A Rectal Mass That Deceived: Solitary Plasmacytoma Masquerading as Mantle Cell Lymphoma With Subsequent Progression to Multiple Myeloma
Milaris M Sanchez-Cordero, Josean Rosado Rivera, Leanette Guzman, Santa Merle

TL;DR
A rare case shows how a rectal tumor was initially misdiagnosed as lymphoma but later revealed to be a plasmacytoma that progressed to multiple myeloma.
Contribution
Highlights diagnostic challenges and progression from solitary plasmacytoma to multiple myeloma in a rectal mass.
Findings
Initial biopsy misdiagnosed rectal mass as mantle cell lymphoma.
Surgical excision confirmed solitary extramedullary plasmacytoma.
Patient later developed multiple myeloma from the plasmacytoma.
Abstract
Solitary extramedullary plasmacytomas (SEPs) are rare plasma cell tumors, particularly when located in the gastrointestinal tract. Misdiagnosis may occur due to overlapping histological and immunophenotypic features with other hematologic malignancies, such as mantle cell lymphoma (MCL). We present the case of a 63-year-old female patient initially diagnosed with MCL based on rectal mass biopsy, who underwent lymphoma-directed therapy. Surgical excision and further histopathological evaluation revised the diagnosis to SEP. Over time, the patient developed serum monoclonal gammopathy and progressed to multiple myeloma (MM). This case highlights the diagnostic pitfalls of rectal lymphoid lesions, the value of surgical pathology, and the potential for SEPs to evolve into systemic plasma cell neoplasia.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1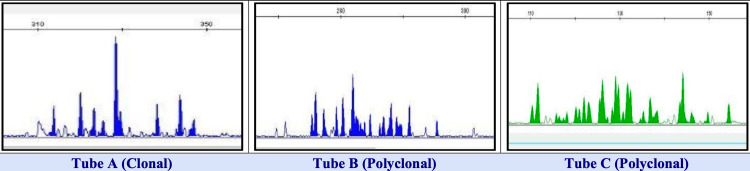 Figure 2
Figure 2 Figure 3
Figure 3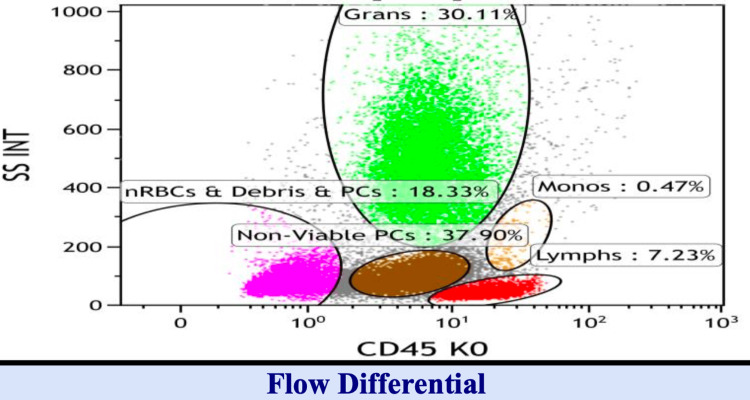 Figure 4
Figure 4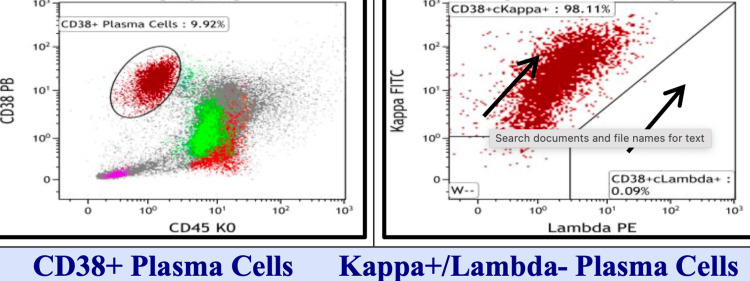 Figure 5
Figure 5 Figure 6
Figure 6 Figure 7
Figure 7| Antibody | Specificity | Result |
| BCL6 | Follicular center | Negative |
| BLC2 | Mature T-lymphocytes and Various B-cell lymphomas | Positive |
| CD20 | Pan B-lymphocytes | Positive |
| CD10 | B-lymphoblasts, follicular center cells & grans | Negative |
| BCL1 | Mantle cell lymphoma | Positive |
| CD5 | Pan T-lymphocytes | Negative |
| CD23 | Follicular dendritic cells (FDC) | Negative |
| CD21 | Follicular dendritic cells | Negative |
| CD30 (Ki-1) | Immunoblasts and Hodgkin Reed-Sternberg cells | Negative |
| CD3 | Mature T-lymphocytes | Negative |
| Ki-67 | Proliferative Index | Low (10-20%) |
| c-MYC | DLBCL subsets | Negative |
| Locus | Probe | Result | Cell counted |
| 11q13.3/14q32.33 | CCND1/IGH | Abnormal/IGH/CCND1 variant translocation (88%) | 100 |
| Cell type | Result (%) | Reference range (%) |
| Pronormoblast | 0.0 | 0-1.0 |
| Basophilic normoblast | 0.0 | 0-5.0 |
| Polychromatic normoblast | 0.0 | 6.0-16.0 |
| Orthochromatic normoblast | 2.5 | 4.0-18.0 |
| Lymphocyte | 6.5 | 3.0-20.0 |
| Plasma cell | 60.0 | 1.0-4.0 |
| Promonocyte | 0.0 | 0-2.0 |
| Monocyte | 0.0 | 1.0-4.0 |
| Myeloblast | 1.0 | 0-1.0 |
| Promyelocyte | 0.0 | 2.0-4.0 |
| Myelocyte | ||
| Granulocyte | 2.5 | 5.0-19.0 |
| Eosinophil | 0.0 | 0.5-3.0 |
| Basophil | 0.0 | 0-1.0 |
| Metamyelocyte | 4.5 | 12.0-22.0 |
| Band | 10.5 | 8.0-16.0 |
| Segmented | ||
| Granulocyte | 12.5 | 7.0-22.0 |
| Eosinophil | 0.0 | 0.5-4.0 |
| Basophil | 0.0 | 0-1.0 |
| Megakaryocytes: not adequately represented | ||
| Iron stain: cannot be assessed (aspicular with no ring sideroblasts) | ||
| Analysis | Gatting strategy | CD45 and side scatter | |
| Specimen | Bone marrow | Viability | 51% (Normal >80%) |
| Gated population | Lymphs | Plasma cells | Large B-lymphs |
| Gated cells | 7% | 10% | 1% |
| B-cell markers | |||
| CD19 | 54% | ||
| CD20 | 53% | ||
| CD10 | 5% | ||
| CD23 | 6% | ||
| CD19/CD5 | <1% | ||
| CD19/CD38 | 8% | ||
| CD38 | 4% | ||
| CD79b | 40% | ||
| CD103 | 1 | ||
| CD19/CD123 | <1% | ||
| BCL2 | <1% | ||
| CD19/Kappa | 67% | 65% | |
| CD19/Lambda | 33% | 25% | |
| CD43 | <1% | ||
| CD200 | 41% | ||
| T-cell markers | |||
| CD3 | 48% | ||
| CD4 | 20% | ||
| CD8 | 26% | ||
| CD2 | 54% | ||
| CD5 | 47% | ||
| CD7 | 57% | ||
| NK cell markers | |||
| CD56 | 9% | ||
| CD16 | 2% | ||
| CD57 | 8% | ||
| Plasma cell markers | |||
| CD38/CD138 | 99% | ||
| CD38/CD56 | <1% | ||
| CD38/CD19 | <1% | ||
| CD38/CD27 | <1% | ||
| CD38/CD117 | <1% | ||
| CD38/CD20 | 3% | ||
| CD38/Kappa | 98% | ||
| CD38/Lambda | <1% | ||
| CD38/IgA | <1% | ||
| CD38/IgG | 5% | ||
| CD38/IgM | <1% | ||
| Locus | Probe | Result | Result | Cell counted |
| 1p36.31/1q25.3 | 1p36/1q25. | ZytoVision #Z-2075-200 | Normal | 200 |
| 9q12 | CEN9 | ZytoVision #Z-2067-200 | Normal | 200 |
| 11q13.3/14q32.33 | CCND1/IGH | ZytoVision #Z-2125-200 | Abnormal/IGH/CCND1 variant translocation (82%) | 200 |
| 13q142/13q34 | D13S319/13q34 (G) | ZytoVision #Z-2280--50 | Abnormal/monosomy 13 (87%) | 200 |
| 17p13.1/13p11.1-q11.1 | TP53/CEN17 | ZytoVision #Z-2153-200 | Normal | 200 |
| Date | Finding | Interpretation |
| May 29, 2020 | Biopsy: Cyclin D1+, CD20+, BCL1+ MCL in sigmoid colon, IGH/CCND1 by FISH | Diagnosis: mantle cell lymphoma (MCL) |
| 2021-2022 | Serial colon biopsies with persistent infiltration, evolving morphology | Reclassified as CD20+ plasmacytoid neoplasm |
| Oct 13, 2022 | Bone marrow: 90% cellularity, CD138+, BCL1+, Kappa restriction | Plasma cell neoplasm confirmed via flow cytometry (CD19-/CD27-) |
| Apr-Nov 2023 | Free Kappa ↑ from 248.19 → 2107.20 mg/L; Kappa/Lambda ratio ↑ to 114.9; Bence Jones proteinuria | Confirms light-chain multiple myeloma secretory phenotype |
| Sep 6, 2024 | Retromandibular mass: CD138+, Cyclin D1+, Kappa+, Lambda-, CD19/20/45- | Extramedullary plasmacytoma with clonal evolution |
| Date | Test | Result | Interpretation |
| Apr 20, 2021 | Immunofixation (urine) | Two monoclonal Kappa light chains | Suggestive of plasma cell disorder (e.g., light-chain MM or AL amyloidosis) |
| Apr 23, 2023 | Free light chains (serum) | Kappa 248.19 mg/L, K/L ratio = 25.1 | Strongly suggestive of monoclonal proliferation |
| Nov 2023 | Free light chains (serum) | Kappa 2107.20 mg/L, K/L ratio = 114.9 | Aggressive clonal plasma cell proliferation |
| Nov 2023 | Immunofixation (urine) | Positive; proteinuria 59.5 mg/dL | Bence Jones confirmed |
| Nov 29, 2023 | SPEP | M-spike 2.67%, Gamma 0.15 g/dL | Early persistent monoclonal gammopathy |
| Phase | Key markers | Interpretation |
| Initial (2020) | Cyclin D1+, CD20+, t(11;14) | Mantle cell lymphoma |
| Transition (2021-2022) | Persistent CD20+, evolving morphology | Suspicion of plasmacytic differentiation |
| Progression (2022) | CD138+, Kappa+, CD19- | Monoclonal plasma cell neoplasm |
| Light-chain MM (2023-2024) | ↑ Free Kappa, ↑ K/L ratio, Bence Jones, ↓ gamma fraction | Confirmed light-chain secretory multiple myeloma |
| Extramedullary involvement | CD138+, Cyclin D1+, Kappa+, Lambda-, CD19/20/45- (retromass) | Clonal progression to extramedullary plasmacytoma |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMultiple Myeloma Research and Treatments · Lymphoma Diagnosis and Treatment · Chronic Lymphocytic Leukemia Research
Introduction
Solitary extramedullary plasmacytoma (SEP) is a rare variant of plasma cell dyscrasia that presents as a localized clonal plasma cell proliferation outside of the bone marrow. SEPs account for less than 5% of all plasma cell neoplasms, and gastrointestinal (GI) involvement is even more uncommon, representing fewer than 10% of all cases [1,2]. When SEPs occur in the GI tract, the stomach, small intestine, and colon are more frequently affected than the rectum [3]. Rectal plasmacytomas are exceedingly rare, with few documented cases in the literature [4].
Differentiating SEP from lymphomas such as mantle cell lymphoma (MCL) is diagnostically challenging due to overlapping histological and immunophenotypic features. MCL is a B-cell non-Hodgkin lymphoma characterized by Cyclin D1 overexpression as a result of the t(11;14)(q13;q32) translocation [5]. Cyclin D1 expression is a hallmark of MCL; however, it can occasionally be observed in plasma cell neoplasms, including plasma cell myeloma and SEP, contributing to diagnostic confusion [6].
The initial misdiagnosis of SEP as MCL may lead to inappropriate therapy and a delay in initiating plasma cell-targeted treatment. This case underscores the importance of comprehensive immunohistochemical panels and, when needed, full-thickness surgical specimens for accurate diagnosis. Additionally, it highlights the clinical relevance of disease progression from SEP to systemic involvement as multiple myeloma (MM), a transformation observed in 50-70% of SEP cases over time [7,8].
Case presentation
A 63-year-old female patient presented with rectal pain, tenesmus, and altered bowel habits. Colonoscopy identified a rectal mass, and initial biopsy showed atypical lymphoid infiltrates. Immunohistochemistry revealed positivity for Cyclin D1, CD5, CD20, and a high Ki-67 index, leading to a preliminary diagnosis of MCL. The patient was started on chemotherapy accordingly.
Due to an incomplete clinical response and persistent symptoms, surgical excision of the mass was performed. Final histopathology of the excised specimen demonstrated a dense monoclonal plasma cell infiltrate. Immunostaining was positive for CD138 and CD56 and showed Kappa light chain restriction. Markers including CD20 (+), CD5 (-), and Cyclin D1 (-) (Figure 1). These findings were diagnostic of SEP (Table 1).
Colon and rectosigmoid segmentsHistologic sections of colonic mucosa show diffuse infiltration by small to intermediate-sized neoplastic lymphoid cells. Immunohistochemical staining demonstrates that the infiltrate is positive for CD20, BCL1 (Cyclin D1), and BCL2
Subsequent workup included serum protein electrophoresis (SPEP), which showed an M-spike, and a serum free light chain assay that demonstrated a significantly abnormal Kappa/Lambda ratio. Initial bone marrow biopsy was negative for plasma cell infiltration (Table 2, Figure 2).
Molecular diagnosis (IGH)IGH: immunoglobulin heavy chainColon-rectosigmoid segments: (+) for clonal B-cell IGH gene rearrangement.
However, six months later, a repeat bone marrow biopsy revealed clonal plasma cells to be ≥10%. Positron emission tomography/computed tomography (PET/CT) imaging did not identify other lesions. The patient was diagnosed with evolving MM and treated with bortezomib, lenalidomide, and dexamethasone (Figure 3, Table 3).
Bone marrow biopsy and aspirate findingsBCL: B-cell lymphomaBone marrow biopsy reveals a markedly hypercellular marrow with diffuse infiltration by plasma cells, comprising approximately 90% of the cellular population. Immunohistochemical staining shows strong CD138 positivity, partial CD20 expression, and BCL1 (Cyclin D1) positivity, consistent with a clonal IgG/kappa-restricted plasma cell neoplasmThe aspirate is aspicular and moderately hemodiluted, demonstrating 60% markedly atypical plasma cells.
Additional evaluations from April to November 2023 showed progressive increases in serum free Kappa chains (from 248.19 to 2107.20 mg/L), a Kappa/Lambda ratio rising to 114.9, and positive Bence Jones proteinuria. By September 6, 2024, the patient developed a retromandibular mass. Biopsy confirmed extramedullary plasmacytoma with CD138+, Cyclin D1+, MUM1+, and Kappa-restricted cells (Tables 4-5, Figures 4-6).
Flow cytometry 1A
Flow cytometry 1B
Flow cytometry 1C
Fluorescence in situ hybridization (FISH) results: bone marrow aspirateFISH analysis performed on conventional bone marrow preparation reveals a positive IGH/CCND1 (t[11;14]) translocation and monosomy 13. In the context of multiple myeloma, the presence of IGH/CCND1 is associated with standard-risk disease based on the International Cytogenetic Risk Stratification System. Monosomy 13 is of uncertain prognostic significance
These were negative for CD19, CD20, CD45, and Lambda, supporting clonal progression from MCL to plasma cell neoplasm (Tables 6-8).
Despite multiple lines of therapy including bortezomib, daratumumab, cyclophosphamide, Kyprolis, and pomalidomide, the disease progressed biochemically and extramedullary, with persistent Kappa chain secretion and need for morphine-based analgesia.
Discussion
This case illustrates the diagnostic complexity associated with rectal lymphoid or plasma cell neoplasms. GI plasmacytomas are rare and often misclassified due to their overlapping morphology and immunophenotype with lymphomas, especially MCL [3,4,6]. Cyclin D1 positivity, although characteristic of MCL, may be expressed in plasma cell neoplasms, contributing to diagnostic error [5,6].
Accurate distinction between SEP and MCL is essential, given the vastly different therapeutic approaches. In our case, the patient initially received lymphoma-directed therapy before surgical resection, and expanded immunophenotyping clarified the true diagnosis. Misclassification can lead to suboptimal treatment and delays in appropriate systemic therapy for plasma cell neoplasms.
According to the International Myeloma Working Group (IMWG), diagnosis of MM requires ≥10% clonal plasma cells in bone marrow or biopsy-proven plasmacytoma with CRAB features (hypercalcemia, renal dysfunction, anemia, bone lesions) or specific biomarkers such as high serum free light chain ratios (>100) [9,10]. Our patient met multiple criteria: increasing free Kappa chains, high Kappa/Lambda ratio, Bence Jones proteinuria, and ultimately, clonal bone marrow plasma cells and extramedullary progression. These changes document a clear trajectory from SEP to MM.
Studies have shown that SEP has a five-year progression risk to MM ranging from 30% to 70% depending on site, size, and baseline laboratory values [7,8]. GI tract SEPs, although rare, should be closely monitored with serum free light chains, SPEP, and periodic bone marrow evaluation.
In addition to Cyclin D1, the use of markers such as CD138, CD38, and light chain restriction by immunohistochemistry and flow cytometry is critical in characterizing plasma cell disorders [6]. In ambiguous cases, fluorescence in situ hybridization (FISH) and molecular studies can further delineate lymphoid from plasma cell malignancies.
Conclusions
This case is notable for the clinical rarity of a solitary plasmacytoma located in the rectum, an uncommon site for extramedullary plasma cell neoplasms. The definitive diagnosis was initially delayed because the patient declined a bone marrow biopsy, leading to the continuation of lymphoma-directed therapy under the presumption of MCL. However, due to a lack of response and persistent disease, surgical resection and full immunophenotypic workup were pursued, ultimately revealing solitary plasmacytoma. This case underscores the importance of comprehensive diagnostic evaluation in Cyclin D1-positive rectal masses, particularly when there is an atypical response to standard lymphoma regimens. In such scenarios, clinicians must maintain a high index of suspicion for plasma cell dyscrasias, even in unusual anatomical sites.
Accurate immunophenotyping, molecular testing (including FISH), and surgical pathology are essential tools that can prevent misdiagnosis and facilitate timely, targeted treatment. Furthermore, this case highlights the potential for SEPs to evolve into systemic MM, justifying the need for long-term surveillance with serial imaging, free light chain monitoring, and bone marrow reassessment. This case contributes to the limited but growing literature on rectal plasmacytomas and reinforces the importance of integrating pathology, molecular genetics, and clinical acumen in the management of rare plasma cell neoplasms.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Guidelines on the diagnosis and management of solitary plasmacytoma of bone and solitary extramedullary plasmacytoma Br J Haematol Soutar R Lucraft H Jackson G Reece A Bird J Low E Samson D 71772612420041500905910.1111/j.1365-2141.2004.04834.x · doi ↗ · pubmed ↗
- 2Extramedullary plasmacytoma: tumor occurrence and therapeutic concepts Cancer Alexiou C Kau RJ Dietzfelbinger H Kremer M SpießJC Schratzenstaller B Arnold W 2305231485199910357398 · pubmed ↗
- 3Extramedullary plasmacytoma of the colon: a case report Ulus Cerrahi Derg Zihniİ DinçR Canpolat S Cengiz F Uslu A 2312333020142593192310.5152/UCD.2013.45PMC 4379798 · doi ↗ · pubmed ↗
- 4Solitary extramedullary plasmacytoma in the lung misdiagnosed as lung cancer: a case report and literature review Front Oncol Wang J Yang X Liu X 12202210.3389/fonc.2022.950383 PMC 946877236110956 · doi ↗ · pubmed ↗
- 5Cyclin D 1 expression in multiple myeloma by immunohistochemistry: case series of 14 patients and literature review Indian J Med Paediatr Oncol Padhi S Varghese RG Ramdas A 2832913420132460495910.4103/0971-5851.125246 PMC 3932597 · doi ↗ · pubmed ↗
- 6A practical approach to diagnosis of B-cell lymphomas with diffuse large cell morphology Arch Pathol Lab Med King JF Lam JT 16016714420203199022810.5858/arpa.2019-0182-RA · doi ↗ · pubmed ↗
- 7Plasmacytoma in patients with multiple myeloma: morphology and immunohistochemistry BMC Cancer Firsova MV Mendeleeva LP Kovrigina AM Solovev MV Savchenko VG 3462020203232146510.1186/s 12885-020-06870-w PMC 7178964 · doi ↗ · pubmed ↗
- 8Solitary bone plasmacytoma and extramedullary plasmacytoma Curr Treat Options Oncol Dimopoulos MA Hamilos G 255259320021205707110.1007/s 11864-002-0015-2 · doi ↗ · pubmed ↗