Intracranial Major Artery Stenosis Associated With Acute Posterior Multifocal Placoid Pigment Epitheliopathy
Kosuke Suzuki, Kaori Sumi, Teruaki Masuda, Ryoko Oki, Atsunobu Takeda, Noriyuki Kimura

TL;DR
A 16-year-old girl with APMPPE developed cerebral infarctions and artery stenosis, which improved with immunotherapy and antiplatelet drugs.
Contribution
Highlights the association between APMPPE and intracranial artery stenosis in young patients.
Findings
APMPPE can cause cerebral infarctions and intracranial artery stenosis in juveniles.
Immunotherapy and antiplatelet drugs resolved arterial stenosis and neurological symptoms.
Vascular stenosis may progress despite immunotherapy, requiring close monitoring.
Abstract
Acute posterior multifocal placoid pigment epitheliopathy (APMPPE) is an immune-mediated chorioretinal disease that can cause cerebral infarctions in young individuals. We report the case of a 16-year-old girl who developed intracranial major artery stenosis. She presented with eye pain and microcerebral infarctions, and CSF examination showed lymphocytosis and elevated interleukin-6 (IL-6). Ophthalmoscopy revealed multiple white posterior pole lesions; hence, she was diagnosed with cerebral infarction due to APMPPE. Five weeks after the initiation of prednisolone (PSL) treatment, she developed asymptomatic intracranial arterial stenosis. The addition of intravenous methylprednisolone (IVMP) and antiplatelet drugs resulted in the complete resolution of arterial stenosis and neurological symptoms. It is important to recognize APMPPE as a potential cause of juvenile cerebral infarction…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
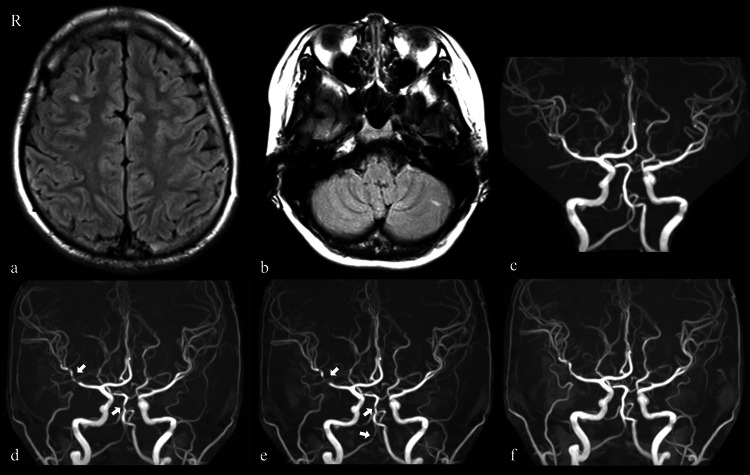 Figure 1
Figure 1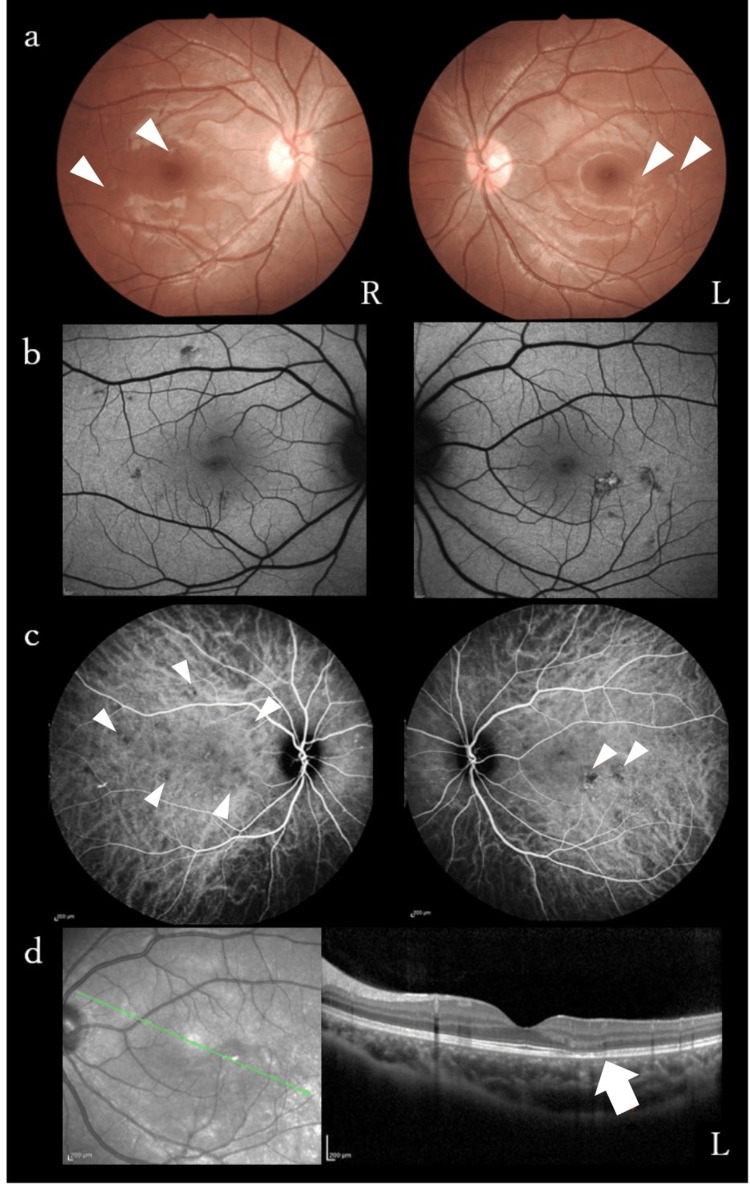 Figure 2
Figure 2| Author (year) | Age/Sex | Timing of stroke after ocular symptoms | Stenotic vessels | CSF findings | Immunothrapy (maximum dose) | Exacerbation during immunotherapy/timing | Immunotherapy at the time of exacerbation | Outcome |
| Smith [ | 25/M | 2 months | Right PCA | WBC 100 cells/mm3, protein 30 mg/dl | Oral PSL (60 mg/d) | (-) | NA | Decreased vision of both eyes |
| Wilson [ | 24/M | 1 month | Multifocal | WBC 0 cells/mm3, protein 66 mg/dl | Oral PSL (40 mg/d) | (+)/1 day | Oral PSL (20 mg/d) | Died |
| De Vries [ | 23/M | 3 days | Left MCA, right PCA | NA | (-) | (-) | NA | Died |
| Luneau [ | 43/M | 1 month | Right ACA, MCA | WBC 253 cells/mm3, protein 57 mg/dl | IVMP (1,000 mg/d), oral PSL, CPA (150 mg/d), AZA (50 mg/d) | (+)/6 months | Oral PSL (10 mg/d), switching from CPA to AZA | Mild decrease in left finger movements |
| Volbers [ | 22/M | 1 month | Left MCA | WBC 16 cells/mm3 | Oral PSL, AZA | (-) | NA | Full recovery |
| Matamala [ | 15/M | 1 year | Left PCA | WBC 13 cells/mm3 | Oral PSL, AZA | (-) | NA | NA |
| Case [ | 23/M | 5 months | Bilateral ACA | Normal | IVMP, oral PSL (80 mg/d) | (-) | NA | Left leg weakness |
| Algahtani [ | 26/F | 3 months | Bilateral ACA, MCA | WBC 10 cells/mm3, normal protein | IVMP, oral PSL (80 mg/d) | (-) | NA | Full recovery |
| Tsuboyama [ | 55/M | 3 weeks | Left ACA, right SCA, PCA | WBC 21 cells/mm3, protein 40 mg/dl | IVMP, oral PSL, CPA | (+)/5 months | Oral PSL (details are unclear) | Improvement |
| Tsuboyama [ | 64/M | 1 month | Bilateral MCA, PCA and SCA, BA, right VA | NA | IVMP, oral PSL (80 mg/d), CPA | (+)/3 weeks | Oral PSL (60 mg/d) | Died |
| Maamari [ | 21/M | 1 month | Multifocal | NA | Oral PSL (80 mg/d) | (+)/18 days | Oral PSL (80 mg/d) | Died |
| Oki [ | 29/M | 1 month | Right PCA | WBC 16 cells/mm3, protein 53.7 mg/dl | Oral PSL (50 mg/d) | (-) | NA | Full recovery |
| Present case | 16/F | Simultaneous | Right MCA, BA, right PCA, VA | WBC 26 cells/mm3, protein 46.6 mg/dl | IVMP, oral PSL (60 mg/d) | (+)/5 weeks | Oral PSL (60 mg/d) | Full recovery |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOcular Diseases and Behçet’s Syndrome · Cerebral Venous Sinus Thrombosis · Retinal and Optic Conditions
Introduction
Acute posterior multifocal placoid pigment epitheliopathy (APMPPE), first described by Gass in 1968, is an inflammatory chorioretinopathy characterized by acute visual symptoms and yellowish-white placoid lesions at the level of the retinal pigment epithelium, located primarily in the posterior pole, and occurs in young individuals aged 20-40 years [1,2]. Most cases of APMPPE present only with ocular symptoms and resolve within two-three months [2]. However, it has been reported that APMPPE is sometimes accompanied by central nervous system involvement, such as stroke [2-5]. Cerebral vasculitis has been proposed as a mechanism of cerebral infarction associated with APMPPE based on histological findings and CSF pleocytosis [3,6-10].
Here, we report the case of a 16-year-old girl who presented with cerebral infarction and major intracranial artery stenosis associated with APMPPE. She was treated with oral prednisolone (PSL) but developed asymptomatic intracranial major artery stenosis. The patient responded favorably to intravenous methylprednisolone (IVMP) and cilostazol. This report aims to provide insights into the management and treatment of stroke associated with major intracranial artery stenosis in patients with APMPPE.
Case presentation
A 16-year-old Japanese girl presented to a local clinic with transient dizziness, vomiting, headache, right eye pain, diplopia, and numbness of her lips and left extremities. MRI of the head revealed multiple acute small cerebral infarctions in the right frontal lobe and left cerebellar hemisphere, without evidence of cerebrovascular stenosis (Figure 1a, 1b, 1c), and she was referred to Oita University one week after onset.
Imaging findings of the patienta-c: MRI of the head revealed multiple cerebral infarctions in the right frontal lobe and left cerebellar hemisphere, with no evidence of vascular stenosis.d: MRA performed on day 34 showing stenosis of the right MCA and BA (arrows).e: By day 47, stenosis of the MCA and BA had progressed, and new stenosis was observed in the right posterior cerebral and right vertebral arteries (arrows).f: The MRA findings normalized by day 52.BA: Basilar artery; MCA: Middle cerebral artery; MRA: Magnetic resonance angiography
The patient had no risk factors for cerebral infarction or relevant family history. Physical examination revealed mild weakness and deep sensory disturbance of the left lower extremity, without headache or fever. Laboratory examination revealed a normal coagulation system with no elevation in C-reactive protein or white blood cell count (WBC). She was negative for antinuclear antibodies and weakly positive for immunoglobulin G (IgG) anticardiolipin antibodies at 13 U/mL (≤ 12U/mL), but the repeat test was negative. CSF analysis showed lymphocytic pleocytosis (26 cells/mm^3^; normal values < 5 cells/mm^3^) and an elevated protein level (46.6 mg/dl; normal, ≤ 40.0 mg/dl). The CSF interleukin-6 (IL-6) level was as high as 109 pg/mL, IgG index was 0.52, and oligoclonal bands were negative. Electrocardiography and transesophageal echocardiography results were normal, and contrast-enhanced CT of the trunk presented no evidence of a thrombus or malignancy. We performed an ophthalmologic evaluation three weeks after the initial symptoms because the patient had ocular symptoms at the onset of the stroke. Ophthalmoscopy, fundus autofluorescence, and optical coherence tomography revealed scattered scars extending from the outer retina to the retinal pigment epithelium of the posterior pole in both eyes (Figure 2a, 2b, 2d). Late phase indocyanine green angiography revealed multiple hypocyanescent lesions due to occlusion of the choriocapillaris (Figure 2c). APMPPE, multiple evanescent white dot syndrome (MEWDS), and punctate internal choroidopathy (PIC) were considered as differential diagnoses for hypofluorescent lesions confined to the posterior pole in young women. MEWDS was excluded due to the bilateral presentation, and PIC was deemed unlikely because of the absence of well-circumscribed, small, round exudative lesions. Based on these findings, she was diagnosed with APMPPE in the inactive phase.
Multimodal ocular imaging findings of the patienta, b: Ophthalmoscopy and fundus autofluorescence revealed scattered scars of retinal pigment epithelium in the posterior pole (arrowheads).c: Indocyanine green angiography revealed punctate hypocyanescent lesions from the early to late phases, suggesting occlusion of the choriocapillaris (arrowheads).d: Optical coherence tomography of the left eye showed outer retinal architectural disruption (arrow) and thickened choroid with dilated vessels.
The patient was diagnosed with cerebral infarction associated with APMPPE since there were no specific blood tests or imaging findings for other systemic small vessel occlusive vasculitis and was started on PSL 60 mg/day and warfarin therapy.
CSF findings improved over time after the start of treatment; however, on day 34, magnetic resonance angiography (MRA) revealed stenosis of the right middle cerebral artery (MCA) and basilar artery (BA) without accompanying clinical symptoms (Figure 1d). In the early phase following treatment with IVMP, stenosis of the MCA and BA progressed, and new stenotic lesions developed in the right posterior cerebral artery (PCA) and right vertebral artery (VA) (Figure 1e). However, with continued oral PSL and a switch in antithrombotic therapy from warfarin to cilostazol in anticipation of vasodilatory effects, the cerebrovascular stenosis resolved by day 52 (Figure 1f). Neurological symptoms resolved completely, and the patient was discharged on day 56. Cilostazol was discontinued on day 167, and oral PSL was gradually tapered over two years.
Discussion
Here, we describe a case of APMPPE presenting with cerebral infarction and major intracranial artery stenosis. This case demonstrates that APMPPE should be considered in juvenile patients with both cerebral infarction and ocular symptoms. Furthermore, cerebrovascular disease can be exacerbated during immunotherapy, and a combination therapy with PSL and antiplatelet agents may be useful. These findings provide insights into the management and treatment of stroke patients with APMPPE.
This case was characterized by a vascular lesion affecting medium-sized vessels rather than small vessels. CNS vasculitis associated with APMPPE mainly involves the small arteries and less commonly affects medium-sized vessels, as in the present case [6,11]. Therefore, we reviewed the literature for case reports of patients with APMPPE who developed intracranial medium-sized artery stenosis. We identified 12 cases through searches of PubMed and Google Scholar up to March 2025 using the search terms "APMPPE," "cerebral vasculitis," "cerebral infarction," and "stroke" [4,6-9,11-16]. A summary of the 13 cases, including ours, is presented in Table 1.
As shown in Table 1, most patients with APMPPE and major cerebral artery stenosis were male (84.6%), with a median age of 29.7 years (range: 15-64 years). While ophthalmic APMPPE affects males and females equally, neurological complications have been reported to be more common in men, and our study showed a similar trend. All patients, except the present case, developed cerebral infarction after the onset of ocular symptoms. The median interval to stroke was nine weeks (range: 0-12 months); three patients experienced stroke more than three months after diagnosis, with the longest interval being 12 months. Immunotherapy with PSL was administered to 12 patients, five of whom also received immunosuppressants. In the present case, a new intracranial major artery stenosis developed despite immunotherapy. Notably, six patients (46.2%), including this patient, experienced worsening of cerebrovascular disease, including new infarcts or progressive arterial stenosis, following the initiation of immunotherapy. Of these cases, three deteriorated within one month, while the remaining three, including the present case, showed worsening beyond one month after treatment, up to six months [7,11,14,15]. All three cases of early exacerbations were fatal, whereas neurological outcomes were good in those who had exacerbations beyond one month. Four patients (30.8%) died of cerebrovascular disease and its complications. One patient did not receive immunotherapy, and one underwent rapid steroid tapering or discontinuation [7,9].
These findings suggest that the appearance of major intracranial arterial stenosis should be monitored for approximately one month after APMPPE diagnosis. CNS vasculitis associated with APMPPE usually occurs after the diagnosis of APMPPE, but as in our case, it can occur simultaneously with ocular symptoms; therefore, APMPPE should be considered when patients present with cerebral infarction and ocular symptoms. Furthermore, if arterial stenosis develops, the dose of immunotherapy should be maintained or adjusted carefully during the first month. In addition, vascular stenosis may progress even during immunotherapy; therefore, careful monitoring with head imaging, such as MRI, is recommended for approximately six months. In our case, the vascular stenosis progressed asymptomatically; therefore, regular monitoring with MRI was useful.
Antithrombotics were administered in combination with immunotherapy. For CNS vasculitis, European guidelines suggest adjunctive aspirin therapy for patients with medium-to-large vessel involvement, and one study has shown an association between aspirin and long-term remission [17,18]. The benefit of antithrombotic therapy in the cerebrovascular disease of APMPPE has not been proven; however, in this case and Algahtani's report, using antiplatelet agents, the patient recovered completely [4]. Adjunctive antiplatelet therapy might be beneficial in patients with APMPPE involving medium-sized arteries. Further clinical data are needed, since the optimal type of antiplatelet agent remains unclear.
A limitation of this study is the small number of cases. While it is important to note that findings from a few cases are not generalizable, the aim of this report is to promote caution in the management and treatment of APMPPE with intracranial major artery stenosis. In addition, the data included in this review are heterogeneous in terms of publication period, reporting detail, and diagnostic criteria, which may limit direct comparisons across cases. Furthermore, the definition of clinical outcomes such as “improvement” may differ across reports, introducing an additional layer of uncertainty to the outcome analysis. It remains unclear which cases of APMPPE develop medium-sized vasculitis rather than small-vessel involvement and which cases worsen during immunotherapy. To the best of our knowledge, no differences have been observed in the timing of vasculitis onset or CSF findings. Additional case reports are needed to improve our understanding of this condition.
Conclusions
In conclusion, APMPPE is a cause of juvenile stroke with ocular symptoms and may have a fatal prognosis when associated with intracranial arterial stenosis. Cerebrovascular disease may be exacerbated during immunotherapy, requiring careful follow-up, such as by head MRI. The combination of immunotherapy and antiplatelet agents may improve clinical outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Acute posterior multifocal placoid pigment epitheliopathy Arch Ophthalmol Gass JD 177185801968566188210.1001/archopht.1968.00980050179005 · doi ↗ · pubmed ↗
- 2Acute posterior multifocal placoid pigment epitheliopathy: clinical presentation and risk of stroke and transient ischaemic attack Br J Ophthalmol Niederer RL Samalia PD Chen YH 39840410820243665795910.1136/bjo-2022-321517 · doi ↗ · pubmed ↗
- 3Neurological complications of acute multifocal placoid pigment epitheliopathy J Clin Neurosci Brownlee WJ Anderson NE Sims J Pereira JA 76803120162718395810.1016/j.jocn.2016.02.012 · doi ↗ · pubmed ↗
- 4Neurological manifestations of acute posterior multifocal placoid pigment epitheliopathy J Clin Neurol Algahtani H Alkhotani A Shirah B 4604671220162781941610.3988/jcn.2016.12.4.460PMC 5063873 · doi ↗ · pubmed ↗
- 5Ocular outcome and frequency of neurological manifestations in patients with acute posterior multifocal placoid pigment epitheliopathy (APMPPE)J Ophthalmic Inflamm Infect Thomas BC Jacobi C Korporal M Becker MD Wildemann B Mackensen F 125131220122257339810.1007/s 12348-012-0077-7PMC 3438297 · doi ↗ · pubmed ↗
- 6Acute posterior multifocal placoid pigment epitheliopathy associated with stroke: a case report and review of the literature J Stroke Cerebrovasc Dis Case D Seinfeld J Kumpe D Folzenlogen Z Jones W Simpson J Hughes R 030224201510.1016/j.jstrokecerebrovasdis.2015.06.02226277292 · doi ↗ · pubmed ↗
- 7Acute posterior multifocal placoid pigment epitheliopathy and cerebral vasculitis Arch Ophthalmol Wilson CA Choromokos EA Sheppard R 7968001061988337000910.1001/archopht.1988.01060130866042 · doi ↗ · pubmed ↗
- 8Teaching neuroimages: stroke and bilateral visual loss in a young adult: more than coincidence Neurology Volbers B Kaldefoss K Bergua A Kloska S Schwab S Köhrmann M 0178201210.1212/WNL.0b 013e 31824 c 46e 322431745 · doi ↗ · pubmed ↗