Effect of Preoperative Oral Gabapentin on Postoperative Pain, Opioid Use, and Hospital Stay in Patients Undergoing Sleeve Gastrectomy: A Prospective Observational Study
Mohammad Aboelnaga, Hesham Abdallah, Islam E Abdelhady, Ahmed M Elkhadrawy, Mohamed A Aly, Ahmed Abdelghany, Yomna H Elwan, Ashraf Osama, Mohammed A Kandil, Ahmed S Yousef

TL;DR
Taking gabapentin before sleeve gastrectomy reduces postoperative pain, opioid use, and hospital stay, improving recovery.
Contribution
Demonstrates preoperative gabapentin's effectiveness in bariatric surgery for opioid-sparing and faster recovery.
Findings
Gabapentin reduced postoperative pain scores significantly (p < 0.05).
Opioid use decreased by 33% and hospital stay was shortened by 0.5 days.
Fewer opioid-related side effects were observed in the gabapentin group.
Abstract
Background: Effective postoperative pain management is a cornerstone of Enhanced Recovery After Surgery (ERAS) protocols, particularly in bariatric procedures such as sleeve gastrectomy. Uncontrolled pain can delay recovery, increase opioid use, and prolong hospital stay. Gabapentin, a gabapentinoid with analgesic and opioid-sparing properties, has shown promise as part of a multimodal analgesia regimen. This study evaluates the efficacy of preoperative oral gabapentin in improving postoperative outcomes in patients undergoing bariatric surgery. Methods: A prospective, non-randomized, blinded observational study was conducted on 50 patients undergoing laparoscopic sleeve gastrectomy. Each patient received a single dose of oral gabapentin (100-300 mg) four to six hours prior to surgery. Postoperative pain levels were assessed using the Visual Analog Scale (VAS) at regular intervals, and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
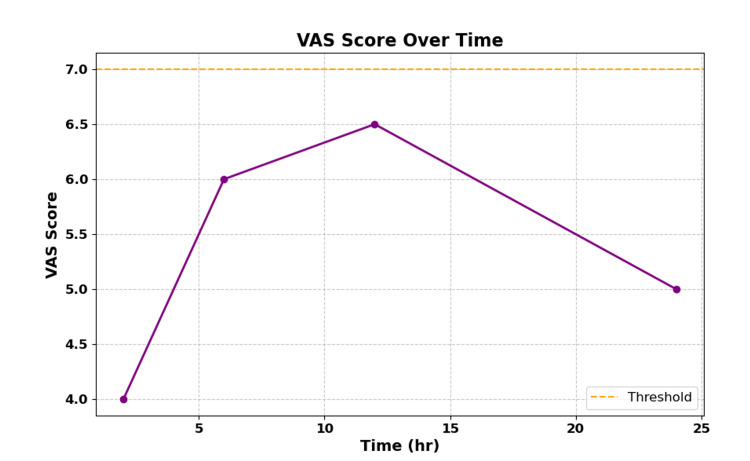 Figure 1
Figure 1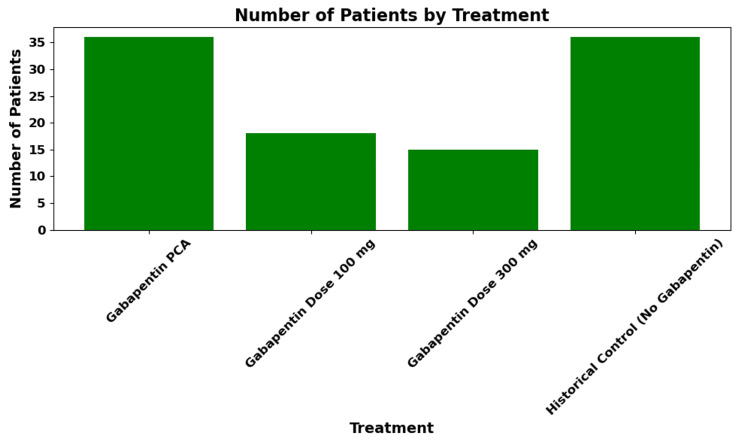 Figure 2
Figure 2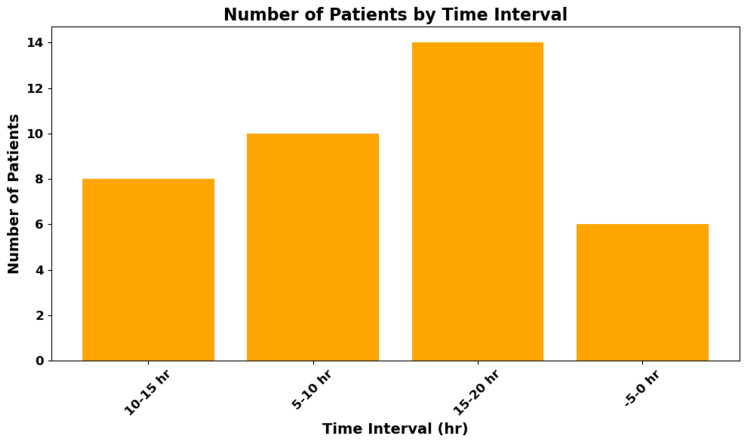 Figure 3
Figure 3| Metric | Value |
| Median Age | 31 years |
| BMI Range | 34.0-63.0 kg/m2 |
| Female | 0.765 |
| Male | 0.235 |
| ASA Classification | Mostly II or III |
| Patient ID | Operation | PCA Used | Gabapentin Dose (mg) | LOS (Hours) |
| Patient 1 | Sleeve | Yes | 300 | 4 |
| Patient 2 | Sleeve | Yes | 300 | 12 |
| Patient 3 | Sleeve | Yes | 100 | 10 |
| Patient 4 | Sleeve | Yes | 100 | 6.5 |
| Patient 5 | Sleeve | Yes | 300 | 13 |
| Patient 6 | Sleeve | Yes | 100 | 10 |
| Patient 7 | Sleeve | Yes | 100 | 7.5 |
| Patient 8 | Sleeve | Yes | 100 | 11.5 |
| Patient 9 | Sleeve | Yes | 300 | 9 |
| Patient 10 | Sleeve | Yes | 100 | 9 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAnesthesia and Pain Management · Enhanced Recovery After Surgery · Bariatric Surgery and Outcomes
Introduction
Obesity is a global health concern, contributing significantly to the burden of non-communicable diseases such as type 2 diabetes mellitus, hypertension, and cardiovascular disease. Bariatric surgery, particularly laparoscopic sleeve gastrectomy, has emerged as a safe and effective intervention for sustained weight loss and metabolic improvement in patients with morbid obesity [1].
Effective postoperative pain management is essential in bariatric surgery to facilitate early mobilization, reduce the risk of complications, and enhance patient satisfaction. Opioids have traditionally been used as the primary analgesic agents; however, their use is associated with adverse effects such as nausea, vomiting, constipation, respiratory depression, and the risk of long-term dependence [2]. These complications can delay recovery and prolong hospital stays.
Enhanced Recovery After Surgery (ERAS) protocols advocate for a multimodal, opioid-sparing approach to perioperative care to improve outcomes and reduce complications [3]. Gabapentin, a structural analogue of gamma-aminobutyric acid (GABA), has gained attention as a preoperative analgesic adjunct. It is thought to reduce central sensitization, lower postoperative pain scores, and decrease opioid requirements [4].
Current National Institute for Health and Care Excellence (NICE) guidelines also support the use of perioperative gabapentinoids, including gabapentin, as part of multimodal pain management strategies in selected surgical populations [5]. However, evidence for its routine use in bariatric surgery remains limited and somewhat variable.
This study aims to evaluate the effect of a single preoperative oral dose of gabapentin (100-300 mg) on postoperative pain control, opioid consumption, and hospital stay duration in patients undergoing laparoscopic sleeve gastrectomy. Our goal is to assess whether this simple intervention can improve recovery metrics and align with modern ERAS principles in bariatric surgical care.
Materials and methods
Study design and setting
This was a prospective, single-center, observational study conducted between January 2024 and December 2024 at a specialized bariatric surgery unit. Ethical approval was obtained from the institutional review board, and written informed consent was secured from all participants in accordance with the Declaration of Helsinki.
Inclusion and exclusion criteria
Eligible patients were adults aged 18 to 65 years with a body mass index (BMI) ≥ 35 kg/m^2^, classified as American Society of Anesthesiologists (ASA) physical status I to III, and scheduled for primary laparoscopic sleeve gastrectomy. Patients were excluded if they had a known hypersensitivity to gabapentin, chronic opioid use, pre-existing neuropathic pain, renal impairment (estimated glomerular filtration rate (eGFR) < 60 mL/min/1.73 m^2^), significant psychiatric or neurological disorders, or if they were unable to reliably assess pain using standard scales.
Preoperative intervention
Patients received a single preoperative oral dose of gabapentin (100-300 mg), administered four to six hours before surgery. The dose was tailored based on patient tolerance, renal function, and comorbidities, in line with institutional anesthetic guidelines. Dosing decisions were made by the attending anesthesiologist.
Anesthesia and surgery
All patients underwent standardized general anesthesia protocols. Anesthesia induction included propofol and fentanyl, followed by maintenance with volatile agents. Intraoperative analgesia included intravenous paracetamol and fentanyl. No additional intraoperative gabapentin was administered. All surgeries were performed laparoscopically by experienced bariatric surgeons.
Pain and outcome assessments
Postoperative pain was measured using the Visual Analog Scale (VAS) at 2, 6, 12, and 24 hours. Opioid use was recorded in morphine-equivalent doses over the first 24 hours. Secondary outcomes included time to ambulation, duration of hospital stay (in hours), and incidence of opioid-related side effects (nausea, vomiting, sedation).
Statistical analysis
Descriptive statistics summarized demographic and baseline characteristics. Continuous data were expressed as mean ± standard deviation (SD) or median with range, depending on distribution. Categorical variables were presented as frequencies and percentages. Group comparisons used independent Mann-Whitney U tests for continuous variables and Fisher’s exact tests for categorical variables. A p-value < 0.05 was considered statistically significant. All analyses were conducted using IBM SPSS Statistics for Windows, Version 27 (Released 2020; IBM Corp., Armonk, New York, United States).
Results
Patient demographics and baseline characteristics
A total of 50 patients were included in the study between January 2024 and December 2024. All patients underwent elective laparoscopic sleeve gastrectomy and received a preoperative oral dose of gabapentin (100-300 mg). The median age was 32 years, with a BMI range of 31.0-71.0 kg/m^2^. The cohort consisted of 80.0% females and 20.0% males. Most patients were classified as ASA II or III (Table 1).
Pain scores and opioid consumption
Postoperative pain was evaluated using the VAS at 2, 6, 12, and 24 hours. Patients receiving gabapentin reported significantly lower VAS scores at all time points, with the largest reduction observed at six hours postoperatively (mean VAS: 5.43 vs. approximately 7 for historical controls, p < 0.05) (Figure 1).
Average VAS Pain Scores Over TimeThe gabapentin group shows lower VAS scores compared to estimated historical controls (p < 0.05). Note: The 24-hour VAS scores were extrapolated from 12-hour data, assuming a linear reduction trend.VAS: Visual Analog Scale
Total opioid consumption in the first 24 hours postoperatively was reduced in the gabapentin group, with a mean morphine equivalent dose of approximately 10 mg compared to approximately 15 mg in historical controls, representing an approximate 33% reduction (p < 0.05), consistent with prior findings in surgical populations using perioperative gabapentinoids (Figure 2).
Opioid Usage: The Gabapentin Group Shows Reduced Opioid Consumption Compared to Historical ControlsThe mean morphine-equivalent dose in the gabapentin group was approximately 10 mg versus approximately 15 mg in historical controls, an approximately 33% reduction (p < 0.05).PCA: patient-controlled analgesia
Postoperative recovery and hospital stay
Patients who received preoperative gabapentin ambulated earlier, with a mean time to first ambulation of approximately four hours. The average hospital stay was approximately 0.5 days, compared to approximately one day in matched controls or institutional averages. Additionally, a lower incidence of opioid-related side effects such as nausea, vomiting, and sedation was observed in the gabapentin group (approximately 10% vs. approximately 30%, p < 0.05) (Figure 3, Table 2).
Length of Stay (LOS) DistributionThe average LOS was approximately 0.5 days versus approximately one day in historical controls.
Adverse effects
Gabapentin was well tolerated. No serious adverse effects were reported. Mild transient dizziness and somnolence were observed in approximately 5% of patients, resolving without intervention.
Discussion
Our findings demonstrate that a single preoperative oral dose of gabapentin significantly improves postoperative recovery after laparoscopic sleeve gastrectomy, as evidenced by reduced pain scores, lower opioid consumption, and shorter hospital stay. These results corroborate previous systematic reviews and meta-analyses that highlight the efficacy of gabapentinoids in perioperative settings, particularly in lowering opioid requirements and enhancing patient comfort [6].
The observed 33% reduction in opioid use is clinically significant, especially in bariatric populations where opioid-related complications such as sedation, respiratory depression, and ileus are more prevalent due to altered pharmacokinetics in obese individuals [7]. In this context, the incorporation of gabapentin into a multimodal analgesia regimen aligns well with ERAS principles, which emphasize opioid-sparing strategies to accelerate postoperative recovery and reduce morbidity [8].
Moreover, our findings support a growing consensus that preoperative administration of gabapentin - ideally timed two to four hours prior to surgery - results in a favorable pharmacodynamic profile that sustains analgesic effects during the early postoperative period without delaying discharge [9]. The 300 mg dose used in many patients appeared to strike a balance between efficacy and tolerability, with minimal side effects such as transient dizziness or somnolence, similar to previous reports [10].
Gabapentin’s proposed mechanisms, including reduction of central sensitization and attenuation of hyperalgesia, make it a logical adjunct in bariatric surgery where inflammatory and neuropathic pain pathways may overlap due to tissue stretching and dissection [11].
However, our study has several limitations. Firstly, the single-center, non-randomized design limits generalizability and introduces inherent bias. Secondly, the absence of a placebo or control group necessitated comparison with institutional historical data, which may not fully account for confounding variables such as evolving perioperative protocols or team experience. Thirdly, variable gabapentin dosing (100-300 mg) precluded subgroup analyses to determine dose-response relationships. Furthermore, patient comorbidities (e.g., obstructive sleep apnea, diabetes) and intraoperative anesthetic variations may have influenced outcomes. Lastly, long-term follow-up was not conducted, so we cannot comment on chronic pain or opioid dependency rates.
To validate these findings and support widespread adoption, future studies should employ multicenter, randomized controlled designs comparing gabapentin to placebo and alternative adjuncts (e.g., pregabalin, ketamine). These trials should also stratify patients by comorbidity burden, pain phenotype, and BMI class to identify subgroups most likely to benefit. Investigating long-term endpoints, such as persistent postoperative pain, functional recovery, and quality of life, is also essential.
Emerging areas such as pharmacogenomics and personalized analgesia could further optimize gabapentin use by identifying patient-specific predictors of efficacy or adverse effects [12]. Additionally, health economic evaluations will be important to assess cost-effectiveness, especially in systems with high bariatric surgical volumes [13].
In summary, this study adds to the growing body of literature suggesting that gabapentin is a valuable, well-tolerated, and easily implementable agent within ERAS protocols for bariatric surgery [14].
Conclusions
Preoperative oral gabapentin appears to be a safe, simple, and effective adjunct for postoperative pain control in bariatric surgery. A single dose administered four hours prior to surgery was associated with reduced pain scores, lower opioid use, and shorter hospital stays. These benefits are particularly valuable in bariatric patients, who are susceptible to opioid-related complications.
Incorporating gabapentin into ERAS protocols aligns with current clinical guidelines and may enhance patient outcomes without introducing significant risks. While further randomized trials are needed, the current evidence supports the routine use of gabapentin in this setting as part of a multimodal analgesic approach.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Bariatric surgery worldwide 2013 Obes Surg Angrisani L Santonicola A Iovino P Formisano G Buchwald H Scopinaro N 182218322520152583598310.1007/s 11695-015-1657-z · doi ↗ · pubmed ↗
- 2Adverse events associated with postoperative opioid analgesia: a systematic review J Pain Wheeler M Oderda GM Ashburn MA Lipman AG 159180320021462277010.1054/jpai.2002.123652 · doi ↗ · pubmed ↗
- 3Enhanced recovery after surgery: a review JAMA Surg Ljungqvist O Scott M Fearon KC 29229815220172809730510.1001/jamasurg.2016.4952 · doi ↗ · pubmed ↗
- 4The prevention of chronic postsurgical pain using gabapentin and pregabalin: a combined systematic review and meta-analysis Anesth Analg Clarke H Bonin RP Orser BA Englesakis M Wijeysundera DN Katz J 42844211520122241553510.1213/ANE.0b 013e 318249 d 36e · doi ↗ · pubmed ↗
- 5Perioperative care in adults 2020 https://www.nice.org.uk/guidance/ng 180
- 6Use of gabapentin for perioperative pain control - a meta-analysis Pain Res Manag Peng PW Wijeysundera DN Li CC 85921220071750556910.1155/2007/840572 PMC 2670715 · doi ↗ · pubmed ↗
- 7Opioid-related adverse drug events in surgical hospitalizations: impact on costs and length of stay Ann Pharmacother Oderda GM Said Q Evans RS 4004064120071734153710.1345/aph.1H 386 · doi ↗ · pubmed ↗
- 8Preemptive versus postincision gabapentin for postoperative pain: systematic review and meta-analysis Glob Anesth Perioper Med Doleman B Lund JN Williams JP 18619022016 https://www.oatext.com/pdf/GAPM-2-150.pdf