Optimizing a community-based intervention to improve help-seeking for depression care: study protocol for a randomized factorial trial
Nagendra P. Luitel, Brandon A. Kohrt, Bishnu Lamichhane, Anvita Bhardwaj, Kamal Gautam, Mark JD Jordans

TL;DR
This study aims to improve help-seeking behavior for depression care in Nepal by testing a community-based intervention using a randomized trial.
Contribution
The study introduces a factorial trial design to optimize a community-based depression intervention in a low-income country.
Findings
The study will evaluate the effectiveness of four components of a community-based intervention on promoting help-seeking behavior.
The Multiphase Optimization Strategy (MOST) framework will be used to determine optimal intervention components for a future full trial.
Abstract
Depression is a common mental health issue that can be effectively managed in primary and community health care settings. However, there is a significant gap between the number of individuals in need of care and those who actually receive treatment, with the greatest gap in low- and middle-income countries (LMICs). Although efforts have been made in LMICs to improve access to mental health services by addressing supply-side barriers, there has been less attention to demand-side obstacles. On the demand side, factors such as stigma, negative attitudes, and limited awareness of available services lead to underutilization of mental health services. This protocol describes a study of active ingredients of a community-based intervention aimed at enhancing help-seeking for depression care in Nepal, a LMIC with low rates of mental health treatment seeking. The study will take place in two…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
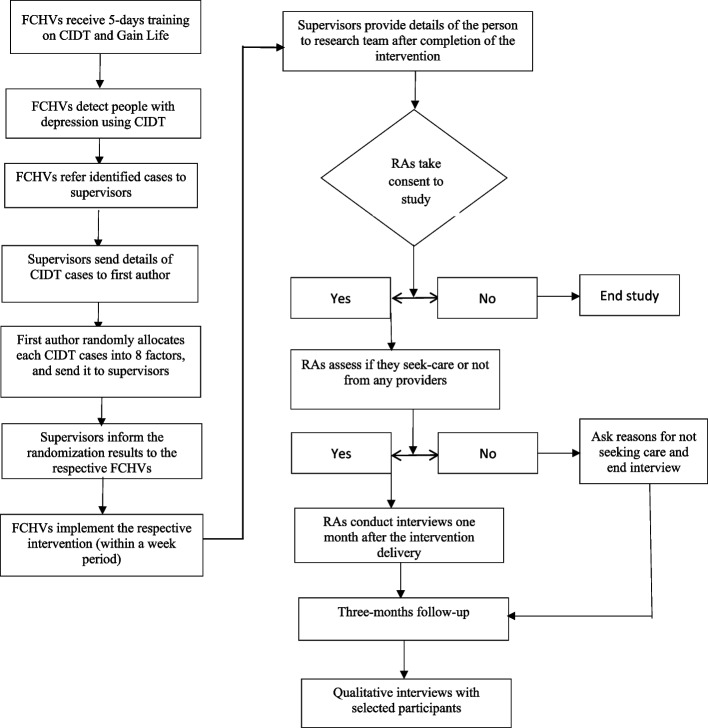 Figure 1
Figure 1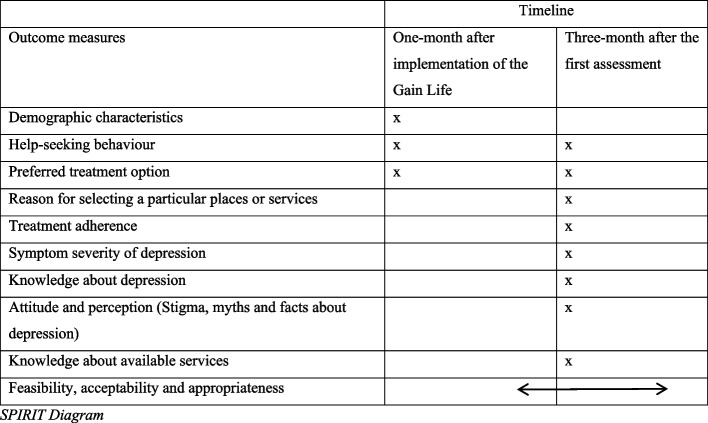 Figure 2
Figure 2- —http://dx.doi.org/10.13039/100010269Wellcome Trust
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMental Health Treatment and Access · Child and Adolescent Psychosocial and Emotional Development · Family Caregiving in Mental Illness
Introduction
Depression is a prevalent mental health condition that imposes significant emotional and financial burden on individuals, families, and communities [22, 25, 35, 56]. It is estimated that over 322 million people globally are affected by depression [76], accounting for 40.5% of disability-adjusted life years (DALYs) caused by mental illness [74]. It is associated with increased risk of suicide, type-2 diabetes, and heart disease [4, 38, 64] with over 50% of suicide victims having depression [64]. Women are reported to be 2 to 3 times more likely to experience depression than men [51, 73], with a higher risk during the perinatal period, from pregnancy to one year post-delivery [2, 23, 58, 73].
Depression is a treatable and potentially preventable condition [3]. Timely and appropriate help-seeking is crucial for early detection, treatment, and recovery [16]. Research has shown that depression and other mental health conditions can be effectively treated in primary and community health care systems through a task-sharing approach [7, 34, 37]. Despite the availability of evidence-based cost-effective interventions for depression, there is a significant gap between the number of individuals in need of care and those who receive treatment [8, 9, 28, 34, 63, 70, 75]. Studies have reported that 86.3% of people with anxiety, mood, or substance disorders in lower-middle-income countries received no treatment [20]. Additionally, individuals with depression often prefer seeking help from informal sources such as traditional healers, friends, or family members rather than professionals like doctors, psychiatrists, or psychologists [65, 66].
Nepal has made significant strides in improving access to mental health care. Initiatives include translating and adapting the WHO mental health gap action programme intervention guide (mhGAP-IG) for use in Nepal [46], developing a national mental health strategy and action plan [57], creating mental health training manuals for health care providers [41, 44], providing free psychotropic medicines at the lowest level of health care facilities [71], and establishing a standard treatment protocol [43]. The World Health Organization (WHO) has been supporting the government in implementing and scaling up mental health services throughout the country through its special initiatives [55]. Despite these efforts, a large proportion of people (77%) with mental health conditions in Nepal do not receive any treatment [62]. The main reasons for not seeking mental health services are related to individuals’ attitudes and intentions towards mental health problems. For example, the national mental health survey revealed that approximately half of the participants who did not seek care believed that the problem would resolve on its own (48%), followed by a willingness to solve the problem independently (47%), and the perception that they did not have mental health issues (46%) [62].
The underutilization of mental health services in many low- and middle-income countries (LMICs) can be influenced by various factors, including structural and attitudinal barriers. Efforts have been made to improve the availability of mental health services by addressing supply-side barriers through a task-sharing approach and reducing structural barriers. However, demand-side barriers, such as low perceived needs, stigma, and negative attitudes towards mental health treatment, are often overlooked [1]. Stigma and negative attitudes towards mental health care significantly contribute to the underutilization of services and are crucial barriers to seeking help [12, 30, 59, 68]. Internalized stigma is linked to reduced help-seeking behaviour or negatively affects help-seeking [10, 11]. Poor mental health literacy, lack of knowledge about available services, lack of trust in services, cultural practices and beliefs, and low detection within the family are other significant barriers to accessing mental health services [1, 5, 18, 26, 30, 45, 47, 67].
Research has shown a positive relationship between mental health literacy and help-seeking behaviour, indicating that improved mental health literacy can increase the likelihood of seeking help [29, 72]. Similarly, individuals’ attitudes and intentions toward seeking help can predict future behaviour [69], emphasing the importance of interventions that promote positive attitudes toward mental health care to encourage actual help-seeking behaviour [27]. Social-contact-based interventions involving education and personal recovery stories have been used to reduce mental health stigma [50] including in Nepal [40], but they often yield only short-term results [54]. These findings suggest a need for evidence-based interventions to improve help-seeking behaviour for mental health care.
This study aims to develop a community-based intervention to address barriers to seeking help for depression by focusing on improving mental health literacy, increasing awareness of available mental health services, dispelling myths and misconceptions about depression, and changing negative attitudes towards depression care through a recovery story from someone who has experienced depression. The intervention was developed through a systematic review, qualitative study, and input from various stakeholders, including individuals with lived experience and mental health experts. This paper outlines the intervention, the evaluation methods used to assess its delivery strategies, and the testing of its feasibility, acceptability, and appropriateness.
Methods
Objective
The aim of this study is to analyze the active components of Gain-Life (Give informAtIoN to transform Life), a community-based intervention designed to promote help-seeking for depression care. The study will examine the effects of intervention components including information on depression, awareness of treatment options, stigma reduction, dispelling myths about depression, and sharing personal transformation experiences, on help-seeking behaviour as the primary outcome and treatment adherence as secondary outcomes. Furthermore, the study will evaluate the delivery methods and assess the feasibility, acceptability, and appropriateness of Gain-Life intervention in encouraging help-seeking for depression care.
- The primary research question of this study is to determine which component of the Gain-Life intervention has a positive impact on the primary outcome of help-seeking behaviour among individuals with depression. This outcome is measured as the percentage of people seeking care from a health care provider within one month of receiving the intervention.
- The secondary research question aims to evaluate the intervention’s effects on different outcomes, such as treatment adherence, reduction in depression symptom severity, and the feasibility, acceptability, and appropriateness of Gain-Life in promoting help-seeking for depression treatment.
Setting
The study will be conducted in two municipalities in the Morang district of eastern Nepal. Morang is one of the most populous districts in the country and also diverse in caste/ethnicity, language, and geography. The total population of Morang district is 1,148,156 according to the 2021 census [61]. The selection of Patharisanischare municipality and Kanepokhari rural municipality for this study was purposeful taking into account factors such as diversity in caste/ethnicity and language, absence of mental health services, lack of FCHVs trained in the community informant detection strategy, and the willingness of local government to provide support. The combined population of Kanepokhari (43,193) and Patharisanischare (72,451) is 115,544 with 54,389 males and 61,255 females [61]. There are 28,643 households, with 10,663 in Kanepokhari and 17,980 in Patharisanischare. The literacy rates in Patharisanischare (81.5%) and Kanepokhari (77.8%) are slightly higher than the national average of 76.2%. Patharisanischare has 10 health facilities (1 municipal level hospital, 2 health posts, and 7 rural health centers), while Kanepokhari has 7 health facilities (1 municipal level hospitals, 2 health posts, and 4 rural health centers). The number of FCHVs in Kanepokhari (n = 24) is slightly lower than in Patharisanischare (n = 30).
Study design
This is a single-blinded, individually randomized factorial trial. Behaviour change interventions are complex due to the many interacting components involved [15]. While traditional randomized controlled trial (RCT) designs are considered the gold standard for evaluating the impact of an intervention, they typically do not identify which specific components contribute to desired outcomes [13]. In contrast, factorial design enables the assessment of individual intervention components and their interactions [36]. This approach is appropriate for enhancing the effectiveness, efficiency, and cost-effectiveness of an intervention, ultimately facilitating its scalability to benefit a large population [14].
In this study, we will utilize a Multiphase Optimization Strategy (MOST), an engineering-based approach aimed at effectively optimizing behavioural interventions [13]. MOST comprises three key phases: preparation, optimization, and evaluation. The preparation phase involves developing a conceptual model for the intervention and piloting it to identify “core components” and determine the optimization criteria (e.g. effectiveness, efficiency, cost). The optimization phase utilizes a multifactorial design to conduct a randomized factorial experiment trial using the specific components identified during the preparation phase. Finally, the evaluation phase involves reviewing the trial results and reaching a consensus on the way forward. We will conduct a 2 × 3 factorial individually randomized, single-blinded controlled trial design. Participants detected by Female Community Health Volunteers using the CIDT, will be randomized into one of eight possible combinations of three candidate intervention components ranging from none to all three components (n = 36 in each condition). All participants will receive component one, i.e. information about depression. However, the three candidate intervention components, each with two options, include the following: (a) information about available services (on/off), (b) addressing stigma and discrimination (on/off), and (c) life transformation recovery stories (on/off). All four intervention components will be delivered in person on a one-to-one basis.
Participants and eligibility criteria
The study will be conducted with an adult population. The eligibility criteria for participation in this study include being an adult aged 18 or older residing in Kanepokhari Rural Municipality or Patharisanischare Municipality, those detected through CIDT for depression, providing written consent for participation, and being proficient in speaking and understanding Nepali. Participants receiving mental health services will be excluded from the study. In Nepal, FCHVs, the lowest level of health workers, will receive training to incorporate CIDT into their regular responsibilities. When FCHVs encounter someone in the community matching the narrative, they ask two additional questions about the impact of the condition on daily activities and the individual’s willingness to seek help [31]. If the person meets the criteria and responds positively to at least one of the two questions, FCHVs will schedule the Gain Life intervention.
Recruitment
Participants will be purposefully recruited through a systematic process. Trained FCHVs will identify potential participants who meet the CIDT criteria, such as individuals whose personal experiences align significantly with the CIDT story, exhibit impaired daily functioning, and express a need for support. Once identified, FCHVs will provide the details (age, gender, location) of individuals who meet CIDT criteria to their supervisor via a phone call. The supervisors will assess the eligibility criteria (i.e. 18 years or older, ability to speak, and CIDT threshold) and send the case details to the first author (NPL) for randomization.
Bi-monthly group meetings will be held for FCHVs to share their progress, discuss challenges encountered during the implementation of the CIDT, and provide motivation. Supervisors will also conduct field visits to offer immediate feedback and enhance FCHVs’ skills in utilizing the CIDT to ensure an effective recruitment strategy.
Sample sizes and sampling process
The sample size for this study was determined based on the need to detect a difference in help-seeking behaviour between participants receiving the mental health literacy component (i.e. information about depression) alone (40%) and those receiving both the mental health literacy and stigma, myths, and facts about depression components (60%) [32, 53]. With 90% power and a significance level of 0.05, a total sample size of 288 participants is required, with 36 participants per condition. This sample size will allow to determine which component of the Gain-Life intervention positively impacts the primary outcome of help-seeking behaviour among individuals with depression.
Randomization
Participants will be randomly assigned to one of eight treatment conditions based on four factors: (i) information on depression, (ii) available treatments, (iii) stigma reduction through myths and facts, and (iv) life transformation experiences. Using Microsoft® Excel (Version 16.86), a list of random numbers between one and eight with no duplicates was generated for each FCHV. As the FCHVs enrol participants, the first author assigns the next random number on their list to each participant, indicating the allocated treatment condition. Because each FCHV will recruit between 8 and 10 participants and there are only 8 treatment conditions, some FCHVs ended up delivering each condition at least once, and some conditions will be delivered twice. The table below summarizes the allocation of participants into different intervention components.
The first author will randomize each case using a computer-generated random table and assign them to one of the eight factors presented in Table 1 below. The randomization will be conducted separately for each FCHV to ensure cases are allocated to all 8 factors. The first author will inform the supervisors of the randomization results within 24 h. The supervisors will then inform FCHV which intervention or combination of interventions should be delivered to each case via a phone call. Table 1. Random allocation of participants into different intervention componentsExperimental condition/factorsInformation about depressionInformation about available servicesStigma reductionRecovery story (video)Sample size1**✓✓✓✓362✓✓✓363✓✓✓364✓✓365✓✓✓366✓✓367✓✓368✓**36
Blinding
Data collectors conducting baseline and follow-up interviews will remain blinded. The Principal Investigator (PI), trainers/supervisors, FCHVs, and participants will not be blinded to the treatment conditions. The PI, who is responsible for managing the study, randomizing participants, and supervising field activities including quality control, will not be blinded to the treatment condition. The statistician, who analyzes the quantitative data for the study, remains blinded (Fig. 1). Fig. 1. Recruitment process map
Assessing and addressing harms
While this study carries a low risk, discussing mental health issues may be distressing for some participants. To mitigate these risks, we will provide access to trained counselors who can effectively handle such situations and make referrals to health care facilities if needed. Participants who report self-harm or suicidal thoughts will be promptly referred to counselors for immediate support.
Description of the intervention
Previous studies have shown that mental health literacy is associated with help-seeking behaviour, suggesting that improved mental health literacy can increase the likelihood of seeking help [29, 72]. Similarly, several studies have found that higher levels of stigma, particularly related to seeking help for mental health issues and personal stigma, are significantly linked to reduced active help-seeking behaviour [21, 68]. A formative study identified lack of information about available services, lack of knowledge about mental health problems, and lack of support from family members as major barriers to seek care for mental health issues. Therefore, the Gain Life intervention was developed based on the evidence from previous studies and the formative study results. The intervention comprises four components: mental health literacy, stigma reduction, information on available services, and a video featuring a service user’s recovery story. Workshops were conducted with psychologists, psychosocial counsellors, and individuals implementing mental health interventions in the community to develop and finalize the contents for these components. The draft intervention was pilot tested with ten FCHVs in a different district to gather their feedback on the content, delivery mechanism, training duration and methods, and supervision needs.
Information about depression
The aim of this component is to raise awareness about depression, with a particular focus on its causes, manifestations, and the potential negative consequences of untreated depression. Previous studies have indicated that the causes of depression are often linked to stressful life events, socio-cultural factors, and genetic predispositions, rather than solely biological factors. In this component, we have highlighted various contextual factors, including cultural practices and beliefs, stressful life events such as natural disasters (e.g. earthquakes, landslides), economic hardships, changes in family structures, family stress, educational stress, genetic influences, social discrimination and exclusion, substance abuse, and chronic illnesses like cancer and HIV/AIDS.
In addition to the common symptoms of depression outlined in standard guidelines, we have included culturally and context-specific symptoms frequently reported by individuals with depression in Nepal, such as stomach-ache, headaches, unexplained body pains, and tingling sensations. Research has shown that individuals are more likely to seek care for their illness if they understand the negative consequences of leaving it untreated. Therefore, we have included information on the potential consequences of untreated depression, which can range from difficulties in daily activities and increased chronicity of the illness to reduced treatment effectiveness and higher treatment costs. This component is designed as a flipchart with animated images to engage participants. FCHVs can use the flipchart on a table or in a planned space, turning the pages to display images on participants’ side and the page containing the content on their side.
Information about available services
The second component of the intervention provides detailed information about mental health services available in the community, district, and neighbouring districts. This includes the types of services offered, costs, distance to service providers, and operating hours. Lack of knowledge about available services has been identified as a barrier to seeking mental health care. Studies have shown that patients often do not know where to seek help and may resort to traditional healers or avoid seeking care altogether. However, mental health services are now accessible in primary and community health care facilities through a task-sharing approach. The aim of this intervention component is to address the lack of awareness about available services and assist individuals in identifying suitable sources of support. It encompasses all treatment options, including primary health care providers who are on the mental health Gap Action Program (mhGAP) intervention guide and municipal hospitals, as well as specialist services within the district and neighbouring districts. This component is being produced as a booklet with images of specific health facilities and their surroundings on one side, and descriptions of available services and services that are not available on the other side. This format helps FCHVs associate the images with available services while implementing the component.
Stigma, myths and facts about depression
The purpose of this component is to address stigma and misconceptions surrounding depression by addressing the root causes of stigma, dispelling myths, and providing accurate information about depression. The component covers the stigma surrounding mental health issues, common stigmatized behaviours experienced by individuals with depression, and how stigma and discrimination can hinder help-seeking behaviour. The second part of the component focuses on debunking prevalent myths about depression and presenting the facts. This information is presented in a table format, with one column listing myths and another column providing factual information. The component is designed as a wall calendar with animated images to enhance understanding, particularly for participants with reading difficulties. FCHVs can use the calendar to display information on a wall or facilitate discussions by connecting the text with corresponding images.
Recovery stories of persons with lived experience
The final component of the Gain Life intervention showcases recovery stories of individuals who have triumphed over depression. This component comprises two 8-min video stories featuring individuals who successfully recovered from depression. The first video narrates the story of a woman from Parbat, a district in mid-western Nepal, who overcomes depression by seeking treatment from various sources and receiving ongoing care from primary health care facilities near her home. She was a person with lived experience trained in PhotoVoice to create a recovery narrative [44]. She also received support from psychosocial counsellors and her family. The second story is about a young man who battled depression and suicidal thoughts, surviving a suicide attempt and eventually opening up to his family, especially his parents, about his struggles. The video demonstrates how this young man overcame depression with the help of his parents, mental health professionals, and his own determination. FCHVs show the videos on a tablet and discuss them briefly with each participant. They focus on the individuals’ problems, symptoms, types of services received, and the crucial role of family members in the treatment process and recovery.
Training
Training to FCHVs
FCHVs will receive a 5-day training that includes the Community Informant Detection Tool (CIDT) and the Gain Life intervention. The first part of the training will cover basic concepts of mental health, reasons for underutilization of mental health services, and the CIDT’s purpose of identifying individuals with depression. FCHVs will learn to use vignettes for detection, recognize symptoms, and assess the need for depression support. Role-playing exercises will emphasize seeking help and involving family members.
The second part of the training will focus on the Gain Life intervention, covering theoretical and practical aspects. FCHVs will learn about mental health problems, depression, causes, symptoms, consequences of untreated depression, available mental health services, stigma associated with mental health problems, and strategies to reduce stigma. Role-playing activities in small groups will help FCHVs gain confidence in implementing the intervention effectively.
Training to primary health care providers
Primary health care workers in Kanepokhari and Pathari-sanischare municipalities have not received training on mental health. Therefore, they will undergo a 5-day mhGAP training based on the module developed by the government of Nepal. The training will focus on the assessment, diagnosis, and management of mental health conditions such as depression, psychosis, alcohol use disorder, epilepsy, anxiety, and child and adolescent mental and behavioural problems. The training will be conducted by a psychiatrist and a psychologist. Female Community Health Volunteers (FCHVs) who receive training in the Gain Life intervention will provide information on the services available in the health facilities where health workers are trained on mhGAP.
Implementation process of Gain Life intervention
FCHVs will utilize the CIDT in their daily tasks to identify individuals experiencing depression. They will initially consider individuals whose experiences resonate with the CIDT vignette. Upon identifying a potential candidate, FCHVs will engage in a consultation to evaluate the impact of the issue on the individual’s daily life and their readiness to seek assistance. If the individual agrees to participate in the Gain Life intervention, FCHVs will arrange a suitable date and time for its implementation.
As per the study protocol, participants may receive all four components of the Gain Life intervention or a combination of three, two, or one component. FCHVs will coordinate the intervention implementation accordingly, with a maximum of two components being delivered simultaneously. In cases where three components are required, they will be administered on separate days. The intervention sessions will take place in confidential settings, such as the participant’s or FCHV’s residence, to ensure privacy. While family members are encouraged to join, participants who prefer not to involve them can opt for individual sessions.
Participants may choose not to receive all allocated components of the intervention for reasons such as feeling that they do not need the additional components, starting treatment after receiving initial components, or other contextual factors. These participants will still be included in the analysis using an intention-to-treat approach. Additionally, there will be no restrictions on participants receiving other interventions, support, or attending awareness programmes. These aspects will be explored in the qualitative component of the intervention.
Supervision of FCHVs
Trained FCHVs will receive regular supervision from psychosocial counsellors in three ways. Firstly, they will participate in group supervision sessions twice a month to discuss challenges encountered while implementing CIDT and Gain Life interventions. The psychosocial counsellor will offer practical guidance and skills to address these challenges. Group supervision sessions will be held separately for FCHVs in Kanepokhari Rural Municipality and Patharisanischare Municipality. Secondly, each FCHV will undergo two live supervisions per month, during which the counselor will observe a Gain Life session. These sessions will only be observed if the participant or their family member feels comfortable. Lastly, the psychosocial counsellors will contact each FCHV before implementing the intervention to ensure they are using the correct components as allocated randomly.
Outcome measures
Primary outcome
Help-seeking behaviour
Changes in help-seeking behaviour will be assessed by determining if participants sought mental health treatment within one month after attending the FCHVs intervention. Mental health treatment is defined as treatment provided by health care providers including trained primary health care workers, doctors, and mental health specialists. This does not include treatment provided by traditional healers and religious leaders. Research assistants, who are unaware of the participants’ assignment to the intervention, will visit their homes one month post-intervention. They will inquire about the participants’ interactions with FCHVs, the places/providers they visited for seeking care, and the reasons for choosing a specific provider using a semi-structured questionnaire. We will not verify the accuracy of the treatment they received. Participants who did not seek treatment will also be asked about the reasons for not seeking care and their plans to seek treatment soon. Participants will be asked a “yes” or “no” question: “Did you seek help for your health issue after attending the FCHV session?” with a yes or no response. We will report the percentage of participants who respond “yes” to this question as an indicator of seeking treatment.
Secondary outcome
Treatment adherence
Treatment adherence will be monitored by following up with participants for three months after they start treatment. The three-month follow-up period was chosen based on feasibility and previous studies [17, 33]. Participants who begin treatment one month after the FCHVs intervention will be followed up after three months to evaluate their ongoing care. During the follow-up, participants will be asked if they are still receiving care from the same providers, if they have switched providers, or if they have stopped treatment. Participants who switched providers will be asked about the reasons for the change, while those who discontinued treatment will be asked about the reasons for their decision to stop receiving services. Participants will be asked “yes” or “no” questions: “Have you been receiving treatment for your health issues since we last met three months ago?” We will report the percentage of participants who respond “yes” to this question as an indicator of treatment adherence.
Mediators
We will examine the mediating effects on help-seeking behaviour at the three-month follow-up. The mediating variables include knowledge, attitude, and perception of depression, as well as the severity of depressive symptoms. These mediating variables were selected based on the impact of these knowledge, attitude, and perception of depression on help-seeking [10, 11, 29, 69].
Knowledge, attitudes, perceptions of depression and available services
Participants’ knowledge, attitudes, and perceptions regarding depression and available services will be assessed during a three-month follow-up. Three structured questionnaires, each with four response options, have been developed based on the intervention content. The knowledge about depression scale consists of 7 items, the stigma and myths scale consists of 5 items, and the knowledge about available services scale consists of 8 items. These scales will be asked during the three-month follow-up, not at baseline. Each question will have one correct response and three incorrect responses. Participants will choose the correct response for each question after a research assistant reads the question and all possible responses. Composite scores will be calculated based on the number of correct responses for each scale for analysis. We will report the number of correct responses in each domain: knowledge, attitudes, and perceptions on depression. Additionally, we will also use continuous scores (i.e. total score of each domain) when performing mediator analysis.
Symptom severity
The severity of depression symptoms will be assessed using the locally validated Patient Health Questionnaire (PHQ-9) three months after treatment initiation. The PHQ-9 is a nine-item tool commonly used to evaluate depression symptoms. Participants will rate nine common symptoms of depression based on their experiences over the previous two weeks using a 4-point scale ranging from 0 (not at all) to 3 (always) [24]. The PHQ-9 has been translated, culturally adapted, and validated in Nepal with a sensitivity of 0.94 and specificity of 0.80 for the recommended cut-off score of ≥ 10 for screening individuals with depression [42]. We will use the total scores of the PHQ-9, which range from 0 to 27, to examine the mediating effects of depression symptom severity in individuals seeking help. A higher score on the PHQ-9 indicates a more severe level of depression [24].
Implementation measures
Data on fidelity, feasibility, acceptability, and appropriateness of the intervention delivered by FCHVs in community settings will be collected for each intervention component and delivery strategy.
Fidelity of the implementation of Gain Life
Fidelity in implementing the components and combination of components in the Gain Life intervention will be assessed by two supervisors. They will observe sessions and engage with Female Community Health Volunteers (FCHVs) within 24 h of the intervention. A structured fidelity checklist will be utilized to evaluate the skills, content, and delivery methods of each intervention component. The checklist is based on the content and delivery methods outlined in different components of the intervention. It will ascertain if FCHVs covered all the methods and content in a particular component, and if they incorporated content from other components not included in that session. Supervisors will observe at least two sessions of each FCHV, and two fidelity checklists will be completed through discussions with the FCHVs within 24 h of the intervention.
Feasibility, acceptability and appropriateness
The feasibility, acceptability, and appropriateness of the intervention will be evaluated using qualitative methods, including individual interviews (IDIs) and focus group discussions (FGDs). FGDs will involve Female Community Health Volunteers (FCHVs) who implemented the intervention to assess their experience with using the CIDT to identify individuals with depression and implementing the Gain Life intervention. Each focus group will include six to eight FCHVs.
Individual interviews will be conducted with three participant groups: those who did not receive treatment, those who started but discontinued treatment, and those who are still receiving care three months after participating in the Gain Life intervention. Some interviews will also involve family members who attended the intervention. Interviews with participants who did not start the intervention will take place two months after their participation, while interviews with the other two groups (those who dropped out and those still receiving care) will occur after a three-month follow-up period.
Process evaluation
The implementation process, including training and supervision of FCHVs, as well as barriers and facilitators of the intervention, will be documented by a separate individual through observation of training and supervision sessions and interviews with supervisors.
Data management and analysis
Quantitative data will be collected using an Android tablet with questionnaire applications. The data will be stored in the TPO Nepal server. Data collected on the ODK platform will be transferred to the TPO Nepal server, and any inconsistencies in data collection will be monitored regularly by the research supervisor. Inconsistencies and errors in the data will be minimized manually.
Quantitative data analysis
Quantitative data analysis will be conducted using StataIC 15.1 and MPlus (v8) [60]. Baseline characteristics of the participants (such as age, sex, caste/ethnicity, education) will be compared to assess balanced randomization. An intent-to-treat model will be used. Participants who do not receive all allocated intervention components for various reasons will be included in the intent-to-treat analysis. Despite the short three-month interval between the baseline and follow-up interviews, there is a risk of participant dropout during the follow-up period, possibly due to work-related mobility. To address this issue, we also plan to conduct the follow-up interviews via phone to minimize the risk of dropout. Any missing data or loss to follow-up will be carefully examined, and if necessary, we will utilize multiple imputation techniques to handle missing data effectively.
Primary outcome
As recommended for factorial designs, effect coding will be utilized for all analyses [13]. The primary outcome of interest is change in help-seeking behaviour. This will be evaluated by determining the proportion of participants who attended the Gain Life intervention and sought care from health care providers rather than traditional or religious leaders. This will be measured by the number of participants who received the Gain Life intervention and sought treatment from health care providers. General linear regression models will be used to test the main effects of the Gain Life intervention components and their association with the primary outcome of interest [52].
Secondary outcomes
Our secondary outcome is treatment adherence for depression care. This will be determined based on the number of participants who initiate treatment one-month post-intervention and continue to engage in care during the three-month follow-up period. General linear regression models will be used to test the secondary outcomes as well.
Mediators
Previous studies have demonstrated a positive correlation between mental health literacy, attitudes, stigma, and symptom severity in relation to help-seeking behaviour [10, 11, 29, 69]. Our formative study also indicated that individuals who were familiar with depression symptoms and aware of mental health service providers and locations were more inclined to seek help from health care providers. Therefore, we aim to investigate whether participants’ knowledge, attitudes, and stigma can act as mediators in influencing help-seeking behaviour. Furthermore, we will also assess the symptom severity of depression, as measured by the PHQ-9 at a three-month follow-up, to determine if it plays a mediating role in help-seeking behaviour. We will use the Baron and Kenny method along with a path analysis to examine the mediation effects. For the Baron and Kenny method, a series of general linear regression models will be tested to assess mediation [49]. Mplus will be used to conduct a path analysis looking at the direct and indirect effects to determine if the hypothesized mediator is in fact a mediator in the relationship between the predictor variable and outcome of interest [19].
Moderators
We will assess how socio-demographic factors such as caste/ethnicity, age, gender, education level, occupation, and religion moderate the intervention’s impact through general linear regression models and interaction variables. Previous studies in Nepal have shown that gender, caste/ethnicity, and occupation can affect rates of depression and anxiety [39, 48]. These analyses are crucial for promoting equitable access to mental health care in Nepal.
Qualitative data analysis
Each interview or focus group discussion will be recorded and transcribed in Nepali immediately after the fieldwork. The transcripts will then be translated into English for analysis by a skilled translator. Two members of the research team will independently code 10% of the interviews or focus group discussions following the CFIR guidelines. A review of all the codes for each interview will be carried out until the research team members reach a consensus on the codes to be applied to specific text segments. Once consensus is reached, interview transcripts will be entered, coded, and analyzed in NVIVO.
Dissemination
We will share the results with key stakeholders in Kanepokhari Rural Municipality and Patharisanischare Municipality. Additionally, we will organize a dissemination programme in Kathmandu for stakeholders involved in mental health, including senior officers from the Ministry of Health and Population, representatives from non-governmental organizations, international non-governmental organizations, and other civil society organizations. The study findings will also be published in academic journals.
Timeline
The training of FCHVs on CIDT and on Gain Life intervention began in May. They began implementing CIDT and the intervention in June. Data collection for the baseline survey commenced in July 2024. The enrollment and assessment schedule, following the SPIRIT guidelines, is outlined in Fig. 2 below. The protocol was developed in strict adherence to the Standard Protocol Items: Recommendations for Intervention Trials 2013 (SPIRIT) guidelines [6].Fig. 2. Schedule of enrolment, interventions, and assessments
Discussion
In this study, we utilized the MOST framework to optimize a community-based intervention aimed at increasing help-seeking for depression care. Through a factorial design, our goal is to develop an effective intervention that raises awareness about depression, available services, and reduces stigma. The study will examine the impact and interaction of intervention components such as depression information, treatment awareness, dispelling myths, and life transformation experiences. The primary outcome will be changes in help-seeking behaviour, with treatment adherence as a secondary outcome.
The strengths of our study include the following: (i) the use of multiple methods and stakeholders in the development of the intervention, such as a systematic review, formative study, consultative workshops with various stakeholders, and pilot testing with a group of 10 FCHVs in another district; (ii) while most global mental health research focuses on developing and evaluating interventions to address supply-side barriers, this study targets demand-side barriers by using the innovative study design MOST, enabling us to evaluate the effectiveness of intervention components through an iterative optimization process; and (iii) the implementation of the intervention and study in multicultural, multilingual, and multi-ethnic communities in eastern Nepal, allowing for generalization of results throughout Nepal.
We anticipate challenges in maintaining intervention fidelity, as participants may seek additional information from FCHVs beyond what is included in the intervention packages or in a particular component. Additionally, ensuring fidelity in delivering the core components and the combination of intervention packages by the same FCHVs may be challenging. To address this, fidelity checklists will be used to guide delivery, and regular supervision sessions will be conducted to support FCHVs in maintaining fidelity.
The study has some limitations, including being single-blinded, with only RAs and the statistician blinded to the study allocation. We have included four intervention components, including information about depression as the core component and three candidate components, due to resource constraints. There may be other factors influencing help-seeking for depression that were not included in this study. The results will guide decisions on progressing to a fully powered randomized controlled trial and further optimization with new intervention components.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Chowdhary N, Anand A, Dimidjian S, Shinde S, Weobong B, Balaji M, Patel V. The Healthy Activity Program lay counsellor delivered treatment for severe depression in India: systematic development and randomised evaluation. Br J Psychiatry. 2015. 10.1192/bjp.bp.114.16107510.1192/bjp.bp.114.161075 PMC 481697426494875 · doi ↗ · pubmed ↗
- 2Jordans M JD, Kohrt BA, Luitel NP, Komproe IH, Lund C. Accuracy of proactive case finding for mental disorders by community informants in Nepal. Br J Psychiatry. 2015;207(6):501–6.10.1192/bjp.bp.113.141077 PMC 466485626450582 · doi ↗ · pubmed ↗
- 3National Statistics Office. National Population and Housing Census 2021 Accessed through https://censusnepal.cbs.gov.np/results/literacy on 30 April 2023. 2023. Kathmandu, Nepal: Government of Nepal, Office of the Prime Minister and Council of Ministers.
- 4WHO. mh GAP intervention guide for mental, neurological and substance use disorders in non-specialized health settings: mental health Gap Action Programme (mh GAP) – version 1.0. Geneva, Swizerland: WHO. 2010.23741783 · pubmed ↗