Effectiveness of ChAdOx1 nCoV-19 (Vaxzevria) primary series vaccine against SARS-CoV-2 beta and delta variants: a nationwide study
Hiam Chemaitelly, Houssein H. Ayoub, Peter Coyle, Patrick Tang, Mohammad R. Hasan, Hadi M. Yassine, Asmaa A. Al Thani, Zaina Al-Kanaani, Einas Al-Kuwari, Andrew Jeremijenko, Anvar Hassan Kaleeckal, Ali Nizar Latif, Riyazuddin Mohammad Shaik, Hanan F. Abdul-Rahim

TL;DR
This study found that the ChAdOx1 nCoV-19 vaccine was effective against SARS-CoV-2 Beta and Delta variants, with strong protection against severe disease, though protection against infection decreased over time.
Contribution
The study provides real-world evidence of the ChAdOx1 nCoV-19 vaccine's effectiveness against Beta and Delta variants in a large population.
Findings
Two-dose vaccine effectiveness was 66.0% against any infection and 73.0% against symptomatic infection.
Effectiveness against severe, critical, or fatal disease was 100% regardless of variant.
Protection against infection declined to 45.6% after 150 days post-second dose.
Abstract
This study assessed the real-world effectiveness of the ChAdOx1 nCoV-19 vaccine in adults against severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection, symptomatic infection, and severe coronavirus disease 2019 (COVID-19) during periods of Beta and Delta variant dominance in Qatar. A national, matched, test-negative case-control study was conducted using 186,130 PCR-positive tests (cases) and 667,289 PCR-negative tests (controls) collected between January 1 and December 18, 2021. Subgroup analyses were performed to evaluate vaccine effectiveness across key strata. The median time between the first and second doses was 61 days (interquartile range, 56–64 days). Two-dose primary-series effectiveness was 66.0% (95% CI, 55.1–74.3%) against any SARS-CoV-2 infection and 73.0% (95% CI, 44.1–87.0%) against symptomatic infection. Effectiveness was estimated at 100% (95% CI,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
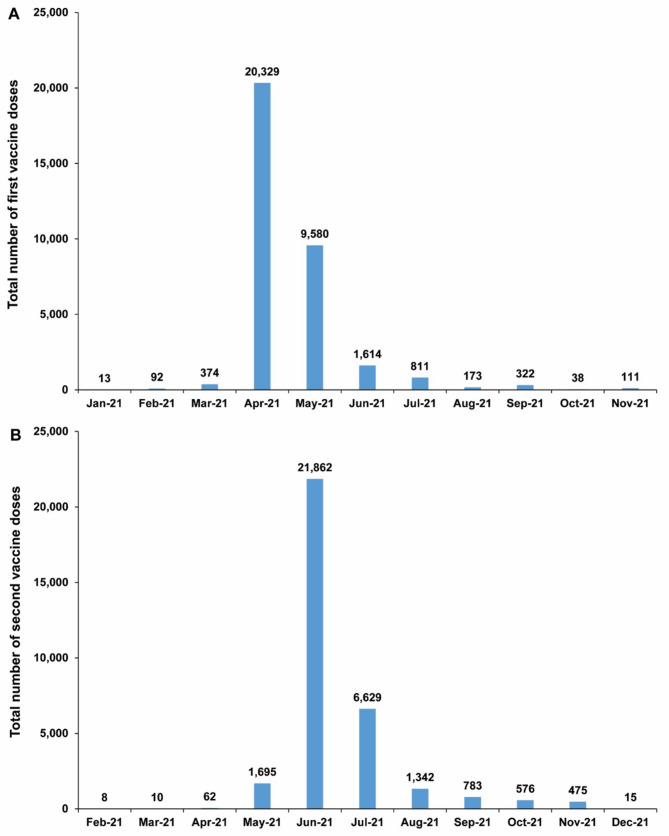 Figure 1
Figure 1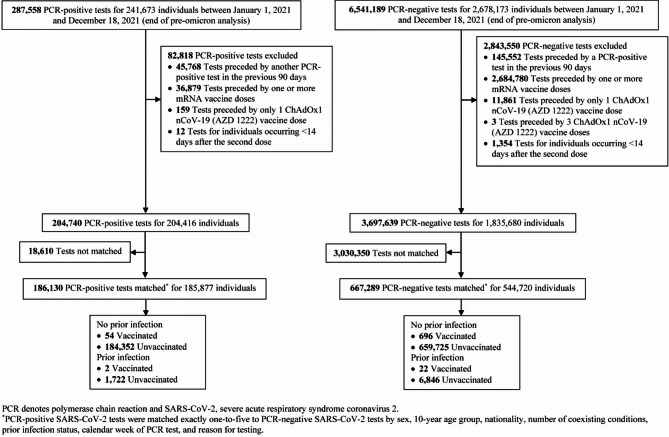 Figure 2
Figure 2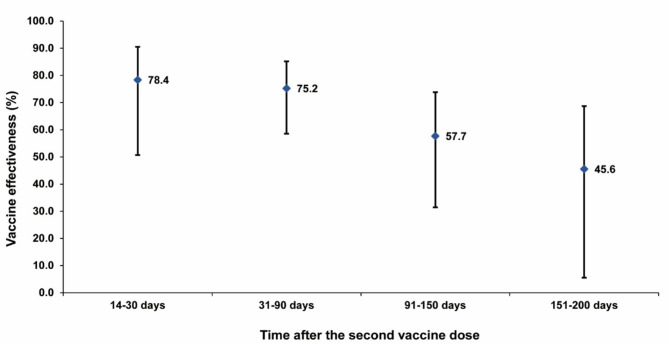 Figure 3
Figure 3- —Qatar Research, Development and Innovation Council
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSARS-CoV-2 and COVID-19 Research · COVID-19 Clinical Research Studies · SARS-CoV-2 detection and testing
Introduction
Multiple vaccines were developed to reduce the acquisition and severity of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection [1]. While mRNA-based vaccines demonstrated high efficacy [2, 3], their high cost and dependence on cold-chain storage posed logistical challenges, particularly in resource-limited settings [4]. In contrast, the ChAdOx1 nCoV-19 vaccine (AZD1222 or Vaxzevria), an affordable viral vector-based platform, is stable at standard refrigeration temperatures (2–8 °C) for at least six months [5], greatly enhancing its feasibility for vaccination scale-up in regions with inadequate healthcare infrastructure [4].
Randomized controlled trials (RCTs) have demonstrated considerable protection for the ChAdOx1 nCoV-19 primary series against SARS-CoV-2 infection [6–8]. Efficacy against symptomatic infection with the Wuhan virus, more than 14 days after the second dose, was 62.1% in an RCT conducted in the United Kingdom (UK) and Brazil [6], and 74% in a separate RCT conducted across the United States, Chile, and Peru [7]. Further analysis from the UK trial found an efficacy of 66.7% against symptomatic infection with the Alpha variant [8].
However, an RCT in South Africa suggested no efficacy against infection with the Beta variant, raising concerns over the vaccine’s utility, though the results carried substantial statistical uncertainty [9]. Subsequent final analysis of this trial estimated the vaccine’s efficacy at 90.6% against infection with the Wuhan virus, 77.1% against infection with the Delta variant, and only 6.7% against infection with the Beta variant but also with considerable statistical uncertainty [10].
Qatar launched its COVID-19 immunization program in late December 2020 using mRNA vaccines [11]. The ChAdOx1 nCoV-19 vaccine was subsequently introduced for a brief period to accelerate vaccination efforts and was administered through a few mass public vaccination campaigns. However, its use in these campaigns was rapidly discontinued following the negative findings of the South African trial against the Beta variant [9], which was also circulating in Qatar at the time [12], along with reports of rare blood clotting events in other countries [13, 14].
Although the ChAdOx1 nCoV-19 vaccine is no longer in use worldwide, particularly following the emergence of the Omicron variant and the availability of updated vaccines better matched to circulating strains, this study was conducted to complete the evidence base on the real-world effectiveness of first-generation vaccines. It offers insights from one of the most comprehensively studied national populations for COVID-19 vaccine effectiveness [15–22] and may help guide the development of future viral vector vaccines.
This study investigates the effectiveness of the two-dose primary series of the ChAdOx1 nCoV-19 vaccine against SARS-CoV-2 infection, symptomatic infection, and severe (acute-care hospitalization) [23], critical (intensive-care-unit hospitalization) [23], and fatal [24] coronavirus disease 2019 (COVID-19) during periods dominated by the Beta and Delta variants. Vaccine effectiveness against infection was assessed overall and stratified by variant type, prior infection status, clinical vulnerability status, and time since the second dose. In addition, the study includes an analysis of the effectiveness of a single vaccine dose against any infection—both overall and stratified by variant—as well as against symptomatic infection and severe, critical, or fatal COVID-19.
Methods
This study builds on previous research assessing COVID-19 vaccine effectiveness in Qatar using a test-negative, case-control design [15–17, 25, 26]. Comprehensive descriptions of this methodological approach have been published elsewhere [15–17, 25, 26]. Key methods are briefly summarized below.
Study population and data sources
This nationwide study was conducted in Qatar from January 1, 2021 to December 18, 2021, covering the period between the launch of the COVID-19 primary-series vaccination campaign [15, 16] and the introduction of the Omicron variant on December 19, 2021 [27]. Early in the year, infection incidence was driven by the Alpha [28] and subsequently the Beta [12] variants, before transitioning into an extended phase dominated by the Delta variant [25] (Supplementary Fig. 1).
Data were sourced from the integrated national digital-health platform (Supplementary Sect. 1), which includes comprehensive information on COVID-19 testing, vaccination, hospitalizations, and deaths. Since the pandemic onset, all SARS-CoV-2 polymerase chain reaction (PCR) tests, regardless of facility or location, have been captured with no missing data (Supplementary Sect. 2). Approximately 5% of Qatar’s population underwent weekly testing during the study period, primarily for routine screening, leading to most infections being identified preemptively rather than through symptomatic testing [17, 18].
Demographic details (sex, age, nationality) were obtained from the national health registry; notably, around 89% of Qatar’s diverse population are expatriates from over 150 countries [29]. COVID-19 vaccines were administered free of charge to all residents and were closely tracked nationwide [11, 17]. More extensive descriptions of the population and data sources have been documented elsewhere [17–20, 29–32].
The ChAdOx1 nCoV-19 vaccine allows flexibility in the interval between the first and second doses, typically ranging from 4 to 12 weeks [6, 33, 34]. Although initial trials used a 4-week interval, subsequent analyses explored extended dosing schedules [6, 33]. Based on these findings, the World Health Organization (WHO) recommended an interval of 8–12 weeks [34, 35]. Many countries adopted this recommendation—or even longer intervals—driven by logistical considerations and emerging immunological evidence [34, 36, 37]. In Qatar, an 8-week interval was adopted as the target schedule for the primary series, reflecting both the logistical demands of mass, field-based vaccination campaigns and the evolving evidence on the vaccine’s immunogenicity at the time.
Study design
The ChAdOx1 nCoV-19 primary-series vaccine effectiveness against SARS-CoV-2 infection was estimated using a test-negative, case-control design [16, 17, 25, 38–40]. Cases were defined as PCR-positive tests and controls as PCR-negative tests, both conducted during the study period. Effectiveness was determined by comparing the odds of having received the two-dose primary series between cases and controls.
Cases or controls with a PCR-positive result in the preceding 90 days were excluded to avoid misclassification of prolonged positivity as a prior infection [41–43], while those with earlier infections (≥ 90 days) were classified as having a prior infection. Cases or controls who had received any mRNA vaccine dose, or a single dose or more than two doses of the ChAdOx1 nCoV-19 vaccine, were also excluded. Tests conducted within 14 days of the second vaccine dose were additionally excluded.
Cases and controls were matched exactly one-to-five by sex, 10-year age group, nationality, number of coexisting conditions (0 to ≥ 6; Supplementary Sect. 3), prior infection status, PCR test calendar week, and reason for testing, with matching ratio chosen to enhance statistical precision. This matching approach minimized confounding based on known risk factors for infection risk [29, 44–47], as informed by findings of earlier studies on Qatar’s population [11, 16, 17, 48–50].
Effectiveness was estimated both against any SARS-CoV-2 infection, as well as against symptomatic infection by restricting the analysis to tests conducted for clinical suspicion of respiratory symptoms. Variant-specific effectiveness was further assessed by restricting the analysis to periods dominated by each variant: March 8–May 31, 2021, for Beta [51, 52], and June 1–December 18, 2021, for Delta [25, 51, 52]. This time-based classification of circulating variants was informed by viral genome sequencing and variant genotyping conducted throughout the pandemic, as detailed in previous publications [16, 17, 19, 25, 53–55] and Supplementary Sect. 2.
To assess protection against severe outcomes, cases that progressed to severe [23], critical [23], or fatal [24] COVID-19 were matched exactly one-to-five to controls. Severity was determined by trained medical personnel based on independent chart reviews, following the WHO guidelines (Supplementary Sect. 4). All hospitalized patients with PCR-confirmed infections were assessed for disease severity every three days until discharge or death. In this study, individuals were classified based on their worst outcome starting with death, followed by critical, then severe illness.
One-dose vaccine effectiveness against infection and severe COVID-19
An additional analysis evaluated the effectiveness of a single dose of the ChAdOx1 nCoV-19 vaccine, starting 14 days after administration, against any SARS-CoV-2 infection—both overall and stratified by variant—as well as against symptomatic infection and severe, critical, or fatal COVID-19, using the same methodological approach as for the two-dose primary series.
Statistical analysis
All PCR test records were reviewed for case and control selection, but only matched samples were included in the analysis. Cases and controls were described using frequency distributions and measures of central tendency, with standardized mean differences (SMDs) ≤ 0.1 indicating adequate balance [56].
Odds ratios (ORs), comparing the odds of primary series vaccination between cases and controls, and associated 95% confidence intervals (CIs), were estimated using conditional logistic regression. CIs were not adjusted for multiple comparisons. Interactions were not examined. Unvaccinated individuals served as the reference group in all estimations.
Vaccine effectiveness and corresponding 95% CI were calculated as 1-OR if the OR was < 1, and as 1/OR-1 if the OR was ≥ 1 [20, 57]. This approach yields a symmetric scale from − 100 to 100% for intuitive interpretation of both positive and negative effectiveness [20, 57]. When the conditional logistic regression failed to converge because of zero vaccinated cases, the 95% CI was calculated using McNemar’s test, using the total number of matched pairs in the 1:n design, as done in earlier studies [26, 51].
Additional analyses were conducted to estimate vaccine effectiveness by time since the second dose (first month and subsequently by 2-month intervals), prior infection status, age (< 50 years; ≥50 years), and clinical vulnerability status. Individuals < 50 years with ≤ 1 comorbidity were considered less clinically vulnerable to severe COVID-19, while those ≥ 50 years or < 50 years but with ≥ 2 comorbidities were classified as more vulnerable to severe COVID-19 [20, 30].
Statistical analyses were conducted in STATA/SE version 18.0 (Stata Corporation, College Station, TX, USA).
Ethics approval, patient consent, and oversight
The study was approved by the institutional review boards at Hamad Medical Corporation (reference number: MRC–01–20–1078) and Weill Cornell Medicine–Qatar (reference number: 20–00017) and a waiver of informed consent was also approved by the institutional review boards at Hamad Medical Corporation (reference number: MRC–01–20–1078) and Weill Cornell Medicine–Qatar. This study was conducted in accordance with the ethical principles outlined in the Declaration of Helsinki. The study was reported following the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines (Supplementary Table 1).
Results
Study population
Between January 1, 2021 and December 18, 2021, the study’s end date, 33,457 individuals received two or more doses of the ChAdOx1 nCoV-19 vaccine. For comparison, during the same period, 2,175,216 individuals received two or more doses of an mRNA COVID-19 vaccine.
The median date for the first ChAdOx1 nCoV-19 dose was April 28, 2021 (interquartile range (IQR), April 26, 2021–May 20, 2021). The median date for the second dose was June 29, 2021 (IQR, June 28, 2021–July 18, 2021). The median time between the first and second vaccine doses was 61 days (IQR, 56–64 days). Figure 1 presents the distribution of first and second doses of the ChAdOx1 nCoV-19 vaccine during the study period.
Fig. 1. Distribution of A first and B second doses of the ChAdOx1 nCoV-19 (Vaxzevria) vaccine during the study period
Fig. 2. Flowchart describing the study population selection process for investigating ChAdOx1 nCoV-19 (Vaxzevria) vaccine effectiveness
Fig. 3. Effectiveness of the ChAdOx1 nCoV-19 (Vaxzevria) vaccine against infection by time since the second vaccine dose. Error bars indicate the 95% confidence intervals for the estimated vaccine effectiveness (blue markers)
Figure 2 outlines the selection process for the study population. Of 287,558 PCR-positive tests from 241,673 individuals, 82,818 were excluded due to recent prior infection, receipt of mRNA vaccines, having only one ChAdOx1 nCoV-19 dose, or insufficient time since the second dose, leaving 204,740 eligible tests. Of these, 186,130 were successfully matched to controls. Among 6,541,189 PCR-negative tests from 2,678,173 individuals, 2,843,550 were excluded for similar reasons, resulting in 3,697,639 eligible tests, of which 667,289 were matched to cases. The final matched dataset included 186,130 PCR-positive tests from 185,877 individuals and 667,289 PCR-negative tests from 544,720 individuals.
Table 1 presents the characteristics of cases and controls in both unmatched and matched samples. As the study was conducted on Qatar’s population, the study population reflects the country’s internationally diverse, yet predominantly young and male demographic profile.
Table 1. Characteristics of cases and controls in samples used to estimate the effectiveness of the ChAdOx1 nCoV-19 (Vaxzevria) vaccine against SARS-CoV-2 infection and against severe COVID-19CharacteristicsUnmatched analysisMatched analysisCasesControlsSMD^†^CasesControlsSMD^†^N = 204,740N = 3,697,639N = 186,130N = 667,289Median age (IQR)—years32 (24–39)30 (21–38)0.10^‡^31 (23–38)31 (23–37)0.06^‡^Age group—no. (%) < 10 years21,312 (10.4)526,774 (14.2)0.1519,566 (10.5)73,488 (11.0)0.08 10–19 years18,685 (9.1)324,387 (8.8)16,826 (9.0)59,861 (9.0) 20–29 years45,903 (22.4)900,034 (24.3)44,107 (23.7)171,397 (25.7) 30–39 years69,549 (34.0)1,133,095 (30.6)65,715 (35.3)236,580 (35.5) 40–49 years34,884 (17.0)537,270 (14.5)30,208 (16.2)98,418 (14.7) 50–59 years11,129 (5.4)202,720 (5.5)8,175 (4.4)23,849 (3.6) 60–69 years2,499 (1.2)57,710 (1.6)1,273 (0.7)3,153 (0.5) 70 + years779 (0.4)15,649 (0.4)260 (0.1)543 (0.1)Sex Male140,390 (68.6)2,655,156 (71.8)0.07129,004 (69.3)468,425 (70.2)0.02 Female64,350 (31.4)1,042,483 (28.2)57,126 (30.7)198,864 (29.8)Nationality^§^ Bangladeshi14,967 (7.3)188,752 (5.1)0.2713,820 (7.4)45,961 (6.9)0.09 Egyptian11,084 (5.4)182,410 (4.9)10,019 (5.4)32,516 (4.9) Filipino22,658 (11.1)215,701 (5.8)21,234 (11.4)73,160 (11.0) Indian57,089 (27.9)1,192,425 (32.2)54,807 (29.4)208,913 (31.3) Nepalese18,169 (8.9)296,022 (8.0)16,746 (9.0)60,174 (9.0) Pakistani10,242 (5.0)208,323 (5.6)9,269 (5.0)34,947 (5.2) Qatari21,653 (10.6)401,165 (10.8)21,035 (11.3)86,787 (13.0) Sri Lankan6,726 (3.3)75,055 (2.0)5,922 (3.2)18,452 (2.8) Sudanese5,235 (2.6)73,557 (2.0)4,534 (2.4)14,924 (2.2) Other nationalities^¶^36,917 (18.0)864,229 (23.4)28,744 (15.4)91,455 (13.7)Coexisting conditions** 0168,285 (82.2)3,239,872 (87.6)0.16159,146 (85.5)587,477 (88.0)0.08 122,250 (10.9)298,426 (8.1)18,250 (9.8)57,392 (8.6) 28,465 (4.1)94,203 (2.5)5,854 (3.1)15,987 (2.4) 32,929 (1.4)32,160 (0.9)1,591 (0.9)3,814 (0.6) 41,394 (0.7)15,626 (0.4)651 (0.3)1,322 (0.2) 5769 (0.4)8,458 (0.2)307 (0.2)591 (0.1) 6+648 (0.3)8,894 (0.2)331 (0.2)706 (0.1)Prior infection status No prior infection202,636 (99.0)3,512,961 (95.0)0.23184,406 (99.1)660,421 (99.0)0.01 Prior infection2,104 (1.0)184,678 (5.0)1,724 (0.9)6,868 (1.0)Reason for testing Clinical suspicion60,732 (29.7)209,840 (5.7)1.0650,286 (27.0)107,634 (16.1)0.32 Contact tracing25,067 (12.2)147,249 (4.0)22,251 (12.0)74,766 (11.2) Survey34,071 (16.6)555,883 (15.0)32,131 (17.3)134,905 (20.2) Port of entry44,159 (21.6)1,833,716 (49.6)43,596 (23.4)213,969 (32.1) Individual request14,875 (7.3)182,759 (4.9)13,989 (7.5)59,733 (9.0) Healthcare routine testing18,627 (9.1)129,120 (3.5)17,493 (9.4)47,823 (7.2) Pre-travel6,552 (3.2)629,773 (17.0)6,150 (3.3)28,005 (4.2) Other657 (0.3)9,299 (0.3)234 (0.1)454 (0.1)IQR denotes interquartile range, COVID-19 coronavirus disease 2019, PCR polymerase chain reaction, SARS-CoV-2 severe acute respiratory syndrome coronavirus 2, and SMD standardized mean difference*Cases (PCR-positive tests) and controls (PCR-negative tests) were matched exactly one-to-five by sex, 10-year age group, nationality, number of coexisting conditions, prior infection status, calendar week of PCR test, and reason for testing^†^SMD quantifies covariate balance between groups and is calculated as the difference in the covariate means divided by the pooled standard deviation. An SMD ≤ 0.1 is typically interpreted as indicating adequate balance. However, in matched samples with variable matching ratios (e.g., one to five controls per case), SMD values may exceed 0.1 even when exact matching on covariate values is applied and cases and controls are fully balanced by design. This apparent imbalance reflects the sensitivity of SMD to differences in within-group variance introduced by variable matching ratios, rather than true imbalance in covariate distributions^‡^SMD is for the mean difference between groups divided by the pooled standard deviation^§^Nationalities were chosen to represent the most populous groups in Qatar^¶^These comprise up to 183 other nationalities in Qatar in the unmatched and 123 nationalities in the matched analysis
Table 2. Effectiveness of the ChAdOx1 nCoV-19 (Vaxzevria) vaccine against (A) any infection, (B) symptomatic infection, and (C) severe, critical or fatal COVID-19EffectivenessCasesControlsEffectiveness^†^ in %(95% CI)^‡^Vaccinated (n)Unvaccinated (n)Vaccinated (n)Unvaccinated (n)(A) Any infection56186,074718666,57166.0 (55.1 to 74.3) Variant Beta0105,94112321,306100 (64.0 to 100)^¶^ Delta5635,497704161,67565.3 (54.2 to 73.8) Time after second dose 14–30 days6186,063125666,34978.4 (50.7 to 90.5) 31–90 days16186,066275666,38775.2 (58.6 to 85.2) 91–150 days19186,068192666,41257.7 (31.4 to 73.9) 151–200 days15186,074122666,57145.6 (5.5 to 68.7) Prior infection status No prior infection54184,352696659,72566.0 (54.8 to 74.4) Prior infection21,722226,84666.5 (-33.7 to 92.6) Age < 50 years54176,368691639,05365.5 (54.2 to 74.0) ≥ 50 years29,7062727,51875.6 (-5.0 to 94.3) Clinical vulnerability to severe COVID-19 Less clinically vulnerable54170,043683621,99464.6 (53.0 to 73.4) More clinically vulnerable216,0313544,57784.0 (32.0 to 96.2)(B) Symptomatic infection^II^850,278121107,51373.0 (44.1 to 87.0)(C) Severe, critical, or fatal COVID-19^§^04,785918,305100 (49.3 to 100)^¶^CI denotes confidence interval, COVID-19 coronavirus disease 2019, and SARS-CoV-2 severe acute respiratory syndrome coronavirus 2*Cases (PCR-positive tests) and controls (PCR-negative tests) were matched exactly one-to-five by sex, 10-year age group, nationality, number of coexisting conditions, prior infection status, calendar week of PCR test, and reason for testing^†^Vaccine effectiveness was estimated using the test-negative, case–control study design^‡^CIs were not adjusted for multiplicity and thus should not be used to infer definitive differences between different groups^§^Severity, criticality, and fatality were defined according to the World Health Organization guidelines^II^A symptomatic infection was defined as a SARS-CoV-2 PCR-positive test conducted because of clinical suspicion due to presence of symptoms compatible with a respiratory tract infection^¶^The 95% CI was estimated using McNemar’s test because of zero vaccinations among cases
Two-dose primary series vaccine effectiveness against infection and severe COVID-19
The overall effectiveness of the ChAdOx1 nCoV-19 primary series in preventing SARS-CoV-2 infection, irrespective of symptoms, was estimated at 66.0% (95% CI, 55.1–74.3%) (Table 2). Effectiveness against symptomatic infection was higher, estimated at 73.0% (95% CI, 44.1–87.0%). Effectiveness against severe, critical, or fatal COVID-19 was estimated at 100% (95% CI, 49.3–100%), with no vaccinated individuals progressing to severe, critical, or fatal disease following infection.
Effectiveness against Beta variant infection, irrespective of symptoms, was estimated at 100% (95% CI, 64.0–100%), while effectiveness against Delta variant infection was 65.3% (95% CI, 54.2–73.8%). In the Beta variant analysis, the median date of the second dose was March 13, 2021 (IQR, February 24–April 9, 2021), whereas in the Delta variant analysis, it was June 28, 2021 (IQR, June 17–June 29, 2021). The median interval between the second dose and the PCR test was 53 days (IQR, 21–62.5 days) in the Beta variant analysis and 81 days (IQR, 39–130.5 days) in the Delta variant analysis.
Effectiveness against any infection, regardless of variant, peaked at 78.4% (95% CI, 50.7–90.5%) during the 14–30 days following the second dose (Fig. 3). It remained relatively high at 75.2% (95% CI, 58.6–85.2%) between 31 and 90 days post-vaccination but declined to 57.7% (95% CI, 31.4–73.9%) during days 91–150. Thereafter, effectiveness further waned to 45.6% (95% CI, 5.5–68.7%) between days 151 and 200 following the second dose.
There was no evidence that vaccine effectiveness differed by prior infection status, age group, or clinical vulnerability status (Table 2). However, the estimated effectiveness in several of these subgroups was associated with wide 95% CIs, limiting the ability to make statistically precise comparisons.
Additional analysis: one-dose vaccine effectiveness against infection and severe COVID-19
The overall effectiveness of a single dose of the ChAdOx1 nCoV-19 vaccine was estimated at 59.9% (95% CI, 51.0–67.3%) against any SARS-CoV-2 infection, 78.4% (95% CI, 60.9–88.0%) against symptomatic infection, and 100% (95% CI, 88.9–100%) against severe, critical, or fatal COVID-19, with no severe cases reported among vaccinated individuals. Variant-specific effectiveness was estimated at 65.0% (95% CI, 49.7–75.6%) against Beta variant infection and 55.9% (95% CI, 43.8–65.5%) against Delta variant infection, irrespective of symptoms.
Discussion
The findings demonstrate substantial protection conferred by the ChAdOx1 nCoV-19 primary series, with overall effectiveness of 66.0% against infection during periods dominated by the Beta and Delta variants. Notably, a single dose also provided considerable protection, with effectiveness estimated at 59.9%. Protection peaked within the first three months following the second dose but declined to below 50% after 150 days.
This waning of effectiveness aligns with evidence of declining protection over time for both ChAdOx1 nCoV-19 [58–61] and mRNA vaccines [17, 48], underscoring the need for booster doses to sustain protection. The vaccine also provided strong protection against severe, critical, or fatal COVID-19, with no severe cases reported among vaccinated individuals during the study period. This reinforces the vaccine’s role in reducing hospitalizations and deaths, consistent with findings from other studies [59, 62–67], and supports its broad protective benefits across population groups and clinical presentations.
Vaccine effectiveness against the Delta variant was estimated at 65%, consistent with vaccine efficacy reported against this variant in an RCT [10] and with findings from real-world effectiveness studies conducted in Canada [63], the Czech Republic [59], Finland [58], India [68], the Netherlands [69, 70], Scotland [64], Spain [71], Thailand [60], and the UK [72, 73].
Importantly, this study, to our knowledge, provided the first statistically meaningful estimate of the effectiveness of the ChAdOx1 nCoV-19 vaccine against the Beta variant [1], demonstrating strong protection. No infection cases were identified among vaccinated individuals, and the estimated minimum effectiveness was 64%. Another estimate from Canada also indicated strong protection against Beta, although the 95% CI was very wide [62].
This finding contrasts with results from the RCT conducted in South Africa, which reported negligible efficacy against the Beta variant, accompanied by a fairly wide 95% CI [9, 10]. In response to that trial, several countries where Beta was circulating discontinued use of this vaccine, despite global vaccine shortages at the time [74]. Reports of rare blood clotting events associated with thromboembolic and thrombocytopenic complications also contributed to the decision [13, 14]. The present findings suggest that this decision may have been suboptimal and potentially premature, limiting access to an affordable vaccine that could have provided protection against infection, reduced severe disease outcomes, and averted deaths during a period of high transmission and unmet vaccination need [14].
Notably, a similar discrepancy was observed for mRNA vaccines and natural infection in relation to protection against infection with the Beta variant. Molecular-level evidence initially suggested that Beta might evade both vaccine-induced and naturally acquired immunity [75, 76], but population-level data later demonstrated that the impact of Beta mutations on protection conferred by mRNA vaccination and prior infection was modest [12, 15, 16].
This study has limitations. Although it included a large number of PCR tests, the number of individuals vaccinated with ChAdOx1 nCoV-19 in Qatar was relatively small due to the vaccine’s early discontinuation. This limited the feasibility and statistical power for some subgroup analyses, particularly for assessing effectiveness over time and against symptomatic infection and severe COVID-19 by variant type. It also constrained the feasibility of relevant analyses, such as evaluating the impact of dosing intervals on vaccine effectiveness. Furthermore, the findings may have reduced generalizability to settings where this vaccine was more widely used.
Variant classification was based on periods of variant dominance rather than genomic sequencing or genotyping of all infections. There also was a difference of nearly one month in the median interval between the second dose and the PCR test in the Beta versus Delta analyses, which may have contributed—albeit modestly—to the observed differences in effectiveness between the two variants. A meaningful analysis of post-vaccination clotting events was not feasible due to the limited number of cases. Only sixteen stroke-related events of any type were reported among individuals who had ever received a dose of ChAdOx1 nCoV-19 [77], a number far too small to allow for a reliable assessment of any potential causal relationship.
COVID-19 vaccination in Qatar was offered free of charge to all citizens and residents through the public healthcare system [11], with prioritization based on factors such as age, chronic conditions, and occupation [17]. The ChAdOx1 nCoV-19 vaccine was available for only a short, specific period before being discontinued and was primarily administered through field-based mass campaigns. As a result, recipients of the ChAdOx1 nCoV-19 vaccine and those who received mRNA vaccines may differ. However, rigorous matching was applied in this study to adjust for potential confounding factors. Moreover, since the analysis estimates the biological effect of vaccination, which is not expected to vary by socioeconomic factors, differences between recipients of different vaccines should not meaningfully impact the estimated outcomes.
This study was conducted in a unique national population that differs substantially from those of most other countries. Qatar has a distinctly young and diverse demographic profile, with only 9% of residents aged ≥ 50 years and 89% comprising expatriates from over 150 countries [29, 78]. Additionally, more than two-thirds of the population are male, primarily migrant workers typically employed in large infrastructure projects [29, 31, 44–47]. As such, the extent to which the study findings can be generalized to other populations remains uncertain.
The observational test-negative design can be subject to potential bias, including from unmeasured differences in test-seeking behavior or changes in testing patterns. Most healthcare data were captured electronically, but misclassification bias remains a concern in real-world data. Such bias may arise from inaccuracies in exposure (e.g., missing vaccination records), covariates (e.g., comorbidities), or outcomes (e.g., hospitalizations outside Qatar), and may be non-differential across study groups.
Matching in case-control studies helps reduce confounding but may not eliminate bias and may introduce selection bias [79]. Although matching included key variables such as age, sex, and nationality, other factors like geographic location or occupation could not be accounted for due to data limitations. However, Qatar’s city-state structure supports relatively uniform infection risk across neighborhoods, and age, sex, and nationality serve as reliable proxies for socio-economic status in this population [29, 44–47]. Matching on these variables may have partially controlled for unmeasured differences in exposure risk, including occupation. This approach has been validated in prior studies using various designs and control groups to test for null effects, with findings supporting its robustness [11, 16, 17, 48, 80].
This study has strengths. It is the first to provide an estimate of the real-world effectiveness of the ChAdOx1 nCoV-19 vaccine against the Beta variant. The analysis was conducted at the national level, encompassing a diverse population with a wide range of national backgrounds. Findings were based on comprehensive, validated national databases established through prior vaccine effectiveness studies, with infections confirmed by PCR testing. The use of an integrated digital health information platform enabled robust data capture on potential confounders and facilitated rigorous matching based on socio-demographic characteristics and a set of health indicators. Controls were drawn from the national population using exact matching, ensuring precise pairing with cases.
In conclusion, this study provides real-world evidence of the effectiveness of the ChAdOx1 nCoV-19 vaccine, including against the Beta variant, for which prior data were limited and inconclusive. The findings affirm the vaccine’s substantial protection against SARS-CoV-2 infection and its strong protection against severe COVID-19 outcomes, including during periods dominated by the Beta and Delta variants. These results contribute to a more complete understanding of the vaccine’s performance across diverse settings and variants, challenge early assumptions, and underscore the value of leveraging national data systems to inform policy decisions.
Supplementary Information
Below is the link to the electronic supplementary material.
Supplementary Material 1
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1International Vaccine Access Center, Johns Hopkins Bloomberg School of Public Health. VIEW-hub: COVID-19 vaccines. Available from: https://view-hub.org/vaccine/covid/. Accessed 9 Mar 2025.
- 2European Medicines Agency. COVID-19 Vaccine Astra Zeneca: benefits still outweigh the risks despite possible link to rare blood clots with low blood platelets. 2021. Available from: https://www.ema.europa.eu/en/news/covid-19-vaccine-astrazeneca-benefits-still-outweigh-risks-despite-possible-link-rare-blood-clots-low-blood-platelets. Accessed 39 March 2025.
- 3World Health Organization (WHO). Living guidance for clinical management of COVID-19. 2023. Available from: https://www.who.int/publications/i/item/WHO-2019-n Co V-clinical-2021-2. Accessed 27 Feb 2023.
- 4World Health Organization (WHO). International Guidelines for Certification and Classification (Coding) of COVID-19 as Cause of Death. 2023. Available from: https://www.who.int/publications/m/item/international-guidelines-for-certification-and-classification-(coding)-of-covid-19-as-cause-of-death. Accessed 27 Feb 2023.
- 5Al Nuaimi AA, Chemaitelly H, Semaan S, Al Mukdad S, Al-Kanaani Z, Kaleeckal AH, Latif AN, Al-Romaihi HE, Butt AA, Al-Thani MH et al. All-cause and COVID-19 mortality in Qatar during the COVID-19 pandemic. BMJ Glob Health. 2023;8(5).10.1136/bmjgh-2023-012291 PMC 1016333437142299 · doi ↗ · pubmed ↗
- 6Chemaitelly H, Ayoub HH, Coyle P, Tang P, Hasan MR, Yassine HM, Al Thani AA, Al-Kanaani Z, Al-Kuwari E, Jeremijenko A et al. Differential protection against SARS-Co V-2 reinfection pre- and post-Omicron. Nature; 2025;639: 1024–1031. 10.1038/s 41586-024-08511-9PMC 1194689739910292 · doi ↗ · pubmed ↗
- 7World Health Organization. Interim recommendations for use of the Ch Ad Ox 1-S [recombinant] vaccine against COVID-19 (Astra Zeneca COVID-19 vaccine AZD 1222 Vaxzevria, SII COVISHIELD™). 2021. Available from: https://iris.who.int/bitstream/handle/10665/343388/WHO-2019-n Co V-vaccines-SAGE-recommendation-AZD 1222-2021.3-eng.pdf?sequence=1&is Allowed=y. Accessed 14 July 2025.
- 8Pilz S, Theiler-Schwetz V, Trummer C, Krause R, Ioannidis JPA. SARS-Co V-2 reinfections: overview of efficacy and duration of natural and hybrid immunity. Environ Res 2022:112911.10.1016/j.envres.2022.112911 PMC 882430135149106 · doi ↗ · pubmed ↗