Successful Control of Chemotherapy-Induced Breakthrough Hemolysis With Ravulizumab in a Patient With Paroxysmal Nocturnal Hemoglobinuria During Carboplatin-Pemetrexed Treatment for Lung Adenocarcinoma
Atsushi Takahata, Keisuke Tanaka, Shigeo Toyota

TL;DR
A patient with PNH and lung cancer successfully managed chemotherapy-induced hemolysis using ravulizumab, allowing continued treatment and extended survival.
Contribution
Demonstrates effective use of ravulizumab for chemotherapy-induced breakthrough hemolysis in PNH patients undergoing cancer treatment.
Findings
Ravulizumab normalized lactate dehydrogenase and raised hemoglobin levels in a PNH patient.
Personalized ravulizumab scheduling enabled 14 chemotherapy cycles without transfusion or thrombosis.
The patient achieved a PFS of two years and five months, exceeding the median for this regimen.
Abstract
Paroxysmal nocturnal hemoglobinuria (PNH) is a rare hematologic disorder characterized by complement‑mediated intravascular hemolysis. Although breakthrough hemolysis (BTH) is typically triggered by infections or surgery, chemotherapy-induced BTH is seldom reported, and optimal management strategies during cytotoxic cancer therapy remain undefined. We report a 52‑year‑old man with longstanding PNH who developed stage IVA epidermal growth factor receptor‑mutated lung adenocarcinoma. After discontinuing first‑line osimertinib due to diarrhea, second‑line carboplatin-pemetrexed (chemotherapy regimen consisting of carboplatin and pemetrexed) induced severe BTH, evidenced by lactate dehydrogenase rising to 2,462 U/L and hemoglobin (Hb) dropping to 4.6 g/dL. Introduction of ravulizumab promptly normalized lactate dehydrogenase (<250 U/L), raised Hb to 10.5 g/dL, and suppressed total hemolytic…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1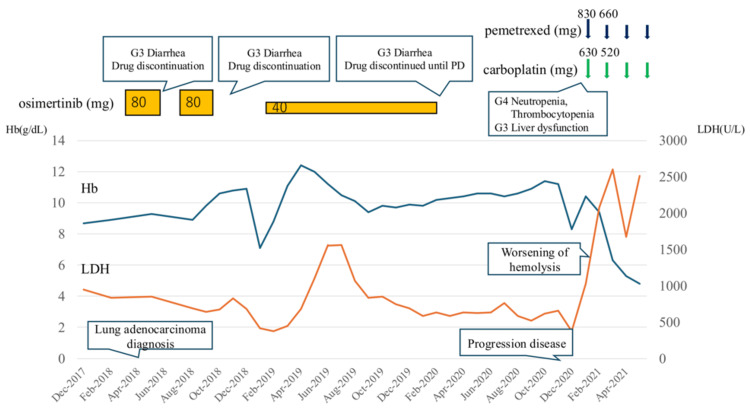 Figure 2
Figure 2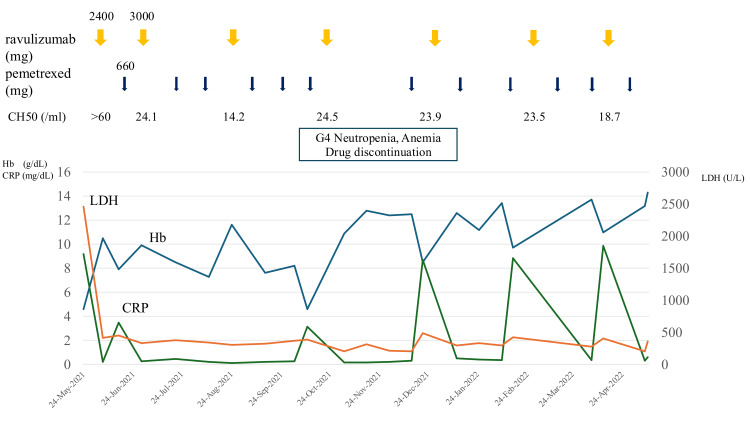 Figure 3
Figure 3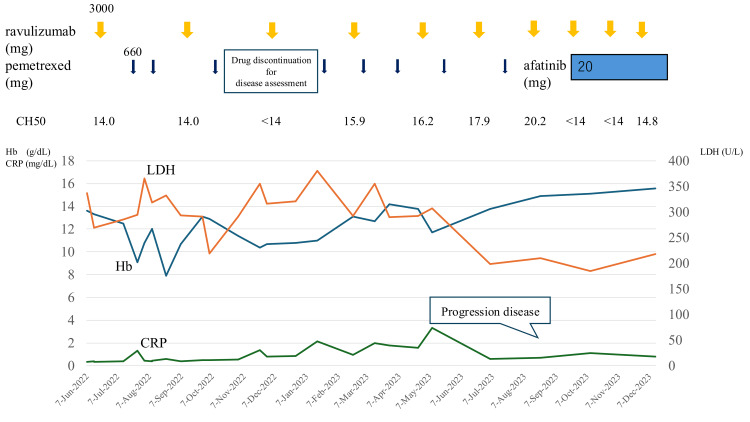 Figure 4
Figure 4| Investigations | Results | Normal range |
| WBC (/μL) | 2,800 | 3,900-9,800 |
| RBC (×10⁴/μL) | 133 | 427-570 |
| Hb (g/dL) | 4.6 | 13.5-17.6 |
| Plt (×10⁴/μL) | 10.6 | 15.8-34.8 |
| Reticulocyte (%) | 1.7 | 0.2-2.7 |
| TP (g/dL) | 6.7 | 6.5-8.0 |
| Alb (g/dL) | 6.7 | 6.5-8.0 |
| AST (U/L) | 120 | 13-35 |
| ALT (U/L) | 20 | 13-35 |
| LDH (U/L) | 2,462 | 124-222 |
| T-Bil (mg/dL) | 2.7 | 0.3-1.2 |
| D-Bil (mg/dL) | 0.2 | 0-0.2 |
| BUN (mg/dL) | 13 | 8.0-22.0 |
| Cre (mg/dL) | 0.98 | 0.60-1.10 |
| Haptoglobin (mg/dL) | 3.8 | 19-170 |
| Fe (μg/dL) | 84 | 80-200 |
| TIBC (μg/dL) | 342 | 290-355 |
| Ferritin (ng/mL) | 1,106 | 13-277 |
| C3 (mg/dL) | 124.7 | 73-138 |
| C4 (mg/dL) | 26 | 11-31 |
| CH50 (/mL) | >60 | 30-46 |
| Erythrocytes surface markers | ||
| CD55-/CD59- (%) | 14.9 | - |
| CD55-/CD59+ (%) | 3 | - |
| CD55+/CD59- (%) | 0 | - |
| CD55+/CD59+ (%) | 82.1 | - |
| Study | Cancer type | Cancer treatment | PNH status | PNH treatment/outcome | Cancer outcome |
| Lim et al. [ | Cancer of unknown primary | Carboplatin-paclitaxel + erlotinib | Hemolytic crisis diagnosed with PNH | Eculizumab hemolysis markedly suppressed | No recurrence for >8 years (under eculizumab) |
| Sikuyayenga and Karlin [ | Breast cancer | Aromatase inhibitor | Known PNH hemolytic crisis | Supportive care | Not specified |
| Hakim et al. [ | Breast cancer | Bispecific antibody MDXH210 | Hemoglobinuric acute renal failure suggestive of PNH | Not specified | Died from metastatic cancer |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsComplement system in diseases · Lung Cancer Research Studies · Adenosine and Purinergic Signaling
Introduction
Paroxysmal nocturnal hemoglobinuria (PNH) is a clonal hematopoietic disorder caused by a somatic phosphatidylinositol glycan class A mutation, leading to a deficiency of glycosylphosphatidylinositol (GPI)-anchored proteins, such as CD55 and CD59 [1]. Epidemiologic surveys report an incidence of 0.08-0.57 per 100,000 person-years and a prevalence of 38 per million [1]. Loss of these surface proteins leads to complement-mediated hemolysis, thrombosis, and marrow failure. Hemolysis in PNH is primarily driven by activation of the alternative complement pathway. Complement activation, exacerbated by stressors such as infection or surgery, can lead to breakthrough hemolysis (BTH) [2]. In advanced lung adenocarcinoma, particularly in cases harboring epidermal growth factor receptor (EGFR) gene mutations, EGFR tyrosine kinase inhibitors (EGFR-TKIs) are the standard first-line therapy. However, for patients who develop resistance or intolerance to EGFR-TKIs, platinum-based chemotherapy remains a key option. Combination therapy with carboplatin (chemotherapy regimen consisting of carboplatin, CBDCA) and pemetrexed (PEM) is an established standard regimen for advanced nonsquamous non-small cell lung cancer (NSCLC). In EGFR mutation-positive NSCLC resistant to EGFR-TKIs, the median progression-free survival (PFS) and overall survival with this regimen have been reported as 5.5 and 14.7 months, respectively [3]. This case report describes a patient with PNH who developed BTH induced by essential chemotherapy for life-threatening lung cancer. The introduction of ravulizumab, a complement C5 inhibitor, not only controlled hemolytic episodes but also coincided with an unexpectedly prolonged disease control of the lung cancer. This report describes a rare case and reviews the management of chemotherapy-induced BTH in PNH.
Case presentation
A 52-year-old man with PNH diagnosed in his 30s had been observed without treatment. In May 2018, he developed exertional dyspnea, and a chest computed tomography (CT) scan in August revealed massive left-sided pleural effusion. Pathological examination of the pleural fluid led to a diagnosis of stage IVA EGFR-mutated lung adenocarcinoma. Osimertinib was initiated as first-line therapy in September 2018; however, frequent Grade 2-3 diarrhea made continuation difficult. In November 2020, following the discontinuation of osimertinib, a chest CT scan demonstrated enlargement of the primary lesion and new lymph node metastases. Consequently, combination chemotherapy with CBDCA and PEM was initiated as second-line treatment in December 2020. From February 2021, hemolytic parameters began to worsen, and by May 2021, laboratory tests showed a marked increase in lactate dehydrogenase (LDH) (peak: 2,462 U/L), a decrease in hemoglobin (Hb) (nadir: 4.6 g/dL), and elevated total bilirubin (peak: 2.7 mg/dL), leading to a diagnosis of BTH. The patient was hospitalized in May 2021 and started on ravulizumab. Key admission findings included marked anemia (Hb 4.6 g/dL), significantly elevated LDH (2,462 U/L), and low haptoglobin (3.8 mg/dL). Flow cytometry revealed a PNH red blood cell clone (CD55-/CD59-) comprising 14.9%. Total hemolytic complement activity (CH50) was elevated (≥60 U/mL), indicating robust complement activation. Chest CT demonstrated an irregular left upper lobe lesion, left-sided carcinomatous pleurisy, and left hilar lymphadenopathy. These laboratory and imaging findings at the time of ravulizumab initiation are presented in Table 1 and Figure 1.
Chest CT at the time of ravulizumab initiation showing an irregular left upper lobe mass, carcinomatous pleurisy, and left hilar lymphadenopathy (yellow arrows)CT: computed tomography
Following the initiation of ravulizumab, hemolytic findings improved rapidly. LDH decreased to approximately 250 U/L, and Hb recovered to 10.5 g/dL without transfusions. CH50 stayed below 14 U/mL. With hemolysis suppressed, PEM chemotherapy was safely resumed on an outpatient basis. However, mild hemolysis still occurred at the start of chemotherapy. Based on the observed pattern of hemolysis, the administration schedule was adjusted to give ravulizumab prior to each cycle of chemotherapy, which effectively prevented further hemolytic episodes. Two years and five months after starting CBDCA-PEM therapy, disease progression of the lung adenocarcinoma was confirmed by imaging studies. This duration substantially exceeded the median PFS of approximately 5.5 months for this regimen in previously treated advanced nonsquamous NSCLC [4]. In June 2023, afatinib was started. After this change, both Hb and LDH levels normalized, strongly suggesting that CBDCA, PEM, or both had triggered the BTH. The clinical course is summarized in Figures 2-4.
Clinical course of the patient, showing the period from lung cancer diagnosis, initial chemotherapy with osimertinib, and subsequent carboplatin plus pemetrexed leading to worsening hemolysis and introduction of ravulizumabHb: hemoglobin; LDH: lactate dehydrogenase; PD: progression disease
Clinical course of the patient, showing the initial phase after ravulizumab introduction, with continued pemetrexed administration (Pem→Rav sequence) and associated hematological changesHb: hemoglobin; CRP: C-reactive protein; LDH: lactate dehydrogenase; CH50: total complement activity
Clinical course of the patient, showing the later phase demonstrating the optimized sequence of ravulizumab prior to pemetrexed (Rav→Pem sequence), long-term disease control, eventual progression, and subsequent treatment with afatinibHb: hemoglobin; LDH: lactate dehydrogenase; CRP: C-reactive protein; CH50: total complement activity
Discussion
BTH precipitated by cytotoxic chemotherapy is rarely reported in PNH; we identified only three published cases (Table 2) [4-6].
These reports suggest that cytotoxic chemotherapy, particularly regimens with pronounced myelosuppressive or proinflammatory effects, can precipitate BTH or reveal previously subclinical PNH. Inflammatory stress appears central to chemotherapy-induced BTH, as cytotoxic agents can promote the release of proinflammatory cytokines and induce systemic responses. Both CBDCA and PEM have been shown to upregulate proinflammatory cytokines and polarize macrophages toward an M1-like phenotype in vivo [7-9]. Such cytokine surges can amplify the activation of the alternative complement pathway, lowering the threshold for intravascular hemolysis in PNH. In our case, a sharp rise in C-reactive protein accompanied each episode of worsening hemolysis, supporting an inflammation-driven mechanism. Persistent complement activation was also reflected by a CH50 level of ≥60 U/mL on admission. These observations indicate that systemic inflammatory responses to cytotoxic chemotherapy can act as a potent trigger for BTH in susceptible individuals with PNH. Local acidosis represents an additional, noninflammatory mechanism that can precipitate BTH. The classical Ham test demonstrates that complement-mediated lysis of PNH erythrocytes is potentiated at pH 6.5-7. Carboplatin preparations are slightly acidic (pH 5-7), and rapid infusion can transiently reduce systemic or microvascular pH. Such acidification may facilitate assembly of the alternative pathway C3 convertase on GPI-deficient red cells, thereby accelerating intravascular hemolysis. We speculate that chemotherapy-related acidosis and the surrounding inflammatory environment acted synergistically in our patient to produce the unusually severe BTH episode. Prompt and durable C5 blockade proved essential to sustaining chemotherapy in this patient. Ravulizumab, a long-acting monoclonal antibody that blocks cleavage of complement component C5, quickly lowered LDH, raised Hb, and reduced CH50 to <14 U/mL. These laboratory changes show full terminal-complement inhibition and match the responses reported in phase 3 PNH trials [10,11]. After the initial response, mild hemolysis recurred at the start of each chemotherapy cycle. Administering ravulizumab prior to each cycle prevented further episodes, and the patient completed 14 cycles without transfusion or thrombosis. These findings underscore the value of tailored C5 inhibition during cytotoxic therapy in PNH. In this patient, lung adenocarcinoma remained progression-free for two years and five months with CBDCA-PEM plus ravulizumab, well beyond the approximately 5.5 month median PFS reported for this regimen in EGFR-TKI-resistant NSCLC [3]. A comparable case, an eight-year remission after eculizumab in cancer of unknown primary, has been described [4]; however, single-patient observations are insufficient to establish an antitumor benefit from C5 blockade. Complement fragments, especially C5a, reshape the tumor microenvironment in several reinforcing ways. Preclinical studies show that C5a recruits myeloid-derived suppressor cells, redirects macrophages toward an M2 phenotype, and increases vascular endothelial growth factor expression [12-17]. Separately, C5a signaling through C5aR1 on tumor cells can enhance cell survival, foster drug resistance, and facilitate immune evasion [18-20]. It remains unclear whether sustained C5 blockade mitigates these protumor pathways in solid tumors; targeted clinical trials are needed to address this point. Because this report describes only one patient, it remains uncertain whether C5 inhibition was responsible for the prolonged tumor control; other factors, such as the patient’s tumor biology or the CBDCA-PEM regimen itself, may have contributed. Even so, the case demonstrates that ravulizumab can suppress chemotherapy-induced severe BTH and keep treatment on track in PNH. Giving the drug before each cycle proved a practical way to avert additional hemolysis without interrupting therapy. The unusually long PFS observed here, together with the eight-year remission reported after eculizumab [4], indicates that it is worth investigating whether sustained complement blockade confers a direct antitumor benefit. Establishing optimal dosing schedules in cancer-complicated PNH and clarifying whether C5 inhibition adds value on its own or in combination with chemotherapy or immunotherapy represent important goals for future prospective studies.
Conclusions
Ravulizumab rapidly controlled chemotherapy-induced BTH in a patient with PNH, enabling uninterrupted CBDCA-PEM treatment for lung adenocarcinoma. Schedule-adjusted dosing before each cycle prevented further episodes and supported a PFS of two years and five months, far longer than expected for this regimen. Although a single case cannot prove an antitumor effect of complement blockade, the experience highlights the practical value of C5 inhibition during intensive chemotherapy and justifies prospective studies in cancer-complicated PNH.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Paroxysmal nocturnal hemoglobinuria, pathophysiology, diagnostics, and treatment Transfus Med Hemother Panse JP Höchsmann B Schubert J 3103205120243937125110.1159/000540474 PMC 11452172 · doi ↗ · pubmed ↗
- 2Characterization of breakthrough hemolysis events observed in the phase 3 randomized studies of ravulizumab versus eculizumab in adults with paroxysmal nocturnal hemoglobinuria Haematologica Brodsky RA Peffault de Latour R Rottinghaus ST 23023710620213194901210.3324/haematol.2019.236877 PMC 7776354 · doi ↗ · pubmed ↗
- 3Phase III KEYNOTE-789 study of pemetrexed and platinum with or without pembrolizumab for tyrosine kinase inhibitor-resistant, EGFR-mutant, metastatic nonsquamous non-small cell lung cancer J Clin Oncol Yang JC Lee DH Lee JS 402940394220243917309810.1200/JCO.23.02747 PMC 11608596 · doi ↗ · pubmed ↗
- 4Prolonged remission of cancer of unknown primary following initiation of eculizumab therapy for paroxysmal nocturnal hemoglobinuria Case Rep Hematol Lim MY Volmar KE Key NS 2587597201920193135502110.1155/2019/2587597 PMC 6636445 · doi ↗ · pubmed ↗
- 5An unusual case of a hemolytic crisis associated with the initiation of an aromatase inhibitor in a patient with known history of paroxysmal nocturnal hemoglobinuria Cancer Clin Oncol Sikuyayenga M Karlin N 1422013
- 6Development of paroxysmal nocturnal hemoglobinuria after chemotherapy Blood Hakim F Childs R Balow J 47254726151996 https://doi.org/10.1182/blood.V 88.12.4725.bloodjournal 881247258977267 · pubmed ↗
- 7Low-dose carboplatin modifies the tumor microenvironment to augment CAR T cell efficacy in human prostate cancer models Nat Commun Porter LH Zhu JJ Lister NL 53461420233766008310.1038/s 41467-023-40852-3PMC 10475084 · doi ↗ · pubmed ↗
- 8Chemotherapy enriches for proinflammatory macrophage phenotypes that support cancer stem-like cells and disease progression in ovarian cancer Cancer Res Commun Cruz LS Robinson M Stevenson D 26382652420243928756510.1158/2767-9764.CRC-24-0311 PMC 11464072 · doi ↗ · pubmed ↗