Four years on: Pregnancy and birth outcomes reported in the MSBase pregnancy, neonatal outcomes, and Women’s Health Registry (2020–2024)
Vilija G Jokubaitis, Raed Alroughani, Ayse Altintas, Sara Eichau, Stella Hughes, Barbara Willekens, Dana Horakova, Eva Kubala Havrdova, Serkan Ozakbas, Cavit Boz, Mario Habek, Tomas Kalincik, Izanne Roos, Masoud Etemadifar, Marek Peterka, Jeannette Lechner-Scott

TL;DR
This study tracks pregnancy and birth outcomes in women with MS and NMOSD from 2020 to 2024, finding mostly safe results despite DMT use.
Contribution
The first report from the MSBase pregnancy registry provides real-world data on perinatal DMT exposure and pregnancy outcomes.
Findings
Most pregnancies involved DMT exposure within six months preconception, with no overt safety signals observed.
18.1% of pregnancies reported in-pregnancy monoclonal antibody DMT exposure.
Live birth rates were high (85.5%), with most births occurring via unassisted or assisted vaginal delivery.
Abstract
Family planning is an important aspect of multiple sclerosis (MS), and neuromyelitis optica spectrum disorder (NMOSD) management. Knowledge gaps remain, including optimal perinatal management strategies, and fetal risks associated with disease-modifying therapy (DMT) exposure. To describe perinatal DMT use, together with pregnancy and neonatal outcomes prospectively recorded in the International MSBase Pregnancy and Women’s Health Registry. We report summary statistics for data collected between May 2020 and August 2024. A total of 1887 relapsing-remitting MS (RRMS), 12 primary-progressive MS (PPMS), 2 radiologically isolated syndrome (RIS) and 21 NMOSD completed pregnancies were recorded, including 1644 (85.5%) live births, 208 (10.8%) miscarriages, and 6 (0.3%) neonatal deaths. Most women had unassisted (53.8%) or assisted (7.4%) vaginal births. Seventy five percent of pregnancies…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
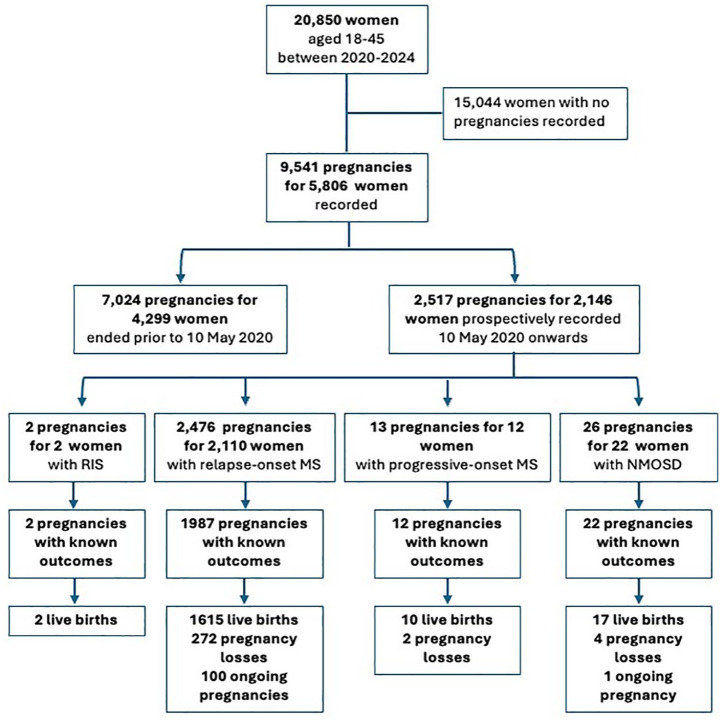 Figure 1
Figure 1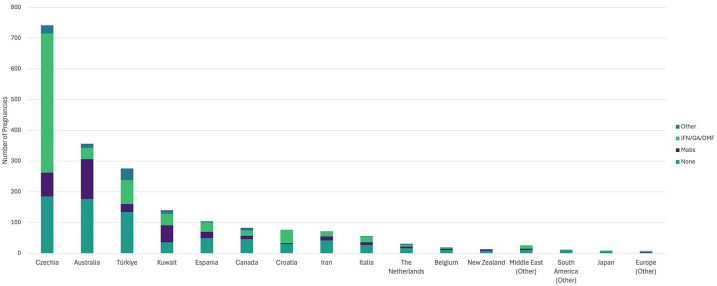 Figure 2
Figure 2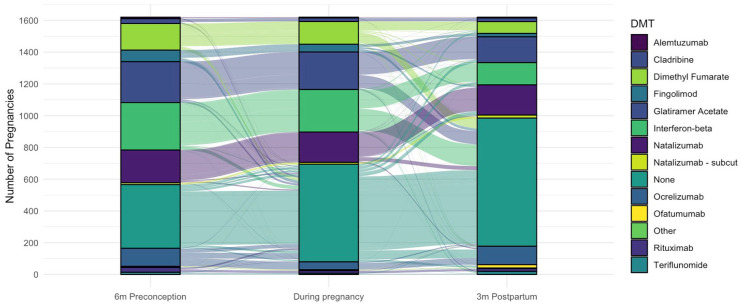 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMultiple Sclerosis Research Studies · Reproductive System and Pregnancy · Pregnancy and Medication Impact
Introduction
Women are disproportionately diagnosed with multiple sclerosis (MS) and related disorders. Women with MS outnumber men by three-fold,^ 1 ^ whereas women with neuromyelitis optica spectrum disorder (NMOSD) outnumber men by nine-fold.^ 2 ^ Commonly diagnosed in their third to fifth decades of life, most women will use disease-modifying therapies (DMTs) for much of their lives. Our understanding of the impact of these conditions, and the use of DMT on women’s health, including fecundity, fertility,^ 3 ^ and pregnancy,^2,4^ together with reproductive aging and menopause^3,5^ is evolving.
The evidence base for the safe and effective use of DMTs perinatally in women with MS is growing, increasing the confidence of neurologists to recommend and prescribe these medications during pregnancy planning and, for some DMTs, in pregnancy. Data from large registries including MSBase,^6,7^ the Canadian,^ 8 ^ Danish,^ 9 ^ French,^ 10 ^ German,^11,12^ Italian,^ 13 ^ and American^ 14 ^ pregnancy registries, as well as purpose-designed studies^ 15 ^ provide critical real-world insights that, in addition to post-marketing pharma-led studies, inform clinical guidelines on the use of these DMT through pregnancy and postpartum.^4,16^ The evidence base around NMOSD and NMOSD DMT use during pregnancy still remains limited, as 2000 exposed pregnancies are ideally required for each DMT to accurately define risks, including rare birth defects.^2,17?–19^
While the international MS outcomes registry MSBase^ 20 ^ has prospectively collected pregnancy-related information since 2004, detailed pregnancy and neonatal outcomes data were not recorded. With the growing number of DMT available to treat MS and NMOSD, the need to capture more detailed data is evident. In response, MSBase launched a prospective Pregnancy, Neonatal Outcomes and Women’s Health Registry^ 21 ^ in 2020. The purpose of this registry is to address the impact of MS and related disorders, together with the impact DMTs on women’s health throughout the lifespan.^ 21 ^ In this first update from our women’s health registry since its launch, we specifically report on pregnancy and birth outcomes in the context of an expanding number of DMT available for the management of MS and NMOSD through pregnancy.
Methods
The MSBase Pregnancy, Neonatal Outcomes and Women’s Health Registry
The MSBase Pregnancy, Neonatal Outcomes and Women’s Health Registry began collecting detailed maternal and neonatal health outcomes on 10 May 2020.^ 21 ^ New data fields include assisted reproductive technology method, pregnancy outcome, obstetric/maternal complications, delivery method, reason for termination/miscarriage, congenital abnormality, birthweight, sex, and breastfeeding data.
Data are collected from 45 countries spanning the northern parts of Africa, North and South America, Asia, Australasia, Europe, and the Middle East.
Study ethics
The Registry is integrated within the MSBase Registry (registered within the WHO International Clinical Trials Registry Platform ID ACTRN12605000455662). The MSBase Registry has ethics approvals or exemptions granted by each participating site’s human research ethics committee. All participants provide informed consent for their de-identified clinical data to be shared with researchers.
Data acquisition and study population
Data were collected during routine outpatient neurology visits and recorded by neurologists or nurses in real-time and therefore reflect real-world clinical care. Data are collected from women of childbearing age with relapse-onset MS (ROMS), progressive-onset MS (POMS), radiologically isolated syndrome (RIS) and NMOSD (both probable and definite).
Definitions
Any woman of childbearing age (18–45 years) actively followed in the MSBase Registry during the observation period was included in the present analysis. Women were classified as actively followed in our registry if they had at least one clinical visit during our observation period between 10 May 2020 (registry launch) and 1 August 2024 (date of data extract). A completed pregnancy refers to any pregnancy that has ended with an outcome reported encompassing live births, miscarriages, terminations, ectopic pregnancies and neonatal deaths.
Statistical methods
We report summary statistics for demographic, clinical, treatment, pregnancy, birth, and neonatal outcomes data collected to-date. All variables were assessed for normality using the Shapiro-Wilk normality test, and reported as means and standard deviations (SD) or as medians and interquartile ranges (IQRs) as appropriate. Categorical data are reported as numbers and percentages.
Data availability statement
MSBase is a data processor, warehousing data from individual principal investigators who agree to share their datasets on a project-by-project basis. Data access to external parties can be granted at the sole discretion of each MSBase Principal Investigator (the data controllers), who will need to be approached individually for permission. To make a request for data access, please contact the corresponding author for instructions.
Results
Patient and pregnancy characteristics
The MSBase Pregnancy, Neonatal Outcomes and Women’s Health Registry^ 21 ^ actively followed 20,850 women of childbearing age between 10 May 2020 and 1 August 2024. Of these 20,850 women, 20,539 had a diagnosis of MS, 40 had a diagnosis of radiologically isolated syndrome (RIS), and 271 had a diagnosis of NMOSD. These women had an average age of 37.3 years (SD 7.1 years) at data extract, with 2411 women now aged between 45 and 49 years. The median follow-up duration for this cohort in the MSBase Registry was 5.25 years (IQR: 1.9, 9.9). The median disease duration at data extract was 8.5 years (IQR: 4.3, 14.0) for women with MS, and 7.2 years (IQR: 2.9, 11.3) for women with NMOSD.
We recorded 9541 pregnancies for 5806 (27.8%) of the women followed during the observation period (see Figure 1). Of these, 7024 pregnancies for 4299 women were completed prior to our registry launch, and 2517 (26.4%) pregnancies for 2146 women were captured from 10 May 2020 onwards. The contribution by country to the registry is displayed in Figure 2.
Consort flow diagram of study inclusion showing the number of pregnancies prospectively recorded, stratified by disease phenotype: radiologically isolated syndrome (RIS), relapse-onset MS (including secondary progressive MS), progressive-onset MS, and neuromyelitis optica spectrum disorder (NMOSD).
Number of pregnancies prospectively recorded by country, or region if fewer than 10 captured. This figure further displays the differences in regional peripartum management, showing the number of disease-modifying therapy (DMT) exposures during pregnancy, categorized by DMT type: none; interferons, glatiramer acetate or dimethyl fumarate (IFN/GA/DMF); monoclonal antibodies (Mabs, including: natalizumab, ocrelizumab, ofatumumab, rituximab, alemtuzumab); and all other therapies.
Of the 2146 women who had pregnancies recorded in the newly launched Registry; 640 women had pregnancies both prior to and after Registry launch, and 1,507 women had pregnancies only after pregnancy registry launch. A total of 1820 (84.8%) women had a single pregnancy, 285 (13.3%) had two pregnancies, and 41 (1.9%) women reported three or more pregnancies during the observation period. The mean maternal age at the last menstrual period (LMP) was 32.3 years (SD 4.7 years), with a median expanded disability status scale (EDSS) score of 1.5 (IQR: 1, 2) within 12 months of the LMP. The median follow-up post-pregnancy was 1.7 years (IQR: 0.8, 2.6 years; range: 0.1–4.2 years). Detailed, per-phenotype, patient characteristics at each pregnancy are summarized in Table 1.
Table 1.: Patient characteristics at each prospectively recorded pregnancy with known outcomes.
We had limited ascertainment of several demographic factors for the 2,146 women with prospectively reported pregnancies. Educational status was available for 684 (31.9%) of women. Of these 57 (8.3%) had completed elementary school, 194 (28.4%) had completed high school, and 433 (63.3%) had completed a tertiary degree. Employment status was available for 660 (30.7%) of women. Of these women, 441 (66.8%) were employed, 45 (6.8%) were unemployed, 83 (12.6%) performed domestic duties, 90 (13.6%) were students, and 1 (0.15%) reported being on a disability support pension. Smoking status was only available for 99 (4.6%) of women, of which 15 (15.1%) were current smokers, 17 (17.2%) were past smokers, and 67 (67.7%) were never smokers. We recorded 592 pregnancies with known outcomes for which assisted reproductive therapy (ART) data were available. Of these, 543 (91.7%) did not use ART; 46 conceived using in vitro fertilization (IVF), two used ovulation drugs and one used other methods.
Pregnancy outcomes
As of 1 August 2024, 1922 (76.4%) of pregnancies were completed, 101 (4%) pregnancies were ongoing. 494 (19.6%) pregnancies did not have outcome data available beyond the date of the last menstrual period and were considered lost to follow-up. Of reported pregnancy outcomes 1464 (76.2%) of pregnancies resulted in full-term births, 180 (9.4%) were preterm births, totaling 1644 (85.5%) live births. 208 (13.7%) of pregnancies resulted in miscarriage, and 55 (2.9%) in termination. Six (0.3%) neonatal deaths and 9 (0.5%) ectopic pregnancies were reported. Of the total 1644 live births reported in our registry, birthweights were available for 413 term babies with a median weight of 3260 g (IQR: 3000, 3590). 918 (55.8%) babies were breastfed of which 150 (16.3%) reported exclusive breastfeeding for a median 3 months (IQR: 1, 5 months; range: 0–6 months). For detailed pregnancy outcomes by disease phenotype, see Table 2. Most pregnancies were singletons, with only 35 twin pregnancies reported. Of the twin pregnancies, 21 were born at term, nine preterm, four miscarriages, and one elective termination were also reported.
Table 2.: Pregnancy and neonatal outcomes by disease phenotype for pregnancies with known outcomes.
The majority of women had unassisted (54.1%) or assisted (7.5%) vaginal births. Elective cesarean sections comprised 29.1% of delivery methods, most often performed in Iran (57.1%), Turkey (50.9%), Italy (46.3%), and Australia (37%). Birth complication data were reported for 614 (31.9%) completed pregnancies. Of these 535 (87.1%) reported no complications. The most common complications were gestational diabetes (n = 16) and pre-eclampsia or pregnancy-induced hypertension (n = 10). Antepartum hemorrhage was reported in five women. Additional complications reported included: growth restriction, large for gestational age, low birth weight, oligohydramnios, polyhydramnios, premature membrane rupture, placenta previa, placental abruption, and others.
Disease-modifying therapy exposures
In the 6 months prior to conception, 506 (25%) pregnancies with known outcomes had no DMT exposure and 1517 (75%) were DMT-exposed, of which 282 (18.6%) discontinued within the 6 months prior to conception with a median 31 days washout (IQR: 2 day, 97 days). Disease-modifying therapy (DMT) exposure in-pregnancy was reported for 1228 (61.8%) pregnancies in women with ROMS, 5 (41.7%) pregnancies in women with POMS, and 4 (19%) NMOSD pregnancies (Table 2). DMT exposure trends varied by country (Figure 2). The interferons, glatiramer acetate, and dimethyl fumarate were most commonly used in pregnancy with 37.8% of pregnancies exposed to these drugs. In-pregnancy monoclonal antibody infusions were recorded in 18.1% of pregnancies.
Of ROMS pregnancies, 1006 (62.3%) of live birth (term and preterm) pregnancies received DMT during pregnancy. The median length of DMT exposure in pregnancy was 42 days (IQR: 25, 218; range: 1–290). Figure 3 summarizes the DMT exposure trends in women with ROMS who had live births from the 6 months prior to conception through to 3 months postpartum. The per-DMT exposure durations for this cohort are summarized in Table 3. Postpartum, 811 (50.2%) ROMS women with live births resumed DMT use within 3 months (Figure 3, Table 3). Whereas, 183 (68%) women reporting miscarriages, terminations and other adverse pregnancy outcomes resumed DMT within 3 months of pregnancy completion.
Frequencies and patterns of disease-modifying therapy (DMT) exposure 6 months preconception, during pregnancy (for any duration) and in the first 3 months postpartum in women with relapse-onset MS. DMTs with fewer than five exposures grouped together in the “other” category.
Table 3.: Disease-modifying therapy use associated with 1615 live births to women with relapse-onset MS.
In the NMOSD cohort, six rituximab exposures were recorded in the 6 months prior to conception. Of these, two ceased therapy prior to conception with a washout of 2 and 4 months, respectively. Four rituximab exposures occurred during pregnancy, median gestation at DMT exposure was 26 days (IQR: 24, 43). Of these six pregnancies, five resulted in healthy, term deliveries, and one in neonatal death. One woman was exposed to eculizumab 2.5 months prior to conception; this pregnancy was aborted. No women with NMOSD restarted DMT within 3 months postpartum; however, five women resumed rituximab a median 271 days (IQR: 219, 287) after the completion of their pregnancies. We did not observe any perinatal exposures to satralizumab.
Of 918 breastfed babies, 296 (32.2%) were DMT-exposed during breastfeeding in the first 3 months postpartum. All breastfeeding mothers who resumed DMT within the first 3 months postpartum had ROMS. The median time to DMT reinitiation during this period was 2 days (IQR: 0, 43; range: 0–91). The DMTs resumed during breastfeeding included glatiramer acetate (n = 78), interferon-beta preparations (n = 62), natalizumab infusions (n = 60), ocrelizumab (n = 20), pegylated-interferon-beta (n = 17), dimethyl fumarate (n = 14), rituximab (n = 12), natalizumab subcutaneous injections (n = 10), ofatumumab (n = 7) and others (n = 16).
Congenital abnormalities
In total, five pregnancies were reported with congenital abnormalities, three preterm pregnancies and two term pregnancies. Of the three preterm pregnancies, one had been exposed to glatiramer acetate for 38 days, another received rituximab at 43 days gestation, the third was not DMT-exposed. No specifics of the congenital abnormalities were reported for this group. One term pregnancy reporting a chromosomal abnormality had been exposed to dimethyl fumarate for 37 days. This mother had a history of prior pregnancies, one of which had also resulted in the birth of a child with congenital abnormalities. The other term pregnancy with congenital abnormality was not DMT-exposed.
Discussion
Family planning and pregnancy decisions are key considerations in the management of women with MS and NMOSD. In the era of highly effective disease-modifying therapies knowledge gaps remain, including best management strategies through pregnancy and whether there are fetal risks associated with DMT exposure in utero.
In this first report from the newly launched prospective MSBase Pregnancy, Neonatal Outcomes and Women’s Health Registry, we report 101 ongoing pregnancies, and pregnancy outcomes for 1922 completed pregnancies, including 21 completed pregnancies for women with NMOSD.
Over 85% of pregnancies with known outcomes resulted in live births, in line with other recently reported studies.^ 22 ^ In our registry, 9% of births were preterm births, 10% of pregnancies were miscarried, reassuringly in line with data from German MS Pregnancy Registry,^ 23 ^ and in line with global rates in the general population as per the World Health Organization.^24,25^
Interestingly, 75% of pregnancies were DMT exposed in the 6 months prior to conception, decreasing to 62% of pregnancies during gestation, an overall lower percentage of DMT use than in the German pregnancy registry that reported 76% exposure at pregnancy.^ 23 ^ Ours may be a slight underestimate as we measured the date of last infusion for monoclonal antibodies, but did not estimate the duration of effect of these drugs. We know, for example that infusional anti-CD20 monoclonal antibodies have a durable effect, protecting against disease activity for many months into pregnancy and potentially beyond.^ 6 ^ The recent study reporting pregnancy outcomes from the Roche pharmacovigilance study for example defined exposure to ocrelizumab if the last infusion was within 3 months of conception.^ 22 ^ Given that here we assessed numerous infusional therapies with varying mechanisms of action, here we determined to use a consistent definition for all. Postpartum, only 50% of our study population with live births had restarted DMT use within the first 3 months of delivery. Most women resumed the use of the same DMT as they had used preconception or during pregnancy, although we did observe a low level of DMT switch. The median exposure to DMT during pregnancy was 42 days. This has increased marginally since our previous 2019 report showing a median exposure of 30 days,^ 26 ^ indicating that many women still discontinue DMT upon pregnancy confirmation. However, we did see a marked increase in the duration of natalizumab exposure, median 202 days (28.9 weeks) in the present study, as compared with 24 days in our previous report.^ 26 ^ This reflects our increased understanding of maternal and fetal outcomes in babies exposed to natalizumab in utero,^ 12 ^ and comfort with using natalizumab through to the end of the second trimester to minimize risk of in-pregnancy disease rebound upon withdrawal.^4,7^
We observed pregnancy management varied among countries. Australian and Kuwaiti clinicians were most likely to manage pregnancies with monoclonal antibodies, whereas Europeans were most likely to use interferons, glatiramer acetate or dimethyl fumarate to manage pregnancy. These differences likely reflect local legislative and therapeutic agency indications for these drugs. While still relatively new, we saw the growing use of ocrelizumab, ofatumumab and subcutaneous natalizumab use perinatally.
While we did not have sufficient weight or other biometric data to analyze neonatal outcomes by DMT exposure, regardless, no overt safety signals were observed. Previous studies have not reported overt differences in outcomes of babies born to mothers with MS, and non-MS controls.^ 27 ^ Furthermore, studies by other groups have not reported concerning safety signals for the newer DMT including natalizumab^12,28^ and ocrelizumab.^ 22 ^
Few studies to-date have reported obstetric outcomes for women with NMOSD.^29?–31^ Here we report 17 (81%) live births and one neonatal death (4.8%) for 21 completed pregnancies in women with NMOSD. Six pregnancies, including the neonatal death, were exposed to rituximab. An analysis of a 153 rituximab-exposed pregnancies reported one neonatal death at 6 weeks.^ 32 ^ In the general population, across Europe, North America, and Australasia, neonatal deaths occur in 2–3 per 1000 live births.^ 33 ^ Here we reported six neonatal deaths across our MS and NMOSD cohorts, marginally higher than the expected five given our cohort size. However, our per-DMT sample size is too small to draw any causal conclusions.
A key strength of our Registry is the unified, prospective, multicenter, international dataset that we have been able to accumulate, with over 2000 pregnancies from women with MS, RIS, and NMOSD recorded over a 4-year period. With time and increasing data collection, we will be able to compare pregnancy and neonatal outcomes across various regions and accumulate real-world evidence for safety signals. Our registry has further worked with the BigMS network to align key data fields, so that we will be able to collaboratively report on safety signals across registries in the future. We will therefore continue to contribute critical evidence for MS management and obstetric care.
We do, however, have several limitations. Our neonatal and pregnancy outcome data are self-reported; therefore, we are unable to confirm outcomes with obstetricians, pediatricians, or other healthcare professionals. Further, details of congenital abnormalities for 4/5 pregnancies were unavailable, and pregnancy complications were underreported. We continue to work with our network to ensure the most accurate acquisition of this important data as we move forward. Another limitation of our registry is that a large number of pregnancies, almost 20%, were lost to follow-up. We have now initiated three-monthly reminders to our network to follow up on known pregnancies, so that we can reduce the number lost to follow-up. Furthermore, the international nature of our database, differing pediatric practice, and legal frameworks means that we are unable to collect neonatal outcomes beyond 12 months of age. To better understand the impacts of DMT exposure in children born to mothers with MS, we will eagerly anticipate results from national registries such as the French RESPONSE study that will be collecting these outcomes out to 6 years.^ 10 ^
Conclusion
This first report from the international MSBase pregnancy registry shows that an increasing number of pregnancies are conceived on monoclonal antibody therapies, confirming increased confidence in their use in the peri-conception period. Reassuringly our data do not show any safety issues at present. However, in an era where pregnancies are increasingly exposed to DMT use and with the growing number of DMT available, it is important to continue to collect data to monitor for fetal and maternal serious adverse events in real-world databases.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Nguyen AL Eastaugh A van der Walt A , et al. Pregnancy and multiple sclerosis: Clinical effects across the lifespan. Autoimmun Rev 2019; 18(10): 102360.31401345 10.1016/j.autrev.2019.102360 · doi ↗ · pubmed ↗
- 2Siriratnam P Huda S Butzkueven H , et al. Risks and outcomes of pregnancy in neuromyelitis optica spectrum disorder: A comprehensive review. Autoimmun Rev 2024; 23(2): 103499.38061621 10.1016/j.autrev.2023.103499 · doi ↗ · pubmed ↗
- 3Krysko KM Graves JS Dobson R , et al. Sex effects across the lifespan in women with multiple sclerosis. Ther Adv Neurol Disord 2020; 13: 1756286420936166.10.1177/1756286420936166 PMC 733177432655689 · doi ↗ · pubmed ↗
- 4Krysko KM Dobson R Alroughani R , et al. Family planning considerations in people with multiple sclerosis. Lancet Neurol 2023; 22(4): 350–366.36931808 10.1016/S 1474-4422(22)00426-4 · doi ↗ · pubmed ↗
- 5Bridge F Butzkueven H van der Walt A , et al. The impact of menopause on multiple sclerosis. Autoimmun Rev 2023; 22(8): 103363.37230311 10.1016/j.autrev.2023.103363 · doi ↗ · pubmed ↗
- 6Yeh WZ van der Walt A Skibina OG , et al. Disease activity in pregnant and postpartum women with multiple sclerosis receiving ocrelizumab or other disease-modifying therapies. Neurol Neuroimmunol Neuroinflamm 2024; 11(6): e 200328.10.1212/NXI.0000000000200328 PMC 1150210639442037 · doi ↗ · pubmed ↗
- 7Yeh WZ Widyastuti PA van der Walt A , et al. Natalizumab, fingolimod and dimethyl fumarate use and pregnancy-related relapse and disability in women with multiple sclerosis. Neurology 2021; 96: e 2989–e 3002.10.1212/WNL.0000000000012084 PMC 825356533879599 · doi ↗ · pubmed ↗
- 8Sadovnick D Criscuoli M Yee I , et al. The Canadian multiple sclerosis pregnancy study: First-trimester miscarriages in women with multiple sclerosis. Mult Scler 2023; 29(3): 407–414.36683353 10.1177/13524585221146270 · doi ↗ · pubmed ↗