post RT response. In addition, while the authors beautifully demonstrate increased vascular permeability post RT, does this treatment alter the leptomeningeal niche to support medulloblastoma growth? Might RT promote one aspect of the metastatic cascade and inhibit another? Nör et al. argue that the prometastatic effect of RT is secondary to the influx of immune cells into the CNS, triggered by tumor cell death and the subsequent clearance of cellular debris, a process that inadvertently heightens inflammation [2]. Might similar mechanisms apply for other solid tumors after RT?
As treatments become more efficacious, and patients live longer, the consequences of the selective pressure of treatment on malignancy become more apparent. This has been observed most readily in the case of tumors treated with targeted therapies: In prostate cancer and EGFR‐mutant lung adenocarcinomas, targeted therapies including antiandrogen treatment and EGFR inhibitors are effective at controlling primary disease [4, 5]. However, these treatments favor the emergence of neuroendocrine phenotypes that were vanishingly rare prior to these therapies [6]. In the context of medulloblastoma, increased mutational burden and pathways such as TP53 have emerged following treatment [7, 8]. Nör et al. invite us to consider the possibility that therapies such as RT may exert selective pressure indirectly, through impacting the tumor microenvironment, to select for metastatic cells.
The work also challenges us to consider our use of RT in the treatment of medulloblastoma. RT remains one of the most effective tools for eliminating residual tumor cells and preventing recurrence, particularly in high‐risk, group 3, group 4 patients. The long‐term cost of RT is substantial; neurocognitive impairment, hearing loss, and impaired quality of life are frequently observed among survivors [1]. These adverse effects are common and significantly impact the patient's ability to live an independent life. Thus, proton radiation, RT avoidance, or reduced dose are often preferable for younger patients [9, 10]. Importantly, RT alone does not protect against disease progression, as Nor et al. demonstrate; rather, it shifts the pathology from local recurrence to metastatic disease [2, 7].
These findings underscore the need to examine our approach to the use of RT in medulloblastoma as well as other CNS tumors. RT‐mediated alteration of the local microenvironment may well reprogram both the micro‐ and macroenvironment, leading to organism‐wide changes that alter the biology of these malignancies. This work suggests that assessing response to RT through imaging measures alone likely overlooks important alterations in the local and systemic inflammatory response. These changes are doubtless present in the context of other CNS malignancies. It is time to conduct thoughtful, biopsy‐rich clinical trials to capture local and distal environmental changes resulting from RT so that we may anticipate and 1 day avoid metastatic progression.
Conflict of interest
AB holds an unpaid position on the Scientific Advisory Board for Evren Scientific and is an inventor on the following patents: 62/258044, 10/413522, and 63/052139. FH declares no conflict of interest.
Author contribution
FH and AB conceived and wrote the manuscript.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ramaswamy V , Taylor MD . Medulloblastoma: from myth to molecular. J Clin Oncol. 2017;35(21):2355–2363.28640708 10.1200/JCO.2017.72.7842 · doi ↗ · pubmed ↗
- 2Nör C , Kharas K , Rasnitsyn A , Vladoiu MC , Cho NW , Young JS , et al. Therapeutic radiation drives leptomeningeal dissemination of medulloblastoma through an innate immune process. Dev Cell. 2025;S 1534–S 5807:00371‐5.10.1016/j.devcel.2025.06.016PMC 1310206740609543 · doi ↗ · pubmed ↗
- 3Garzia L , Kijima N , Morrissy AS , de Antonellis P , Guerreiro‐Stucklin A , Holgado BL , et al. A hematogenous route for medulloblastoma leptomeningeal metastases. Cell. 2018;172(5):1050–1062.e 14.29474906 10.1016/j.cell.2018.01.038PMC 6346737 · doi ↗ · pubmed ↗
- 4Chan JM , Zaidi S , Love JR , Zhao JL , Setty M , Wadosky KM , et al. Lineage plasticity in prostate cancer depends on JAK/STAT inflammatory signaling. Science. 2022;377(6611):1180–1191.35981096 10.1126/science.abn 0478 PMC 9653178 · doi ↗ · pubmed ↗
- 5Niederst MJ , Sequist LV , Poirier JT , Mermel CH , Lockerman EL , Garcia AR , et al. RB loss in resistant EGFR mutant lung adenocarcinomas that transform to small‐cell lung cancer. Nat Commun. 2015;6(1):6377.25758528 10.1038/ncomms 7377 PMC 4357281 · doi ↗ · pubmed ↗
- 6Quintanal‐Villalonga Á , Chan JM , Yu HA , Pe’er D , Sawyers CL , Sen T , et al. Lineage plasticity in cancer: a shared pathway of therapeutic resistance. Nat Rev Clin Oncol. 2020;17(6):360–371.32152485 10.1038/s 41571-020-0340-z PMC 7397755 · doi ↗ · pubmed ↗
- 7Morrissy AS , Garzia L , Shih DJH , Zuyderduyn S , Huang X , Skowron P , et al. Divergent clonal selection dominates medulloblastoma at recurrence. Nature. 2016;529(7586):351–357.26760213 10.1038/nature 16478 PMC 4936195 · doi ↗ · pubmed ↗
- 8Wu X , Northcott PA , Dubuc A , Dupuy AJ , Shih DJH , Witt H , et al. Clonal selection drives genetic divergence of metastatic medulloblastoma. Nature. 2012;482(7386):529–533.22343890 10.1038/nature 10825 PMC 3288636 · doi ↗ · pubmed ↗