Acute Kidney Injury: A Blocked Diagnosis
Zhi Tian Chen, Lih Yin Chong, Irushna Perera, Rizuan Mohamed

TL;DR
This case report discusses a challenging diagnosis of acute kidney injury caused by a blocked urinary catheter in an elderly patient.
Contribution
The novelty lies in highlighting how a blocked catheter can cause AKI and how initial imaging may fail to detect the obstruction.
Findings
Initial ultrasound failed to detect obstruction despite clinical suspicion of obstructive uropathy.
CT scan revealed severe hydronephrosis and bilateral hydroureter, confirming the obstruction.
The case emphasizes the need for clinical judgment and advanced imaging in diagnosing AKI.
Abstract
Acute kidney injury (AKI) is a common medical condition that we encounter in our daily clinical practice. However, in certain cases, ascertaining the underlying cause of the AKI could be challenging and requires a thorough history, focused investigations, and a high index of suspicion. We present the case of a 79-year-old gentleman who has been using a long-term urinary catheter and presented with AKI, which we found to be challenging to diagnose. In patients with a history of obstructive uropathy, particularly those using long-term catheters, a blocked catheter is the most probable cause of AKI. In this case, we found it challenging to establish a definitive diagnosis, given that the initial ultrasound scan of the kidneys failed to identify an obstruction. This necessitated broadening our differential diagnoses and resorting to second-line investigations such as a CT scan. As the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
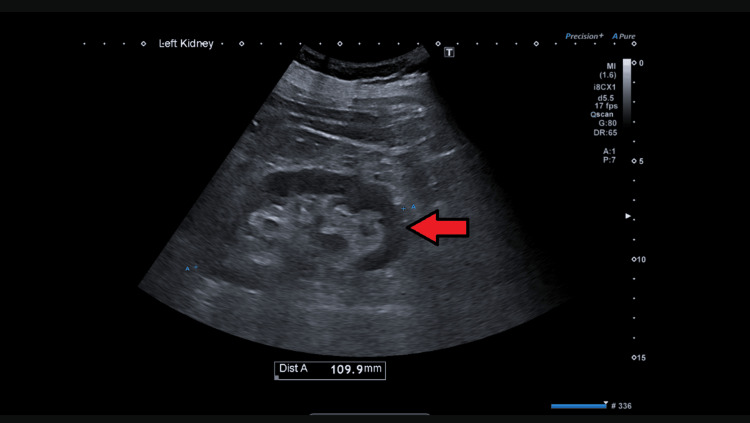 Figure 1
Figure 1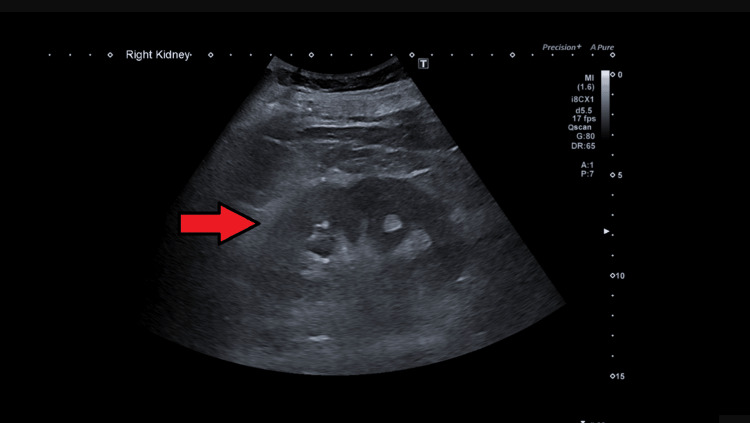 Figure 2
Figure 2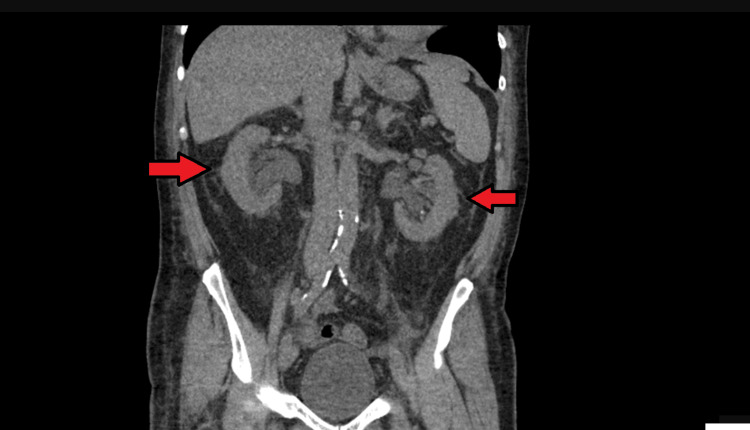 Figure 3
Figure 3| Laboratory test | Date | ||
| 08/12/2024 (Day 1: day of admission) | 10/12/2024 (Day 3) | 12/12/2024 (Day 5) | |
| Sodium (133-146 mmol/L) | 120 | 130* | 130 |
| Potassium (3.5-5.3 mmol/L) | 4 | 3.8 | 3.7 |
| Urea (2.5-7.8 mmol/L) | 23 | 30.3* | 32.4* |
| Creatinine (59-107 umol/L) | 375 | 558* | 618* |
| Hemoglobin (130-180 g/L) | 132 | 108* | |
| White blood cells (4-11x109/L) | 15.3 | 9.6 | |
| Platelets (150-400x109/L) | 90 | 91 | |
| Total bilirubin (0-21 umol/L) | 21 | 38* | |
| CRP (<5 mg/L) | 211 | 155 |
| Fluid chart | Date | ||
| 09/12/2024 | 10/12/2024 | 11/12/2024 (After Tiemann tip insertion) | |
| Input (mL) | 1850 | 1575 | 1800 |
| Output (mL) | 2000 | 476 | *6170 |
| Total (mL) | -150 | 1039 | *-4370 |
| Laboratory test | Date | |
| 12/12/2024 | 13/12/2024 (Date of discharge) | |
| Sodium (133-146 mmol/L) | 141 | 141 |
| Potassium (3.5-5.3 mmol/L) | 3.7 | 4 |
| Urea (2.5-7.8 mmol/L) | *11.9 | *5.8 |
| Creatinine (59-107 umol/L) | *122 | *85 |
| Hemoglobin (130-180 g/L) | 124 | 119 |
| White blood cells (4-11x109/L) | 7.1 | 8.3 |
| Platelets (150-400x109/L) | 197 | 208 |
| Total bilirubin (0-21 umol/L) | 18 | 20 |
| CRP (<5 mg/L) | 30 | |
|
| Negative | |
|
| Negative | |
|
| Negative | |
|
| Negative | |
|
| Negative | |
| Blood film (FBP) | No evidence of hemolysis | |
| Direct antiglobulin | Positive | |
| IgA (0.8-4 g/L) | 1.7 | |
| IgG (6-16 g/L) | 8.3 | |
| IgM (0.5-2 g/L) | 1.6 | |
| Complement C3 (0.9-1.8 g/L) | 1.1 | |
| Complement C4 (0.14-0.54 g/L) | <0.1 | |
| Anti-PLA2R antibody (0-14 kU/L) | <2 | |
| Anti-GBM antibody (7-10 U/mL) | <0.8 | |
| LDH (240-400 U/L) | 369 | |
| Reticulocyte count | ||
| Antinuclear antibody (0.1-0.69) | 0.4 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAcute Kidney Injury Research · Trauma, Hemostasis, Coagulopathy, Resuscitation · Chronic Kidney Disease and Diabetes
Introduction
Acute kidney injury (AKI) is a common medical condition that we encounter in our daily practice. It is defined as an abrupt decrease in kidney function, resulting in the retention of urea and other nitrogenous waste products and in the dysregulation of extracellular volume and electrolytes [1-3]. However, diagnosis and ascertaining the etiology of AKI can sometimes be challenging and not straightforward, especially during on-call periods when stress levels are high and resources are limited. We hereby present a challenging case of AKI in an elderly gentleman on a long-term catheter.
The challenge we faced was determining the cause of the AKI in the face of a rapidly declining kidney function so that corrective treatment could be offered as early as possible. As is the norm, obstructive uropathy was high in our list of differential diagnoses for the AKI, given that he had a history of prostate cancer and was on a long-term catheter. However, the first ultrasound did not show any blockage, so we had to review the patient's history and examination to find other possible reasons for the AKI, such as kidney or pre-kidney issues, even though we still strongly suspected obstructive uropathy.
Case presentation
A 79-year-old gentleman was admitted to our hospital with a blocked long-term urinary catheter. He had his urinary catheter changed twice in the ED over the past few days and has been passing clear urine since then. Notably, a week before this incident, he experienced several episodes of diarrhea during a trip to Norfolk, where he had eaten street food. He described diarrhea as "watery," with no mucus or blood in the stool. Upon admission to the hospital, he exhibited a deranged renal profile indicating Stage 1 AKI.
He is a known hypertensive who is being treated with indapamide and lisinopril, and he also has type 2 diabetes for which he takes alogliptin. He is on treatment for carcinoma of the prostate with 12 weekly leuprorelin injections and is on a long-term catheter. In addition to these medications, he also takes atorvastatin.
Upon examination, he was fully alert and orientated. There was no raised jugular venous pressure, and he appeared euvolemic. His chest was clear, and no heart murmur was appreciated. There was no pedal edema seen. His abdomen was soft, and there was no palpable bladder or renal angle tenderness. His observational chart indicated that his blood pressure ranged from 90 to 100 mmHg. We initially used a differential diagnosis to rule out an obstructive cause of the AKI. We performed several bladder scans on admission, but they did not reveal urinary retention. We also requested a formal ultrasound scan of the abdomen (Figures 1, 2). The ultrasound revealed no evidence of obstruction or stones. Given the history of watery diarrhea, hypotension on examination, high inflammatory markers, and the absence of solid evidence of obstructive uropathy, our next strategy was to believe that a prerenal cause of AKI was the most likely culprit; therefore, we continued rehydration therapy, and we closely monitored his fluids and input and output charts.
Ultrasound of the kidney, ureter, and bladderThere was no significant hydronephrosis seen in the ultrasound. The left kidney measured around 10.9 cm.The red arrowhead indicates preserved corticomedullary differentiations.
Ultrasound of the kidney, ureter, and bladderThere was no significant hydronephrosis seen in the ultrasound.The right kidney measured around 10.6 cm.The red arrowhead indicates preserved corticomedullary differentiations.
Unfortunately, despite aggressive hydration, the renal profile and metabolic acidosis continued to deteriorate alarmingly (Table 1). During the admission, he had his urine catheter changed twice and continued to maintain a satisfactory urine output. We repeated numerous bladder scans; however, they did not show any evidence of urinary retention. On the third day of admission, he developed hypotension that was refractory to fluid resuscitation. Upon reviewing his blood investigations, we noticed that he had newly developed anemia and thrombocytopenia, as well as a mild elevation of bilirubin. Given that he had watery diarrhea before being admitted, our findings made us consider less common conditions such as hemolytic uremic syndrome (HUS) or thrombotic thrombocytopenic purpura (TTP). Upon examining the patient, he was fully alert and oriented; there were no obvious signs of neurological deficit or rash.
Keeping the rare but possible differentials in mind, we subsequently requested an urgent full blood picture, a hemolytic profile, and an autoimmune screen panel. A full blood picture did not show any evidence of hemolysis; other hemolysis workups came back as unremarkable. Despite fluid hydration, the patient continued to be persistently hypotensive. At this point, we decided to revisit our initial diagnosis for this patient, which was obstructive uropathy. It was the most plausible cause given his background of long-term catheter use and prostate carcinoma. Therefore, we requested an urgent CT scan of the kidney, ureter, and bladder in view of the diagnostic dilemma. The CT scan revealed severe hydronephrosis with bilateral moderate hydroureter (Figure 3), a likely obstructive cause of AKI initially missed in the ultrasound scan. We liaised urgently with our urology colleagues, who immediately reviewed the patient. They advised that a Tiemann tip silicone catheter be inserted, as it is very likely that a conventional urinary catheter was draining his bladder completely.
CT renalBilateral arrowheads show evidence of severe hydronephrosis with moderate hydroureter bilaterally, without obvious cause.The kidneys are normal in size with severe hydronephrosis.
After a Tiemann tip urinary catheter was inserted, he drained as much as 6 L of urine (Table 2). Following the procedure, his renal profile and blood parameters significantly improved along with his clinical observations. The renal autoimmune profiles turned out to be unremarkable. The stool sample did not show Escherichia coli or Shiga toxin. After three days, his renal profile reverted back to baseline, his vital signs became stable, and he was discharged on medical advice afterwards (Table 3).
Discussion
Although AKI is a common condition encountered in daily clinical practice, sometimes determining its underlying cause can be challenging, as illustrated by this case presentation. We discussed a 75-year-old male on a long-term urinary catheter who presented to us with AKI [2]. Initially, ruling out an obstructive cause was our main differential diagnosis. However, the initial negative bladder scans, negative formal ultrasound kidney, ureter, and bladder results, and persistent hypotension despite fluid resuscitation led us to consider both pre-renal and renal causes for the AKI [4-6]. Most clinical cases are not as straightforward as in our medical literature, and therefore, we found it quite challenging to determine the exact nature of the AKI.
His worsening renal profile, despite fluid challenges, antibiotics, and supportive management, pushed us to rethink. Is there anything we may have missed? While ultrasound is quite sensitive in identifying hydronephrosis, in certain clinical scenarios, such as early obstructive uropathy, operator dependence, or suboptimal visualization, its sensitivity may be reduced [7]. Therefore, in cases of diagnostic uncertainty and clinical deterioration, with a high degree of suspicion for an obstructive uropathy, a CT scan should be promptly considered to rule out obstruction [8]. This case serves as a reminder that even seemingly routine medical conditions can evolve unpredictably if appropriate treatment is not offered timely.
On the other hand, we should always remain vigilant in thinking of a broader differential diagnosis, even if it is a rare and life-threatening cause. TTP and HUS are rare diseases that both work in a similar way, called thrombotic microangiopathy (TMA). TMA occurs when small blood vessels get blocked with microthrombi, leading to low platelet counts, destruction of red blood cells, and failure of multiple organs [9]. Even though the patient did not show clear signs of organ failure besides AKI or neurological issues, the presence of anemia, low platelet counts, and high bilirubin levels, along with a quick decline in kidney function, made us want to look deeper, since the treatment could be very different and more specific than usual care. For example, we could use plasma exchange or administer biological agents such as eculizumab. The ongoing urosepsis in this case likely contributed to the development of anemia and thrombocytopenia, as well as the elevated bilirubin [10].
With the establishment of an obstructive uropathy, we were able to resort to the most appropriate treatment, which was addressing the bladder outflow obstruction by changing the catheter. However, in this case, even this proved challenging, as the traditional urinary catheter was unable to completely relieve the obstruction. Therefore, with the advice from urology specialists, a Tiemann tip catheter was inserted, relieving the urinary retention. Following this, the blood parameters improved significantly, normalizing within a few days.
Conclusions
This case highlights the importance of maintaining a high index of clinical suspicion in our daily medical practice. While initial history and examination pointed toward an obstructive cause for the AKI, the lack of evidence from the initial sonography made us reconsider other causes of AKI, such as pre-renal and renal causes. The rapid clinical and biochemical deterioration prompted us to broaden our differential diagnoses. Ultimately, further imaging studies and excellent clinical judgement led us to a diagnosis of obstructive uropathy, despite earlier negative imaging.
Additionally, this case teaches us to remain vigilant regarding rare but serious conditions in our practice. A thorough and detailed history, focused clinical examination, and appropriate investigations, along with a high index of clinical suspicion, were the keys to achieving a positive outcome in this complex clinical case.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1A European Renal Best Practice (ERBP) position statement on the Kidney Disease Improving Global Outcomes (KDIGO) clinical practice guidelines on acute kidney injury: part 1: definitions, conservative management and contrast-induced nephropathy Nephrol Dial Transplant 12 2012 Fliser D Laville M Covic A Fouque D Vanholder R Juillard L Van Biesen W 426342722720122304543210.1093/ndt/gfs 375PMC 3520085 · doi ↗ · pubmed ↗
- 2KDIGO clinical practice guidelines for acute kidney injury Nephron Clin Pract 8 2012 Khwaja A 084120201210.1159/00033978922890468 · doi ↗ · pubmed ↗
- 3Acute renal failure Lancet Lameire N Biesen WV Vanholder R 4174309457200510.1016/S 0140-6736(05)17831-315680458 · doi ↗ · pubmed ↗
- 4Renal sonography: can it be used more selectively in the setting of an elevated serum creatinine level?Am J Kidney Dis 3 1997 Gottlieb RH Weinberg EP Rubens DJ 362367291997904121110.1016/s 0272-6386(97)90196-7 · doi ↗ · pubmed ↗
- 5Point-of-care ultrasound for the detection of hydronephrosis in emergency department patients with suspected renal colic Ultrasound J 6 2020 Sibley S Roth N Scott C Rang L White H Sivilotti ML Bruder E 311220203250790510.1186/s 13089-020-00178-3PMC 7276462 · doi ↗ · pubmed ↗
- 6The accuracy of point-of-care ultrasound performed by emergency physicians in detecting hydronephrosis in patients with renal colic Sultan Qaboos Univ Med J 8 2022 Al-Balushi A Al-Shibli A Al-Reesi A 3513562220223607207910.18295/squmj.9.2021.130PMC 9423761 · doi ↗ · pubmed ↗
- 7Diagnostic accuracy of ultrasonography compared to unenhanced CT for stone and obstruction in patients with renal failure BMC Med Imaging Ather MH Jafri AH Sulaiman MN 242004 https://pmc.ncbi.nlm.nih.gov/articles/PMC 514525/1528387010.1186/1471-2342-4-2PMC 514525 · doi ↗ · pubmed ↗
- 8An expert discussion on the atypical hemolytic uremic syndrome nomenclature-identifying a road map to precision: a report of a National Kidney Foundation Working Group Kidney Int Nester CM Feldman DL Burwick R 32633610620243917419210.1016/j.kint.2024.05.021 · doi ↗ · pubmed ↗