Development Process and Evaluation of an Anti-racism Primer and Toolkit for Medical Educators
Meghan T O'Brien, Rachel Fields, Andrea Jackson, Megha Garg

TL;DR
This paper describes the creation and success of an anti-racism toolkit for medical educators to help revise curricula and promote equity.
Contribution
The paper introduces a novel anti-racism primer and toolkit specifically designed for medical educators to address racism in curricula.
Findings
The Anti-Racism Primer was used by 67.6% of content creators to revise curricular materials.
74.1% of users strongly agreed the toolkit helped them reflect on their materials.
Over half of users made revisions to increase inclusivity and eliminate stereotypes.
Abstract
Introduction: Medical educators are expected to address racism and health inequities in their curricula but may feel ill-equipped to do so. Currently, resources to support educators in reviewing and revising curricula through an anti-racism lens are limited. We describe the development process and evaluation of an anti-racism primer and toolkit for medical educators to support curriculum development. Methods: In 2020, three members of the University of California, San Francisco Differences Matter Educational Action Group collaborated to create an iterative, self-directed tool to support educators in creating and revising teaching materials to be anti-racist: the Anti-Racism and Race Literacy: Primer and Toolkit for Medical Educators (Anti-Racism Primer). From August 2020, all medical educators in pre-clinical coursework were recommended to use the Anti-Racism Primer for their…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
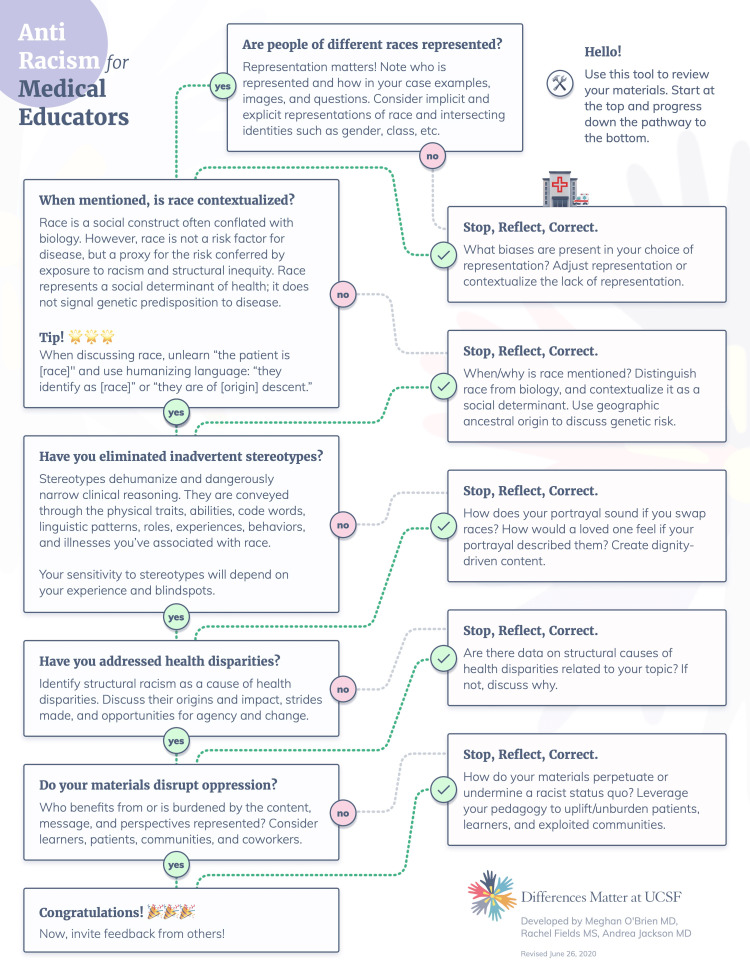 Figure 1
Figure 1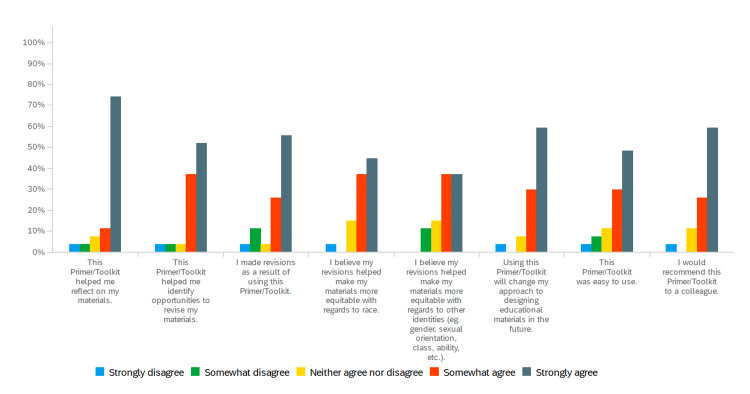 Figure 2
Figure 2| Participant characteristics | N= 82 (%) |
| Gender | |
| Female | 51 (62.2%) |
| Male | 29 (35.4%) |
| Non-Binary | 0 (0.0%) |
| Prefer to self-identify | 0 (0.0%) |
| Preferred not to say | 2 (2.4%) |
| Race | |
| American Indian or Alaska Native | 0 (0.0%) |
| Asian | 15 (18.3%) |
| Black or African American | 5 (6.1%) |
| Hispanic, Latino, or Spanish origin | 8 (9.8%) |
| Native Hawaiian or other Pacific Islander | 3 (3.7%) |
| White | 50 (61.0%) |
| Prefer to self-identify | 4 (4.9%) |
| Prefer not to say | 5(6.1%) |
| LGBTQIA | |
| Yes | 11 (13.4%) |
| No | 66 (80.5%) |
| Prefer not to say | 5 (6.1%) |
| Raised in the United States | |
| Yes | 66 (80.5%) |
| No | 13 (15.9%) |
| Prefer not to say | 3 (3.7%) |
| Years in medical education | |
| <5 | 34 (41.5%) |
| 5-10 | 14 (17.1%) |
| 10-15 | 19 (23.2%) |
| >15 | 15 (18.3%) |
| Theme | Example |
| Language | Used more inclusive language. Removed racial stereotypes. Reconsidered and revised sex- and race-based language. Removed stereotypes and outdated language (e,g, “third world”) |
| Representation | Reviewed and modified vignettes. Included more photos of skin of color. Included multiple gender identities in examples |
| Content | Added different readings focused on equity. Incorporated a focus on anti-racist medicine. Added slides about disparities in care (race, gender, sexual orientation |
| Centering equity | Incorporated statement about educator’s DEI and anti-oppressive goals. Incorporated statement affirming values, incorporation of health equity and access. Created a new curriculum centering on health equity. The course directory asked lecturers to use a primer/toolkit when creating content |
| Uncoupling race/genetics | Looked deeper into the evidence provided to support differences/disparities based on race. Removed language that suggested race has a biological basis. Distinguished risk factors based on genetic ancestry and structural factors from race. More careful references to genetic ancestry and populations. When incorporating data that are published using race as a proxy for genetics, reflected on whether the data is pertinent. Challenges: Distinguishing race from genetics does not reflect how genetics is implemented in practice Difficult to incorporate data from studies that use race as a proxy for genetics |
| Reinforcement | Use the primer as a source to advocate for changes in content that were previously resisted |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGlobal Health Workforce Issues · Cultural Competency in Health Care · Medical Education and Admissions
Introduction
Medical educators and clinicians are often called upon to address race, racism, and health disparities while teaching and delivering care [1,2]. There is increased recognition that medical school curricula can perpetuate false beliefs and implicit biases and lead to misdiagnosis through stereotyping, lack of representation, and racism. This, in turn, can negatively impact clinical care and drive health disparities [3-12]. These factors also affect the integrity and safety of the learning climate and may impact learner success [13]. There is increasing recognition that the physician workforce needs to understand the complex mechanisms, contexts, and manifestations of racism to decrease health disparities and prevent harm to patients and learners [2,14]. However, many educators feel unprepared to address race and racism in curricular materials or the learning environment [15, 16]. As a result, learners may receive an education that inadvertently reinforces biases and inequitable structures in health care.
Recognizing these educational failings, and sparked by the decision not to indict White police officers involved in the murders of unarmed Black men in 2014, medical students around the country organized protests to call attention to how racism is reinforced institutionally and in education. In response to the medical student organization White Coats for Black Lives led a die-in to demand institutional action, the University of California, San Francisco School of Medicine (UCSF) established the Differences Matter Initiative to advance diversity, equity, and inclusion, with a $10 million commitment over five years [17,18]. Through this initiative, a multidisciplinary Education Action Group identified a need to support faculty in revising and creating anti-racist educational materials.
Although neither one’s race nor individual experience of racism necessarily confers comfort or expertise in addressing racism, those with identities historically excluded [19] from medicine are frequently called upon to advance diversity, equity, inclusion, and belonging. This work is under-recognized and often uncompensated, reflecting a disproportionate burden, or “minority tax” [20]. Requests to provide feedback on or revise curricular materials are one manifestation of this tax. To reduce the minority tax and improve the quality of medical education, resources are needed to guide all educators to examine and revise their curricular materials to disrupt inadvertent racism [21].
Working as part of the Differences Matter Educational Action Group, we developed a comprehensive guide entitled the “Anti-Racism and Race Literacy: Primer and Toolkit” (Anti-Racism Primer) to address the gap in peer-reviewed resources for faculty and meet the needs of educators at our institution. Currently, few resources in the peer-reviewed literature exist to support faculty as they develop curricula conscious of bias, stereotypes, structural racism, and health disparities [22]. We identified one checklist for self-assessment to identify and ameliorate areas of bias [23]; however, it assumed the user already had the foundational knowledge needed to understand and implement the necessary revisions.
Because checklists have become an industry standard to achieve higher baseline performance through a standardized approach [24], we included a checklist for educators to guide their self-review, as well as accompanying examples of checklist applications. The checklist helps to identify and revise biased representations, disrupt normative perceptual frames, center health disparities, and interrogate the methodology and objectivity of data to cultivate critical reasoning.
Objectives
We describe the development process and evaluation of an anti-racism primer and toolkit for medical educators to support curriculum development. Specific areas of feedback from educators included whether the Anti-Racism Primer facilitated reflection on and revision and design of curricular materials.
Materials and methods
Anti-racism primer development process
Our toolkit was created for medical school faculty at UCSF, with a student body of approximately 600 medical students. In 2018, the authors (MTO, RF, AJ), working as part of UCSF’s Differences Matter Educational Action Group, developed the Anti-Racism Primer for Medical Educators [25]. The authors were two women faculty medical educators, one Black and one White, and one White woman medical student.
In alignment with Kern’s six-step approach [26] to curriculum development, we identified faculty needs through peer discussions, aggregated student feedback on curricular content, and unpublished internal qualitative research on faculty experience with race and racism in their curriculum and classrooms. Then, we established goals and objectives and developed an educational resource for self-directed application to curricular materials. During the development process, we incorporated iterative feedback from Educational Action Group members, colleagues, and students with expertise in equity and education, and educators who might use the resource. To balance the goals of responsibly handling complex content and producing a tool that was accessible in length, we created multiple points of entry with clear sections that users could access individually as needed.
The Anti-Racism Primer includes an introduction that reviews the reasons for educators to address racism in their materials, the objectives of the primer and toolkit, and instructions for use. It was emphasized that the Anti-Racism Primer provided a starting point for continued self-development.
The Anti-Racism Primer was divided into four steps: 1) Prepare to talk about rRacism and race, which helped navigate the tensions and emotions that surface when discussing these topics; 2) Definitions and frameworks, which provided a mental model of race as a social construct distinct from genetic ancestry; 3) Historical origins of racism in healthcare and medicine, which delved into how the medical system reinforced racism and incorporated racist ideas into its structure; and 4) Implement anti-racism in medical rducation, which provided a checklist guide for developing anti-racist materials and revising materials. Each section was designed to stand alone and included reflection questions and a list of additional resources for deeper engagement.
In July 2020, the Anti-Racism Primer was launched as a living document, updated once per year or as needed by an author (MO) to reflect emerging literature, on the UCSF Differences Matter website [25] as a resource for UCSF health professions educators. Those outside of UCSF could also access and download the document from the publicly accessible website.
At the time of launch, UCSF’s Office of Medical Education asked interdisciplinary course directors and educators involved with the preclinical and clerkship curricula for first- and second-year medical students to review the Anti-Racism Primer and use it to revise their curricular materials.
Anti-racism primer evaluation
After curricular blocks between November 2020 and July 2021, educators who were offered the resource received a survey via email, with a reminder sent two weeks after the initial email, to assess their experience using the Anti-Racism Primer. Following Kern's six-step methodology [26], we evaluated this educational intervention with a survey consisting of multiple-choice questions, Likert scale questions, and open-ended questions about the individual components of the Anti-Racism Primer (Appendix A). We defined “effectiveness” of the Anti-Racism Primer broadly as the majority of users finding benefit from the toolkit in curriculum development across the array of questions asked in our survey. The open-ended questions were intended to give context to multiple-choice question answers and understand specific curricular changes, and were not designed for thematic qualitative analysis.
Results
We received 82 complete survey responses from 1,314 UCSF faculty course directors and health professions educators (response rate 6.2%). Seventy-eight (95.1%) respondents were from the Department of Medicine, with eight (9.8%) from the School of Pharmacy, three (3.7%) from the School of Nursing, four (4.9%) from the School of Dentistry, and one (1.2%) other (participants could select multiple affiliations). Fifty (61.0%) of respondents identified as White, 15 (18.3%) as Asian, five (6.1%) as African American, and three (3.7%) as Native Hawaiian or other Pacific Islander, while nine (11.0%) preferred not to say or to self-identify (participants could select all races that applied). Fifty-one (62.2%) respondents identified as female and 29 (35.4%) as male. Eleven (13.4%) identified as lesbian, gay, bisexual, transgender, queer or questioning, intersex, or asexual or ally (LGBTQIA), while 66 (80.5%) did not, and five (6.1%) preferred not to say. Thirty-four (41.5%) had been involved in health professions education for <5 years. Respondent characteristics are reflected in Table 1.
Overall, 48 (58.5%) of respondents reviewed the Anti-Racism Primer, while 20 (24.4%) did not use it, and 14 (17.1%) reported never receiving it. Forty (48.8%) of the 82 respondents contributed course content, while 42 (51.2%) did not (i.e., facilitators). Of the 40 content contributors, 27 (67.5%) reviewed the toolkit, compared to 21 (50%) of the 42 educators who did not contribute content.
Content creators used the toolkit to revise various curricular materials, including lectures/PowerPoints (22/27, 81.5%), small-group session guides (19/27, 70.4%), clinical vignettes or cases (15/27, 55.6%), exam/practice questions (7/27, 25.9%), and something else (5/27, 18.5%) (respondents could select all that applied). The most used sections of the Anti-Racism Primer were the “one-page flow chart” (22/27, 81.5%) (Figure 1), “Step 2: Definitions and frameworks” (19/27, 70.4%), “Step 3: Understand race in the historical context of healthcare and medicine” (17/27, 63.0%), and “Step 1: Prepare to talk about racism and race” (14/27, 52.9%). Other sections were used less frequently, including “Applying the guide: examples” (11/27, 40.7%), “Introduction” (9/27, 33.3%), and “Additional resources for exploration” (4/27, 14.8%).
One page anti-racism checklist for medical educators
Considering their experience using the Anti-Racism Primer, 20/27 (74.1%) of content creators strongly agreed it helped them reflect on their materials, and 16/27 (59.3%) strongly agreed it would change their approach to designing educational materials in the future and identify opportunities to revise materials. A majority, 15/27 (55.6%), strongly agreed that they made revisions because of using the Anti-Racism Primer. Ten of 27 (37.0%) somewhat agreed and 10/27 (37.0%) strongly agreed that the revisions made their materials more equitable. Thirteen of 27 (48.2%) strongly agreed and 8/27 (29.6%) somewhat agreed that the Anti-Racism Primer was easy to use. Sixteen of 27 (59.3%) strongly agreed and 7/27 (26.9%) somewhat agreed that they would recommend it to a colleague (Figure 2).
Experience using the Anti-Racism and Race Literacy Primer and Toolkit for Medical Educators
Our evaluation survey collected reflective statements from participants regarding the types of changes they made as a result of using the Primer. Respondents who created content described examples of revisions they made because of using the Anti-Racism Primer (Table 2).
These included increased use of inclusive language, eliminating racial stereotypes, diversification of photos, including more expansive gender representation, inclusion of values-affirming statements in syllabi, incorporating health equity topics and evidence, removal of language suggesting race is biological, distinguishing risk factors of genetic ancestry from structural risk factors, and more precise use of genetic ancestry to describe population risk. Others described greater awareness of language used, having an easier time discussing racism with learners, and opening more space in sessions for learner perspectives. Another respondent described that having an institution-endorsed resource empowered their prior advocacy for curricular changes that previously received pushback. Critiques included that the Anti-Racism Primer was too long and bulky. Others noted the difficulty of incorporating discussion points about how race and genetics are distinct when the studies they teach historically conflated the two by using race as a proxy for genetic ancestry.
Those respondents who did not contribute content but reviewed the Anti-Racism Primer to facilitate sessions with students described it as helpful for more specific anti-racism vocabulary, awareness of the magnitude and extent of systemic racism in our society, and language and awareness to bring more nuance to conversations.
Discussion
We developed the Anti-Racism Primer to disseminate a shared mental model and approach to handling the topics of race and racism in educational content. The goal was to offer students a more consistent educational experience that minimized harm and prepared them to respond to health disparities. Anti-Racism Primer users agreed that the resource helped them make revisions that improved perceived equity in their curricular materials. Many described concrete changes they made after engaging the toolkit or feeling better equipped to discuss race with more precision and nuance. At least one respondent noted that its dissemination as an institutionally supported resource reinforced their prior unheeded advocacy for curricular change, suggesting some easing of the minority tax [20]. The importance of institutional support in resource adoption was paramount.
We navigated a tension between responsibly handling complex content and producing a tool accessible in length. To address this, we made multiple entry points with clear sections that users could access individually to suit their needs. Facilitators more commonly used the background information sections, while content creators more commonly used the toolkit checklist components, reflecting the success of this approach. We chose the format of a living document, allowing for responsiveness to both educators’ dynamic needs, new concerns, and evolving understandings of the mechanisms and manifestations of racism. Alternative formats that are shorter, delivered as faculty training workshops, or interactive formats could make the toolkit more accessible. An institutional expectation that the Anti-Racism Primer would be reviewed by educators interacting with students supported its use.
While the toolkit and primer focus on race, we recognize that the depiction and treatment of other identities, including, but not limited to, gender, age, sexuality, ability, education, and economic status, also require thoughtfulness and skill. We choose to center on understanding race and racism because racial inequities are deeply rooted, pervasive, and traverse all indicators of success when other aspects of identity are controlled [27].
The Anti-Racism Primer and our evaluation of its efficacy have limitations. We are a large, publicly funded institution with multiple initiatives devoted to advancing diversity, equity, inclusion, and belonging. This created a climate of receptivity among educators, the lack of which may limit adoption in other settings. Survey respondents continued to struggle with the tension between genetics and race as a proxy for genetics, which we did not discuss as deeply in the Anti-Racism Primer due to length considerations. Our survey assessed educator perceptions of the Anti-Racism Primer and perceived improvement in curricula, which reflect neither the learners’ experience of those materials nor objective curricular material review.
Limitations of the survey include selection bias of respondents (people who used the toolkit were more likely to respond) and a low response rate. The low response rate has several underlying considerations. First, the survey was sent to all educators, whether they facilitated one session or created course content. This range of faculty may have led to many not remembering the Anti-Racism Primer or choosing to respond to the survey request. There was also a lag of months from when some faculty used the primer to when they received the related survey. However, we felt it was important to send the survey out widely and not bias the responses by targeting specific educators. Finally, keeping the Anti-Racism Primer up to date with evolving knowledge and terminology is challenging. Further resources are required to support ongoing revisions.
The Anti-Racism Primer addressed a knowledge gap within our institution where few external resources existed at the time. The checklist from the Anti-Racism Primer has been adapted to a faculty development workshop focused on equitable approaches to curriculum development. It has also been adapted, in conjunction with materials from UCSF’s Anti-Oppressive Curriculum Initiative, into a content review checklist that Office of Medical Education staff use to support workshop creators in revising their content to be anti-oppressive. This Anti-Racism Primer contributes to a growing number of resources for developing anti-racist curricula [28-30]. Future directions for these resources include focused support tools for specific, more challenging, and controversial content areas (i.e., genetics) in partnership with content experts. In particular, regarding such toolkits, more robust studies including comparison or control groups and direct review of curricular materials rather than educator perceptions would help with understanding the direct impact of such resources on curricula.
Conclusions
The Anti-Racism Primer is an effective resource to support health professions educators in their understanding and incorporating anti-racism in the creation and revision of curricular materials. Users engaged with different sections depending on their needs, and most described that using the Anti-Racism Primer supported reflection and would influence their approach to future content development. Dissemination as an institutionally supported resource supports utilization and can amplify pre-existing efforts toward equitable change. Future steps include studies about the impact of such resources on learners and further qualitative evaluation of faculty development needs in anti-racism education.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Association of a health equity curriculum with medical students’ knowledge of social determinants of health and confidence in working with underserved populations JAMA Netw Open Denizard-Thompson N Palakshappa D Vallevand A 04202110.1001/jamanetworkopen.2021.0297 PMC 792190133646312 · doi ↗ · pubmed ↗
- 2Medical schools overhaul curricula to fight inequities 9 2023 2021 https://www.aamc.org/news/medical-schools-overhaul-curricula-fight-inequities
- 3Misrepresenting race - the role of medical schools in propagating physician bias N Engl J Med Amutah C Greenidge K Mante A 87287838420213340632610.1056/NEJ Mms 2025768 · doi ↗ · pubmed ↗
- 4Under-representation of skin of colour in dermatology images: not just an educational issue Br J Dermatol Lester JC Taylor SC Chren MM 1521152218020193115742910.1111/bjd.17608 · doi ↗ · pubmed ↗
- 5Towards the Abolition of Biological Race in Medicine: Transforming Clinical Education, Research, and Practice Chadha N Lim B Kane M Rowland B Berkeley, CAUC Berkeley: Othering & Belonging Institute.2020 https://escholarship.org/uc/item/4gt 3n 0dd
- 6Race/ethnicity in medical education: an analysis of a question bank for Step 1 of the United States Medical Licensing Examination Teach Learn Med Ripp K Braun L 1151222920172805188910.1080/10401334.2016.1268056 · doi ↗ · pubmed ↗
- 7Racial bias in pain assessment and treatment recommendations, and false beliefs about biological differences between blacks and whites Proc Natl Acad Sci U S A Hoffman KM Trawalter S Axt JR Oliver MN 4296430111320162704406910.1073/pnas.1516047113 PMC 4843483 · doi ↗ · pubmed ↗
- 8The effects of racism in medical education on students’ decisions to practice in underserved or minority communities Acad Med Phelan SM Burke SE Cunningham BA 117811899420193092044310.1097/ACM.0000000000002719 · doi ↗ · pubmed ↗