Reduction of Festinating Clinical Gait Parameters to Near Normal After Hip Joint Mobilization: A Parkinson’s Disease Case Report
Chistopher K Wong, Chelsea E Macpherson

TL;DR
Hip joint mobilization significantly improved gait in a Parkinson's patient, restoring near-normal walking speed and step length.
Contribution
This case report introduces hip joint mobilization as a novel intervention for improving gait in Parkinson's disease.
Findings
Hip joint mobilization led to a 20.4% increase in gait speed to 1.30 m/s.
Step length improved by 30.2%, reaching 0.69 m, and cadence decreased to near-normal levels.
Improvements were maintained for two weeks and allowed the patient to return to tennis.
Abstract
People with Parkinson's disease (PD) walk with decreased speed and step length that worsen with disease progression. Despite treatments that yield statistically significant yet clinically small changes, normal gait parameters are rarely restored. Few PD studies assess joint passive range-of-motion concurrently with temporospatial gait parameters or joint mobilization effects on gait outcomes. This case introduces hip joint mobilizations for passive range of motion in PD and the unusual outcome of temporospatial gait parameters returning to near normal. A male with PD managed consistently pharmacologically presented with bradykinesia, rigidity, and characteristic festinating gait dysfunctions: slow speed, short step lengths, and fast cadence. Bilateral hip passive range of motion was impaired in all planes. He attended only two sessions for hip joint mobilizations and stretching. Hip…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
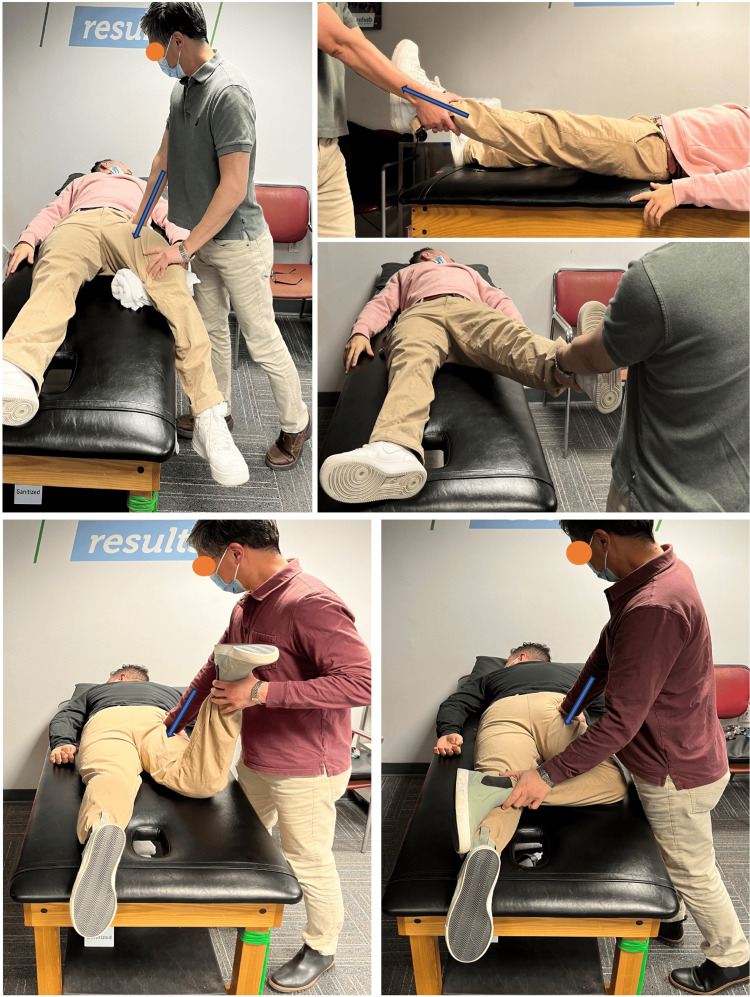 Figure 1
Figure 1| Outcome Measure | Men with PDa | Session 1: pre-treatment | Session 1: post-treatment | Session 2: pre-treatment | Session 2: post-treatment | Men without PD | |
| Bilateral Passive ROM (degrees) | Hip AB | No data | 10 | 25 | 25 | 25 | 39 |
| Hip E | No data | 10 | 10 | 10 | 20 | 7.5 | |
| Hip ER | No data | 30 | 30 | 30 | 50 | 50 – 55 | |
| Gait speed (m/s) | 0.87–1.09 | 1.08 | 1.14 | 1.21 | 1.30 * | 1.38-1.49 | |
| Step length (m) | 0.51-0.63 | 0.53 | 0.71 | 0.60 | 0.69 | 0.71 | |
| Cadence (steps/s) | 1.68–1.73 | 2.05 | 1.60 | 2.00 | 1.90 | 1.89 | |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsParkinson's Disease Mechanisms and Treatments · Parkinson's Disease and Spinal Disorders · Botulinum Toxin and Related Neurological Disorders
Introduction
People with Parkinson's disease (PD), a progressive multi-system disorder [1], display the cardinal signs of rigidity, bradykinesia, postural instability, and gait dysfunction [2]. Festinating PD gait is characterized by short step lengths and slow walking speed with or without altered cadence and freezing-of-gait [3]. Medically managed pharmacologically, the PD physiotherapy Clinical Practice Guidelines (CPG-PD) strongly recommend multi-modal rehabilitation for intertwined physiologic and musculoskeletal impairments with aerobic, resistance, balance, gait, and task-specific training and weakly recommend stretching based on one study [4]. PD movement dysfunction worsens musculoskeletal impairments, while pre-existing musculoskeletal impairments worsen movement dysfunction apparent in temporospatial gait measures [3]. Despite much exercise and movement training research [4], passive joint motions necessary for active movement, treatments to address joint impairments, and concurrent PD gait assessment remain unexplored [5].
No CPG-PD articles examined passive joint range-of-motion impairments [4], which represent the mechanical limit and potential for active movements powered by muscles and observed in gait analysis studies as limited throughout the lower limb [6]. Basal ganglia-brainstem system dysfunction in PD affects muscle tone, active movement, and locomotion via motor neurons that directly innervate muscles, but not joint capsules [7]. Stretching, which requires underlying joint mobility and passive range of motion, can improve muscle flexibility but not PD temporospatial gait parameters [4]. Joint passive range-of-motion, however, is rarely assessed in PD, with just one study showing passive hip range-of-motion minimally increased after 48 exercise sessions [8]. Spinal manipulative studies all lack passive range-of-motion measurements, and no CPG-PD studies explored joint mobilizations with temporospatial gait outcomes [4,5]. This PD case, previously presented as a poster at the American Physical Therapy Association Combined Sections Meeting in February 2023, introduces hip joint mobilizations aimed at increasing the mechanical range of motion available for gait and the unusual outcome of temporospatial gait parameters improved to near age-sex-matched normal at two weeks with a seven-month follow-up.
Case presentation
Informed written consent was obtained, confidentiality rights were preserved, and CARE guidelines were followed, though approval from the participating medical center's institutional review board was not required for this case report. One licensed board-certified orthopedic clinical specialist physiotherapist performed all assessments and treatments. All case data were obtained from the electronic medical record.
The 51-year-old male patient was diagnosed with PD three years earlier when bilateral motor symptoms, bradykinesia, rigidity, freezing-of-gait, and intention tremor became apparent. Dopamine transporter single-photon emission computed tomography imaging confirmed the diagnosis. His pharmacological management included consistent carbidopa/levodopa, rotigotine, and amantadine doses. Despite being in an on state, function declined over six months, and worsening festination prevented participation in his weekly tennis games. He denied pain and walked independently without an assistive device. His only physiotherapy goal was to improve gait to enable return to tennis.
Findings
Evaluation revealed flexed posture, bradykinesia, rigidity, and intention tremor without freezing-of-gait. Gait was slow with short shuffling steps clinically assessed over a 40-meter walkway with one 180-degree turn using a digital stopwatch and manually recorded step counts yielding gait speed (distance/time), step length (distance/steps), and cadence (steps/time). Initial temporospatial gait parameters were comparable to men with PD, with slower speed, shorter steps, and faster cadence than non-PD age-sex-matched peers [9,10] (Table 1). Standard goniometry revealed limited hip passive range of motion and end-range accessory joint hypomobility. Manual muscle tests revealed 4/5 hip strength throughout.
**Table 1: Case data with age-matched normal values for men with and without Parkinson’s disease.AB: Abduction, E: Extension, ER: External Rotation, ROM: Range-of-Motion
- Increase exceeded minimal clinically important difference in Parkinson’s disease.**
Diagnosis
His presentation aligned with the postural instability/gait dysfunction (PIGD) phenotype and Hoehn-Yahr Stage 3 mild to moderate diagnosis, including bradykinesia, rigidity, postural instability, and gait dysfunction [2]. Prognosis, despite consistent medication, was disease progression and functional decline [2]. Even sustained adherence to weekly physiotherapy typically produces small effect size gait speed changes [4]. Gait speed is the product of cadence and step length, which appears 2-dimensional in sagittal plane double support measurements but results from active hip motion to position the limb in all planes (sagittal-extension, frontal-abduction, and transverse-rotation) [11].
Plan of care
The personalized patient-centered physiotherapy care plan focused on reducing gait dysfunction and facilitating lateral frontal plane hip mobility required for return-to-tennis [12,13]. Thus, intervention emphasized maximizing hip joint passive range of motion in all planes to increase active step length potential and gait speed, whether impairment preceded disease onset or resulted from PD muscular rigidity [3]. Since the basal ganglia-brainstem system directly controls muscle rigidity but not joint capsule hypomobility [7], joint mobilizations to optimize passive range of motion were prioritized over muscle flexibility. While people function without full joint range of motion, movement becomes limited and dysfunctional compensations occur, including short step lengths and slow speed that characterize festinating gait [3] (Table 1). Biweekly sessions for eight weeks were planned to reduce joint impairments before progressing to functional exercise and return-to-tennis activities.
Intervention
He attended only two sessions, two weeks apart. The session-1 evaluation included treatment constrained to hip joint mobilizations (~15 minutes) [14] and ~15 minutes of home exercise program education, including lunge stretches to maintain step length: 3-5 repetitions, 30s each (Figure 1). The session-2 reassessment revealed that improved hip passive range of motion and gait parameters were maintained (Table 1). Session-2 treatment included hip joint mobilizations (~15 minutes) [14] and home program education (~15 minutes), adding prone figure-of-four position stretching to maintain new hip abduction and external rotation range-of-motion (3-5 repetitions, 30s each) and encouragement to continue daily walking. While comprehensive care was planned, he discontinued physiotherapy two weeks later because his walking and return-to-tennis goals were met.
Hip joint mobilizations were performed in the case.Top: session-1 hip joint mobilizations to increase abduction: Left) posteriorly directed grade III+ oscillations in supine with hip in slight flexion and abduction for general mobility biased towards abduction and to prepare for thrust. Right) Long axis distraction grade V thrust modified in slight flexion, internal rotation and abduction for frontal plane impact and hip abduction range of motion.Bottom: Session-2 hip joint mobilizations to increase hip extension and external rotation. Left) Anteriorly directed grade III+ oscillations in the prone knee bend position to increase anterior capsule mobility and rectus femoris muscle flexibility for sagittal plane impact and hip extension range-of-motion. Right) Anteriorly directed grade III+ oscillations in the prone figure-of-four position to increase anterior capsule mobility for transverse plane impact and hip external rotation range-of-motion.
Outcomes
From first to last assessment, gait speed increased by 20.4% (0.22 m/s), exceeding the 0.06 m/s minimal clinically important difference (MCID) in PD and indicating an upper-range large effect size change [15]. Improvements occurred within- and between-sessions in hip passive range-of-motion, step length, and gait speed, with all approaching age-sex-matched norms [9,10,16] (Table 1). Cadence decreased 7.3%. Step length increased 30.2% (0.16 m), exceeding the ≤0.08 m statistically significant yet small effect size changes from various non-pharmacologic PD treatments [17]. Visible festination was not apparent upon reassessment, for him, an important clinical outcome. He reported immediate walking improvements and considered his walking goals met, and he achieved his primary return-to-tennis goal after two sessions. At the seven-month follow-up, he walked without visible festination and played tennis regularly, so he declined reassessment and further care.
Discussion
After two sessions emphasizing joint mobilization, this patient had passive hip range-of-motion, gait speed, and step length improvements beyond MCID and common PD treatments [15,17]. Temporospatial gait parameters initially sex-matched for PD were restored to near healthy age-sex-matched norms [9,10,18], a personally significant clinical improvement potentially more impactful than statistically significant small effect size changes. Multiple body systems affect locomotion, but movement is expressed and kinematically measured by musculoskeletal motions. Underlying passive joint hypomobility restricts active musculoskeletal movement and function, and this patient’s 3-plane hip passive range-of-motion impairment restricted gait and tennis-specific lateral movements [3,11,13]. For him, both hip passive range-of-motion and temporospatial signs of festinating gait improved after physiotherapy, emphasizing joint mobilizations, not stretching muscles directly affected by PD basal ganglia-brainstem dysfunction [7].
Multimodal PD rehabilitation includes range-of-motion exercises, yet the clinical practice guideline for Parkinson's disease (CPG-PD) cites none, including joint mobilizations [4]. The three PD spinal manipulative studies lack passive range-of-motion and follow-up temporospatial gait measures [5]. For non-PD neurological diseases, ankle mobilizations show immediate range-of-motion and gait speed improvements [19]. Because ankle, knee, and hip impairments impact gait with distal-to-proximal progression across different PD stages [20], analyzing specific gait-related joint impairments and personalizing PD rehabilitation with targeted joint mobilization may optimize outcomes [12,20].
Case studies cannot determine cause and effect. PD is progressively neurodegenerative despite his consistent pharmacological treatment and independent physical activity before functional decline stopped him from playing tennis, a progression inconsistent with his rapid recovery of near-normal step length and gait speed after two joint mobilization sessions [2]. Gait speed (m/s) increases with longer step lengths (m/step), potentially affected by increased passive hip range-of-motion, assuming similar cadence (step/s) [6]. Mechanisms explaining how mobilizations increase passive joint range-of-motion remain unclear, but passive range-of-motion absent pain does not vary as active range-of-motion does.
Case studies highlight novel approaches and unusual outcomes, prompting future study. PD research incorporating passive joint range-of-motion assessments with temporospatial gait parameters would clarify the relationship between joint impairments and gait dysfunction [5]. Without concurrent assessment, understanding of PD gait dysfunction is incomplete. The one PD study to assess gait and passive hip joint range of motion in an eight-month multi-modal exercise program found minimal single-plane improvement without functional effects [8]. Exercise and functional tasks are constrained by the available passive range of motion, potentially explaining limited functional benefit [8]. Increasing passive joint range of motion to maximize potential active movement before functional exercise training is a logical treatment sequence, warranting investigation.
All case reports lack randomized controlled conditions. Limitations also included a lack of instrumented gait analysis common in research laboratories, though unusual in private clinics, one clinician performing assessments and treatments reflecting real-life clinical practice, and patient-reported long-term follow-up. Freezing-of-gait never occurred, though festination can be episodic. The patient met his goals quickly and thus did not need or complete planned multi-modal care, though without behavioral change, improvement could be short-lived. The two-week between-session carryover and seven-month walking and tennis outcomes were promising, even if longevity remains unknown.
Conclusions
Joint stiffness and limited passive hip range of motion have rarely been studied concurrently with temporospatial gait parameters in people with PD. While the short steps of festinating gait in PD are a well-known phenomenon generally attributed to the neurodegenerative disease course and progressive muscle rigidity, joint capsules are not directly innervated by motor neurons and mechanically limit range-of-motion, thus providing an avenue to gain hip range-of-motion and improve step length and thereby gait speed.
In this PD case, temporospatial parameters typical for festinating gait increased by a large effect size to near age-sex-matched normal after two hip joint mobilization and stretching sessions without pharmacologic changes. While various treatments yield small statistically significant changes in PD gait, restoring gait to near-normal without festination is a novel occurrence with a clinical personal impact. Assessing passive hip range-of-motion with temporospatial gait parameters in controlled PD trials of joint mobilization is warranted.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Parkinson's disease as a multisystem disorder J Neural Transm (Vienna) Klingelhoefer L Reichmann H 70971312420172815513310.1007/s 00702-017-1692-0 · doi ↗ · pubmed ↗
- 2How to identify tremor dominant and postural instability/gait difficulty groups with the movement disorder society unified Parkinson's disease rating scale: comparison with the unified Parkinson's disease rating scale Mov Disord Stebbins GT Goetz CG Burn DJ 6686702820132340850310.1002/mds.25383 · doi ↗ · pubmed ↗
- 3Mechanical energy recovery during walking in patients with Parkinson disease P Lo S One Dipaola M Pavan EE Cattaneo A 011201610.1371/journal.pone.0156420 PMC 489268127258183 · doi ↗ · pubmed ↗
- 4Physical therapist management of Parkinson disease: a clinical practice guideline from the American Physical Therapy Association Phys Ther Osborne JA Botkin R Colon-Semenza C 102202210.1093/ptj/pzab 302PMC 904697034963139 · doi ↗ · pubmed ↗
- 5Effects of manual therapy on Parkinson’s gait: a systematic review Sensors (Basel) Delafontaine A Vialleron T Barbier G 24202410.3390/s 24020354 PMC 1082078638257446 · doi ↗ · pubmed ↗
- 6Gait parameters of Parkinson's disease compared with healthy controls: a systematic review and meta-analysis Sci Rep Zanardi AP da Silva ES Costa RR 7521120213343699310.1038/s 41598-020-80768-2PMC 7804291 · doi ↗ · pubmed ↗
- 7Role of basal ganglia-brainstem systems in the control of postural muscle tone and locomotion Prog Brain Res Takakusaki K Oohinata-Sugimoto J Saitoh K Habaguchi T 23123714320041465316810.1016/S 0079-6123(03)43023-9 · doi ↗ · pubmed ↗
- 8Effects of physical exercise on articular range of motion of the lower limb in the Parkinson's disease individuals Fisioterapia e Pesquisa Barbieri FA Batistela RA Rinaldi NM 167173212014