Comparing the effects of transthoracic echocardiography and transesophageal echocardiography on stress injury, pain mediators in patients with severe aortic stenosis
Aidong Chen, Bin Chen, Po Yang, Xiaoming Shi, Zhipeng Xu, Fanxin Deng

TL;DR
This study compares TTE and TEE in patients with severe aortic stenosis, finding that TEE improves TAVR outcomes with better hemodynamics and reduced stress and pain mediators.
Contribution
The study provides novel empirical evidence on the comparative benefits of TEE over TTE in reducing stress and pain mediators during TAVR procedures.
Findings
TEE group showed superior postoperative hemodynamics compared to TTE group.
TEE group had lower levels of stress and pain mediators like IL-1b, IL-6, TNF-a, 5-HT, ET-1, and SP.
TEE and TTE were equally effective in evaluating aortic root via echocardiography and MSCT.
Abstract
We compared the differences in the effects of transthoracic echocardiography (TTE) and transesophageal echocardiography (TEE) on hemodynamics, inflammatory stress response, and pain mediators in patients with severe aortic stenosis (AS). 204 patients with severe AS treated with transcatheter aortic valve replacement (TAVR) in our hospital were selected as the research subjects from January 2022 to February 2024. Among them, 109 patients received TTE (TTE group), and another 95 received TEE (TEE group). Differences in the evaluation effects of preoperative echocardiography and multi-slice helical computed tomography (MSCT) in all patients were compared, and changes in echocardiographic parameters before and after surgery were observed. In addition, the differences in postoperative hemodynamics, cardiac function [brain natriuretic peptide (BNP), cardiac troponin I (cTnI), creatine kinase…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
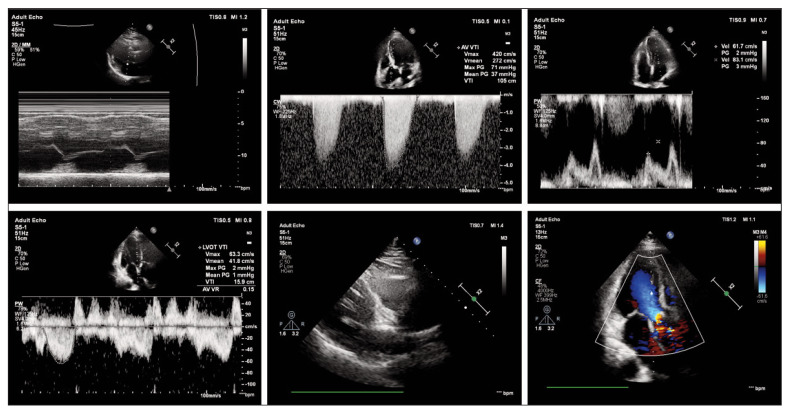 Figure 1
Figure 1| n=204 | Maximum diameter<br>(mm) | Minimum Diameter<br>(mm) | Area (mm2) | Circumference<br>(mm) | AVA<br>(cm2) |
|---|---|---|---|---|---|
| MSCT | 27.32±3.33 | 22.19±3.56 | 485.83±169.93 | 78.31±11.68 | 0.69±0.16 |
| Echocardiography | 27.78±4.07 | 22.55±3.08 | 474.06±141.20 | 79.12±10.66 | 0.67±0.15 |
| t | 1.252 | 1.116 | 0.760 | 0.731 | 0.901 |
|
| 0.211 | 0.265 | 0.448 | 0.465 | 0.368 |
| n=204 | Before surgery | After surgery | t |
|
|---|---|---|---|---|
| AVPGmax (m/s) | 4.82±0.76 | 2.34±0.76 | 33.120 | <0.001 |
| AVPGmean (mmHg) | 53.99±15.79 | 11.96±7.11 | 34.660 | <0.001 |
| Vmax (m/s) | 4.99±0.75 | 2.28±0.47 | 43.840 | <0.001 |
| LAD (mm) | 43.95±6.59 | 42.81±8.12 | 1.691 | 0.092 |
| LVEDD (mm) | 49.67±7.29 | 48.50±6.76 | 0.373 | 0.710 |
| LVESD (mm) | 35.08±8.91 | 29.39±6.92 | 7.213 | <0.001 |
| IVST (mm) | 13.74±2.00 | 12.25±1.30 | 8.905 | <0.001 |
| PWT (mm) | 12.86±1.34 | 11.35±1.31 | 11.480 | <0.001 |
| PASP (mmHg) | 49.14±5.74 | 38.95±8.44 | 8.156 | <0.001 |
| LVEF (%) | 57.37±12.44 | 37.83±6.02 | 20.190 | <0.001 |
| AVA (cm2) | 0.67±0.15 | 1.81±0.24 | 58.910 | <0.001 |
| TTE group (n=109) | TEE group (n=95) | t (or χ2) |
| |
|---|---|---|---|---|
| Age | 72.54±5.66 | 72.16±4.42 | 0.534 | 0.594 |
| Sex | 0.130 | 0.718 | ||
| male | 65 (59.63) | 59 (62.11) | ||
| female | 44 (40.37) | 36 (37.89) | ||
| Course of disease (years) | 4.72±1.23 | 4.48±1.11 | 1.457 | 0.147 |
| NYHA cardiac function grade | 0.431 | 0.512 | ||
| IV | 19 (17.43) | 20 (21.05) | ||
| III | 90 (82.57) | 75 (78.95) | ||
| Combined hypertension | 0.113 | 0.737 | ||
| yes | 71 (65.14) | 64 (67.37) | ||
| no | 38 (34.86) | 31 (32.63) | ||
| Combined diabetes mellitus | 0.543 | 0.370 | ||
| yes | 62 (56.88) | 50 (52.63) | ||
| no | 47 (43.12) | 45 (47.37) | ||
| Smoking | 1.317 | 0.251 | ||
| yes | 33 (30.28) | 36 (37.89) | ||
| no | 76 (69.72) | 59 (62.11) | ||
| Drinking | 0.529 | 0.396 | ||
| yes | 27 (24.77) | 20 (21.05) | ||
| no | 82 (75.23) | 75 (78.95) |
| Groups | SVRI (dyn·s·cm5/m2) | GEDVI (mL/m2) | EVLWI (mL/kg) | ITBVI (mL/m2) |
|---|---|---|---|---|
| TTE (n=109) | 1657.22±541.66 | 633.50±174.78 | 15.92±6.13 | 963.14±207.77 |
| TEE (n=95) | 2200.38±586.30 | 838.43±179.51 | 11.65±4.86 | 1052.81±191.67 |
| t | 6.875 | 8.249 | 5.450 | 3.187 |
|
| <0.001 | <0.001 | <0.001 | 0.002 |
| Groups | BNP (pg/mL) | cTnI (ng/mL) | CK-MB (U/L) |
|---|---|---|---|
| TTE (n=109) | 151.67±37.28 | 1.01±0.24 | 52.54±13.98 |
| TEE (n=95) | 156.77±39.85 | 1.08±0.36 | 50.79±12.05 |
| t | 0.944 | 1.617 | 0.951 |
|
| 0.346 | 0.107 | 0.343 |
| Groups | SOD (U/L) | MDA (mmol/L) | IL-1β (pg/mL) | IL-6 (pg/mL) | TNF-α (pg/mL) |
|---|---|---|---|---|---|
| TTE (n=109) | 6.98±2.65 | 171.32±28.71 | 25.63±4.95 | 18.99±4.26 | 23.18±4.61 |
| TEE (n=95) | 7.83±3.14 | 173.72±24.76 | 21.51±5.52 | 15.28±3.05 | 19.17±2.02 |
| t | 2.075 | 0.636 | 5.618 | 7.055 | 7.841 |
|
| 0.039 | 0.525 | <0.001 | <0.001 | <0.001 |
| Groups | 5-HT (ng/L) | ET-1 (ng/L) | PGE2 (ng/L) | SP (ng/L) |
|---|---|---|---|---|
| TTE (n=109) | 54.71±8.84 | 0.55±0.10 | 80.85±0.87 | 5.01±1.02 |
| TEE (n=95) | 51.77±7.93 | 0.52±0.11 | 79.67±9.79 | 4.51±1.24 |
| t | 2.485 | 2.450 | 0.912 | 3.159 |
|
| 0.014 | 0.015 | 0.363 | 0.002 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac Valve Diseases and Treatments · Cardiovascular Function and Risk Factors · Cardiac, Anesthesia and Surgical Outcomes
Introduction
Aortic stenosis (AS) is the most frequent valvular heart disease among older individuals [1]. AS can present as dyspnoea, angina, syncope and palpitations [2]. Statistics show that about 12 per cent of people aged 75 have AS [3].
Surgical aortic valve replacement (SAVR) is the primary clinical treatment for severe AS, which replaces the original diseased or abnormal heart valves with artificial valves to restore normal cardiac function [4]. However, there are still some severe AS patients who cannot tolerate SAVR with significant trauma due to various reasons such as advanced age, left ventricular dysfunction, pulmonary insufficiency, or comorbidities [5]. With the development of medical technology, transcatheter aortic valve replacement (TAVR) has gradually become the preferred treatment for severe AS due to its advantages of short operation time, less trauma, and quick recovery [6] [7]. In TAVR, echocardiography is one of the essential means for preoperative screening, intraoperative monitoring, and postoperative follow-up, which can quickly evaluate the significance of essential indexes such as left ventricular function [8]. Currently, the commonly used clinical ultrasound protocols in intermediate TAVR are transthoracic echocardiography (TTE) and transesophageal echocardiography (TEE), both of which can accurately reflect the patient’s cardiac status and help the clinic perform TAVR better. However, we found that all the related studies focused on TAVR, often ignoring the importance of imaging technology, with little research discussing the application differences of TTE and TEE in TAVR. Therefore, the use of both protocols remains highly controversial. For example, Rozenbaum Z et al. [9] concluded that TTE provides a more accurate indication of vascular resistance in the patient’s lungs and is more conducive to controlling blood loss during surgery. In contrast, Bax JJ et al. [10] stated that TEE is more accurate in assessing cardiac function in complex clinical situations.
To address these limitations, this study will analyse the use of echocardiography in TAVR to identify which ultrasound protocol is more suitable. Thus, it will further improve the surgical safety and prognosis of TAVR for severe AS.
Materials and methods
Research participants
Two hundred and four patients with severe AS admitted to our hospital from January 2022 to February 2024 were selected as the research participants. Age 58–85 years, mean (72.26±5.11) years; disease duration 2–8 years, mean (4.61±1.18) years; 124 males, 80 females; New York Heart Association (NYHA) [11] grade III 165 cases, grade IV 39 cases. All of them completed TAVR in our hospital, of which 109 underwent transthoracic echocardiography (TTE) as the TTE group, and 95 underwent transesophageal echocardiography (TEE) as the TEE group. This study was approved by the Ethics Committee of our hospital (No. 2021-SR-020) and strictly followed the Declaration of Helsinki. All study subjects signed an informed consent form.
Inclusion and exclusion criteria
Inclusion criteria: (1) age>18 years old, with complete medical records; (2) severe AS [maximum aortic valve orifice blood flow velocity (V_max_) 4.0 m/s, mean aortic valve pressure gradient (AVPG_mean_)40 mmHg, or aortic valve area (AVA)<1.0 cm^2^; NYHA cardiac functional classification >grade II] diagnosed by our hospital. (3) meeting the indications for TAVR surgery and completing surgical treatment in our hospital. Exclusion criteria: (1) inability to undergo echocardiography (including elderly patients who are unable to hold their breath to acquire three-dimensional images); (2) allergies or contraindications to anticoagulant/antiplatelet therapy; (3) cerebrovascular accident or transient ischemic attack within 2 months before surgery; (4) severe liver, lung, and kidney diseases and contrast agent allergies; (5) estimated survival after correction of AS<12 months.
Surgical procedure
Before surgery, the patient fasted, abstained from food and drink, and completed all routine tests. The TAVR for all patients was performed by the same physician in our hospital. By combining preoperative multi-slice helical CT (MSCT) (Somatom Sensation 16, Siemens, Germany) and echocardiography to measure the valve annulus diameter, the patient was fitted with a suitable type of prosthetic valve. A stiffened guidewire was fed into a valve-equipped catheter delivery system to the aortic annulus, where the valve was released with the assistance of aortic root angiography and rapid right ventricular pacing (frequency 120–150 beats/minute, pacing time: 10-20 seconds). Immediately after the operation, echocardiography was performed to evaluate prosthetic aortic valve positioning and perivalvular leakage (PVL). After surgery, patients must avoid a high-fat, high-salt and high-sugar diet and consume plenty of vegetables and fruits. Medications such as anticoagulants and antiplatelet agents are taken as prescribed to prevent thrombosis and reduce the risk of cardiovascular events. Clinical success was defined as no intraoperative transfer to surgical thoracotomy, no prosthetic valve displacement or detachment, moderate or higher PVL or coronary artery occlusion within 30 days postoperatively, and no implantation of a permanent pacemaker [11].
Imaging examination methods
All patients were examined by MSCT 3–5 days before surgery. Experts in the TAVR team analysed the maximum diameter, minimum diameter, area, and circumference of the aortic valve annulus and the height of the openings of the left and right coronary arteries to select an appropriate valve model. In addition, echocardiography was performed before the operation and 30 days after surgery. TTE group: TTE was employed, with a probe frequency of 2.0–4.0 MHz. TEE group: TEE was utilised, with a probe frequency of 5 MHz. The examination instrument was a Philips EPIIQ 7 colour Doppler ultrasound (Nether lands). Under the display of four-chamber cardiac images, three short-axis images of the apical two-chamber and the basal, middle, and apical segments of the left ventricle in three cardiac cycles were collected and saved.
Endpoints
Surgical outcomes were analysed. (2) Differences in the detection results of the maximum diameter, minimum diameter, circumference, area, and aortic valve area (AVA) of the aortic root between MSCT and echocardiography before surgery in all patients were observed. (3) Changes in echocardiographic parameters before and after surgery in patients, including left atrial diameter (LAD), left ventricular end-diastolic diameter (LVEDD), left ventricular end-systolic diameter (LVESD), left ventricular ejection fraction (LVEF), interventricular septum thickness (IVST), posterior wall thickness (PWT), pulmonary artery systolic pressure (PASP), maximum aortic valve pressure gradient (AVPG_max_), AVPG_mean_, V_max_, and AVA, were determined. (4) Differences in postoperative hemodynamics between the observation and TTE groups, including systemic vascular resistance index (SVRI), global end-diastolic volume index (GEDV), intrathoracic blood volume index (ITBVI), and extravascular lung water index (EVLWI), were analysed. (5) Venous blood was collected from patients after examination for laboratory tests, specifically cardiac function [Brain natriuretic peptide (BNP), cardiac troponin I (cTnI), Creatine kinase iso enzyme (CK-MB)], stress response [Superoxide dismutase (SOD), Malondialdehyde (MDA)], inflammatory factors [Interleukin-1β/6 (IL-1β/6), Tumor necrosis factor-α (TNF-α)], and pain mediators [5-hydrox ytryptamine (5-HT), Endothelin-1 (ET-1), Prostaglandin E_2_ (PGE_2_), Substance P (SP)]. These tests were done by Sir Run Run Hospital, Nanjing Medical University medical laboratory.
Statistical analysis
SPSS26.0 statistically analysed all the data in this study. Count data were recorded as [n(%)], and the chi-square test was used to compare groups. Measurement data, described as (x̄±s), were compared between groups with the independent sample t-test. P<0.05 was the statistical significance level.
Results
Surgical conditions of patients
All patients were treated via the transfemoral approach, with 16 cases implanted with VenusA valves and 31 with VitaFlow valves. The operation was successful in 39 cases. Seven patients developed grade III atrioventricular block within one week after surgery and underwent permanent pacemaker implantation; one patient underwent coronary artery bypass grafting due to mechanical coronary occlusion caused by valve displacement. None of the patients experience moderate or above PVL. Figure 1 demonstrates the patient’s echocardiographic findings.
Echocardiographic findings of a patient. Female, 71 years old.
Evaluation effect of echocardiography and MSCT on the aortic root
Regarding the aortic valve annulus, we found no significant differences between echocardiography and MSCT in measuring the maximum diameter, minimum diameter, circumference, and area (P>0.05). In addition, the measurement result of AVA by echocardiography was (0.67±0.15) cm^2^, and that by MSCT was also (0.69±0.16) cm^2^, also without statistical significance (P>0.05) (Table 1).
Changes in echocardiographic parameters before and after surgery
Statistics of echocardiographic parameters showed that LAD and LVEDD did not change significantly before and after surgery (P>0.05); however, LVESD, IVST, PWT, PASP, AVPG_max_, AVPG_mean_, and V_max_ were all decreased after the operation compared to the levels before surgery, while LVEF and AVA were increased (P<0.05) (Table 2).
Baseline data of patients
We compared patients’ clinical baseline data and found no statistically significant differences in age, sex, and course of disease between the TEE group and the TTE group (P>0.05), confirming the comparability (Table 3).
Differences in hemodynamics between TEE and TTE
Comparing the hemodynamics between the TEE group and the TTE group, it can be seen that the SVRI, GEDVI, and ITBVI in the TEE group were (2200.38±586.30) dyn·s·cm^5^/m^2^, (838.43±179.51) mL/m^2^, and (1052.81±191.67) mL/m^2^, respectively, which were all higher compared to the TTE group (P<0.05); the EVLWI of the TEE group was (11.65±4.86) mL/kg, which was even lower compared with the TTE group (P<0.05) (Table 4).
Differences in cardiac function between TEE and TTE
However, in the comparison of cardiac function, we found no statistically significant differences in BNP, cTnI, and CK-MB between the TTE and TEE groups (P>0.05), suggesting that the effects of TTE and TEE on cardiac function were similar (Table 5).
Differences in stress injuries and inflammatory factors between TEE and TTE
In contrast, in comparing stress injury and in flammatory factors, we found no difference in the com parison of MDA between the two groups (P>0.05). Still, the SOD in the TEE group was higher than that in the TTE group, while IL-1β, IL-6, and TNF-α were lower than that in the control group (P<0.05), which showed that stress injury and inflammatory response were milder in the TEE group (Table 6).
Differences in pain between TEE and TTE
Finally, we assessed the pain in both groups by examining the pain mediators, and it was seen that there was no difference in the comparison of PGE_2_ between the two groups as well (P>0.05). However, 5-HT, ET-1 and SP were lower in the TEE group than in the TTE group (P<0.05), suggesting that the pain in patients in the TEE group was lower than that in the TTE group (Table 7).
Discussion
In this study, we found that compared to TTE, TEE reduces stress response and pain mediators in patients with severe AS with a higher safety profile. These results provide a new reference for the future use of TTE and TEE.
First, we observed that in the evaluation of the aortic valve annulus and AVA, there were no significant differences in various detection indicators between echocardiography and MSCT, confirming the high accuracy and reference value of echocardiography as a non-invasive and convenient detection scheme. After surgery, the LVESD, IVST, PWT, PASP, AVPG_max_, AVPG_mean_, and V_max_ patients were all lower than before the operation. At the same time, LVEF and AVA were higher, indicating a significant improvement in their cardiac function. These results align with those of Peteiro J et al. [12] when investigating the changes in echocardiographic parameters before and after surgery in patients with severe AS. TAVR is known to replace the function of the aortic valve by inserting an artificial aortic valve through a catheter into the diseased aortic valve [13]. Therefore, when TAVR is used to correct severe AS, the patient’s AVPG_mean_ will be significantly reduced, leading to a decrease in resistance load, an enhancement of cardiac blood supply function, and an increase in LVEF, which is also in line with the imaging manifestations of left ventricular reverse remodelling [14]. Meanwhile, in the follow-up study of 176 patients with aortic regurgitation by Zeng Q et al. [15], it was found that the left ventricle of patients underwent evident reverse remodelling, with a smaller left ventricular inner diameter, a thinner left ventricular wall thickness, and an increased LVEF, supporting our findings.
According to research reports, more than 0.6%-4.7% of post-TAVR patients will develop moderate or severe PVL, a condition associated with an increased in-hospital mortality rate [16]. In this study, none of the patients had moderate or severe PVL due to poor valve fitting after surgery. The reasons are as follows: (1) Preoperative MSCT and echocardiography accurately evaluated the anatomical structure of the aortic root (such as aortic root diameter [AORD] and aortic annulus diameter), providing an accurate basis for clinical practice. Moreover, the artificial aortic valve model most suitable for the patient’s aortic root structure is selected for the surgery. (2) The unique skirt design of the self-expanding artificial aortic valve adopted in our hospital effectively reduces PVL. Besides, 7 cases (15%) underwent permanent pacemaker implantation due to atrioventricular block in this study. The results of the study by Elmaraezy A et al. [17] showed that TAVR was associated with a higher risk of permanent pacemaker implantation (risk ratio (RR) 2.57, 95% confidence interval (CI) [1.36, 4.86]), vascular-access complications at 1 year (RR 1.99, 95%CI [1.04, 3.80]), and paravalvular aortic regurgitation at 30 days (RR 3.90, 95% CI [1.25, 12.12]), compared to SAVR.
Regarding echocardiography, transesophageal and transthoracic approaches are currently employed in clinical practice. However, there is still a lack of reference regarding the differences in their application in heart valve replacement for severe AS. In this regard, we compared the clinical effects of the two schemes. First of all, regarding postoperative hemodynamics, SVRI, GEDVI, and ITBVI were higher in the TEE group than in the TTE group. At the same time, EVLWI was lower, suggesting that TEE is more beneficial for improving postoperative hemodynamics in patients. As for cardiac function, we observed no difference in BNP, cTnI and CK-MB between the two groups (P>0.05), indicating no significant difference in the effect of the two examination methods on the patient’s cardiac function. However, when comparing stress response, inflammatory response, and pain conditions, we see that the TEE group is better than the TTE group in all cases, indicating that TEE has a higher safety profile. TEE and TTE are invasive mechanical manoeuvres, and the body is bound to produce a stress response during the examination. However, TEE does not affect the surgical operation and visual field and can be performed simultaneously during surgery and anaesthesia without causing multiple stressful stimuli to the patient [18]. Furthermore, a TEE examination can perform targeted exhaust and determine the amount and location of gas embolism formation, which can also reduce the stress and inflammatory response of the patient to some extent [19]. In a study by Dahl A et al. [20], they also found that in patients with cardiovascular and infectious diseases, the use of TEE for examination did not further increase the inflammatory response of the patients, which also validates the high safety of TEE. It is also because TEE has a milder stress injury and inflammatory response that the patient experience of the examination is better, and therefore, the level of pain mediators is further reduced compared to TTE.
This study has the following limitations: (1) The sample size is small, and the follow-up time is short, so it is necessary to expand the sample size and extend the follow-up time in the future to confirm the results of this study. (2) MSCT was not performed on patients after surgery in this study. Further postoperative MSCT should be performed and combined with echocardiography to jointly evaluate the changes in artificial aortic valves, heart structure, and function before and after TAVR.
Conclusion
Echocardiography has an excellent guiding effect on implementing TAVR in patients with severe AS and can assist clinicians in better completing it. In addition, TEE has a higher safety profile than TTE, reduces stress and inflammatory responses in patients, and is recommended as the first choice.
Dodatak
Data availability
Original data in this study are available from the corresponding author upon reasonable request.
Acknowledgements
Not applicable.
Conflict of interest statement
All the authors declare that they have no conflict of interest in this work.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 15359206202310.1016/j.amjcard.2023.08.001 Sarkar A Chowdhury S Kumar A Khan B Chowdhury S Gupta R et al Am J Cardiol Biomarkers as Prognostic Markers for Aortic Stenosis: A Review 37683577 · doi ↗ · pubmed ↗
- 27419013202310.1159/000529543 Rivera F B Cu M V V Cua S J De Luna D V Lerma E V Mc Cullough P A et al Cardiorenal Med Aortic Stenosis and Aortic Valve Replacement among Patients with Chronic Kidney Disease: A Narrative Review 36812906 · doi ↗ · pubmed ↗
- 3250221251417202410.1016/j.jcin.2024.08.046 Maznyczka A Prendergast B Dweck M Windecker S Généreux P Hildick-Smith D et al JACC Cardiovasc Interv Timing of Aortic Valve Intervention in the Management of Aortic Stenosis 39537272 · doi ↗ · pubmed ↗
- 411015111128202310.1007/s 10741-023-10312-7 Avvedimento M Angellotti D Ilardi F Leone A Scalamogna M Castiello D S et al Heart Fail Rev Acute advanced aortic stenosis 37083966 PMC 10403405 · doi ↗ · pubmed ↗
- 5145351432022 Guedeney P Collet J P Rev Med Interne Aortic stenosis: An update 3518116110.1016/j.revmed.2021.06.003 · doi ↗ · pubmed ↗
- 67328132202210.1016/j.tcm.2020.12.005 Maeder M T Weber L Rickli H Trends Cardiovasc Med Pulmonary hypertension in aortic valve stenosis 33346089 · doi ↗ · pubmed ↗
- 71912825202110.1177/1089253220969576 Whitener S K Francis L R Mc Murray J D Whitener G B Semin Cardiothorac Vasc Anesth Asymptomatic Severe Aortic Stenosis and Noncardiac Surgery 33136524 · doi ↗ · pubmed ↗
- 85665571135202210.1016/j.amjmed.2021.11.022 Schweiger M J Chawla K K Lotfi A Am J Med Severe Aortic Stenosis: More Than an Imaging Diagnosis 34973961 · doi ↗ · pubmed ↗