Tuberculosis as a significant cause of uveitis-related blindness: current referral trends at a tertiary uveitis center in Indonesia
Ikhwanuliman Putera, Ulifna Alfiya Sifyana, Saskia M. Rombach, Johannes R. Vingerling, P. Martin van Hagen, Rina La Distia Nora

TL;DR
In Indonesia, nearly 10% of uveitis patients have active tuberculosis, and over half experience blindness in their worse-seeing eye.
Contribution
This study highlights the high prevalence of active TB among uveitis patients in Indonesia and the significant risk of blindness.
Findings
Active systemic TB was diagnosed in 9.8% of uveitis patients.
Blindness in the worse-seeing eye was observed in 56.1% of uveitis patients.
Most TB-related uveitis patients sought care due to eye problems.
Abstract
•Active systemic tuberculosis was diagnosed in approximately one in 10 patients with uveitis.•More than half of referred patients with uveitis had blindness in worse-seeing eye.•Eye problems were the main reason patients with uveitis with active tuberculosis sought medical care. Active systemic tuberculosis was diagnosed in approximately one in 10 patients with uveitis. More than half of referred patients with uveitis had blindness in worse-seeing eye. Eye problems were the main reason patients with uveitis with active tuberculosis sought medical care. Uveitis may lead to blindness if improperly treated, yet the data on blindness due to uveitis, particularly, in low-resource countries, remain limited. In high–tuberculosis (TB) burden countries such as Indonesia, active systemic TB is among the leading causes of infectious uveitis. The combined impact of blindness, uveitis, and TB…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
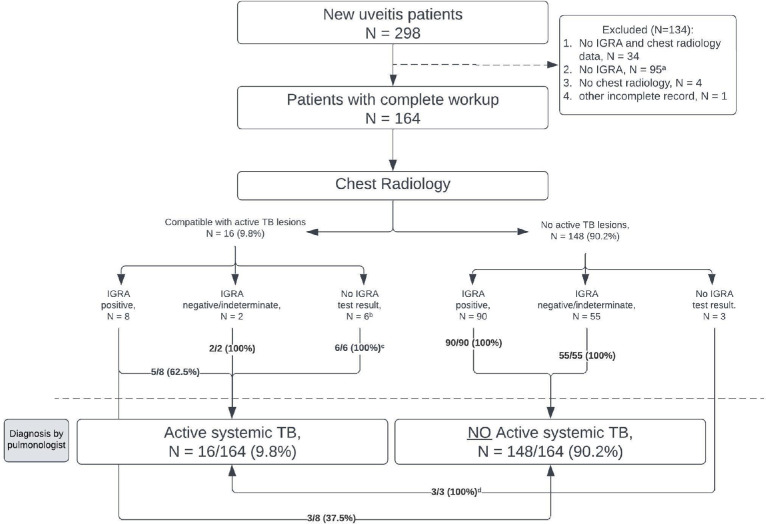 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOcular Diseases and Behçet’s Syndrome · Infectious Diseases and Tuberculosis · Sarcoidosis and Beryllium Toxicity Research
Introduction
Uveitis, an inflammation of the uveal tract, may lead to irreversible blindness due to complications, such as secondary glaucoma, secondary cataract, optic neuropathy, retinal scars, macular edema, or even phthisis, if improperly treated [1]. In total, uveitis is estimated to contribute for up to 10% of blindness in developed countries [1]. However, population-based data on blindness due to uveitis in low-resource countries such as Indonesia are lacking because the current epidemiological survey remains largely focused on avoidable causes of blindness such as cataracts [2]. Notably, the prevalence of infectious and non-infectious causes of uveitis varies between high- and low-resource countries, with infectious causes being more prevalent in the latter [1]. In Indonesia, ocular toxoplasmosis, followed by uveitis associated with active systemic tuberculosis (TB), are the two leading causes of infectious uveitis [3]. From a health economic perspective, the combination of blindness, uveitis, and TB collectively impose a substantial economic burden because of direct and indirect costs. It is estimated that the direct medical costs for uveitis alone, such as those for corticosteroids or other immunosuppressants, are 4.3 times higher for patients who are blind than those without vision loss at presentation [4]. In addition, the mean direct medical cost incurred for TB treatment for each patient is estimated to be as high as US1253 [5]. Therefore, it is important to objectively assess the current situation of the triple burden of uveitis, blindness, and active TB. As an initial step, (i) we aimed to report the current proportion of uveitis presented with active systemic TB among newly referred patients with uveitis and (ii) report the proportion of blindness among patients with TB-related uveitis, including a subgroup with an undetermined cause of uveitis but positive Quantiferon-TB Gold Plus (QFT) test results in addition to those with active systemic TB.
Materials and methods
Between February 2023 and January 2024, 164 newly referred patients with uveitis who completed routine uveitis workup were identified at the uveitis outpatient clinic of Cipto Mangunkusumo Kirana Eye Hospital, a tertiary care hospital in Jakarta. The workup minimally included complete blood counts, liver and kidney function tests, syphilis serology, HIV screening, QFT, and chest X-ray, with additional tests to rule out other infectious and non-infectious causes of uveitis tailored based on the clinical presentation. Patients with incomplete medical record data were excluded (Figure 1). There was no significant difference in age, sex, or proportion of blindness in the worse-seeing eye between patients included and excluded from the analysis.Figure 1. Flow of active systemic TB evaluation among patients with uveitis.Chest radiology, primarily, CXR, and the IGRA, using QFT test, were performed simultaneously during the initial workup, with a QFT cutoff of 0.35 IU/ml. Mantoux testing was far less commonly performed in our center and, therefore, was not taken into account in this analysis.ATT, anti-TB treatment; CXR, chest X-rays; IGRA, interferon-γ release assay; QFT, Quantiferon-TB Gold Plus; TB, tuberculosis.^a^Of the 95 excluded patients without IGRA but with CXR, nine had findings suspicious for active pulmonary TB but lacked follow-up or diagnostic confirmation by pulmonologists.^b^Four of six patients had Mantoux test performed; three (75%) showed induration ≥10 mm.^c^Three patients had been diagnosed with active pulmonary TB and started ATT at the previous hospital, one had a history of TB, and two were diagnosed through clinical and radiological means.^d^One patient was HIV-positive and had been on ATT for 3 months before the CXR performed at uveitis presentation, one patient had biopsy-proven TB lymphadenitis, and another, a 16-year-old patient, was diagnosed using the TB pediatric scoring system.Figure 1
We retrospectively collected data on sex, age, workup results, and visual acuity at the time of initial presentation. Best-corrected visual acuity was assessed by trained nurses using a Snellen chart. For this study, blindness was defined as a best-corrected visual acuity of less than 3/60 in the worse-seeing eye because uveitis can occur unilaterally, and unilateral blindness is known to sufficiently impair quality of life [6].
Data on TB status, as assessed by pulmonologists following a national guideline for TB control [7], were retrieved. Cases without interferon-γ release assay test results were still included if the pulmonologist was able to determine the status of active disease. In addition to identifying cases of uveitis associated with active systemic TB, we categorized patients into two additional groups: those with an undetermined cause of uveitis who were QFT-positive (“QFT-positive uveitis”) and those with an established non-TB cause of uveitis or an undetermined cause with a negative QFT result (“other uveitis”).
This study was approved by the local ethical committee, Faculty of Medicine University of Indonesia (KET-850/UN2.F1/ETIK/PPM.00.02/2022).
Results and discussion
Among the 164 patients with uveitis included in this study, 16 (9.8%) were diagnosed with active systemic TB (Figure 1). This group comprised two patients with disseminated TB (both had miliary pulmonary TB and TB lymphadenitis), one patient with active pulmonary TB with a GeneXpert test positivity from sputum sample, one with TB pleurisy, one with biopsy-proven TB lymphadenitis, and 11 patients with sputum smear–negative active pulmonary TB supported by chest radiological findings (culture was not performed). Among the latter group, one patient was also HIV-positive. Interestingly, of all 16 patients, 14 initially sought the first medical attention due to their ophthalmological symptoms.
From an ophthalmological perspective, the proportion of blindness in the worse-seeing eye among newly referred patients with uveitis was 56.1% (92 of 164 patients), whereas it was 64.4% (94 of 146 patients) in our previous data from the 2014-2015 period (Table 1). Active systemic TB cases were observed in 9.8% of patients, whereas it was 8.2% previously. In addition, the current proportion of blindness was slightly higher in patients with uveitis with active systemic TB and QFT-positive uveitis than in those with other uveitis (56.3% vs 61.1% vs 51.3%, respectively) (Table 1). The distribution of anatomical subtypes of uveitis between groups in the current cohort is presented in the Supplementary Table.Table 1. Characteristics of patients with uveitis referred to our center: current situation and 2014-2015 period.Table 1. La Distia Nora et al.’s study (2014-2015)Current study (2023 – 2024)Total patientsActive Systemic TBQFT-positive uveitisOther causes of uveitisTotal patientsActive Systemic TBQFT-positive uveitisOther causes of uveitisNumber of patientsa14612/146 (8.2%)58/146 (39.7%)76/146 (52.1%)16416/164 (9.8%)72/164 (43.9%)76/164 (46.3%)CharacteristicsSex Female75 (51.4%)4 (33.3%)42 (72.4%)29 (38.2%)94 (57.3%)11 (68.8%)45 (62.5%)38 (50.0%) Male71 (48.6%)8 (66.7%)16 (27.6%)47 (61.8%)70 (42.7%)5 (31.3%)27 (37.5%)38 (50.0%)Age <25 years old22 (15.1%)2 (16.7%)5 (8.6%)15 (19.7%)12 (7.3%)4 (25.0%)4 (5.6%)4 (5.3%) 25-50 years old76 (52.1%)6 (50.0%)28 (48.3%)42 (55.3%)117 (71.3%)10 (62.5%)53 (73.6%)54 (71.1%) >50 years old48 (32.9%)4 (33.3%)25 (43.1%)19 (25.0%)35 (21.3%)2 (12.5%)15 (20.8%)18 (23.7%)Previous TB Yes23 (15.8%)0 (0%)15 (25.9%)8 (10.5%)7 (4.3%)3 (18.8%)b3 (4.2%)1 (1.3%) No123 (84.2%)12 (100%)43 (74.1%)68 (89.5%)157 (95.7%)13 (81.3%)69 (95.8%)75 (98.7%)Contact TB Yes11 (7.5%)1 (8.3%)7 (12.1%)3 (3.9%)4 (2.4%)0 (0%)3 (4.2%)1 (1.3%) No135 (92.5%)11 (91.7%)51 (87.9%)73 (96.1%)160 (97.6%)16 (100%)69 (95.8%)75 (98.7%)Worse-seeing eye vision categoryc <3/60 (blind)94 (64.4%)8 (66.7%)37 (63.8%)49 (64.5%)92 (56.1%)9 (56.3%)44 (61.1%)39 (51.3%) ≥3/6052 (35.6%)4 (33/3%)21 (36.2%)27 (35.5%)72 (43.9%)7 (43.8%)28 (38.9%)37 (48.7%)QFT, Quantiferon-TB Gold Plus; TB, tuberculosis.aIn the 2014-2015 data, the total number of new patients was 247, of whom 146 (59.1%) were included after exclusions, including those without complete workups. In the current 2023-2024 data, 164 of 298 patients (55.0%) were included.bThe three patients with active systemic tuberculosis were tested using GeneXpert to assess rifampicin resistance, and none showed evidence of resistance. In accordance with current national guidelines (https://repository.kemkes.go.id/book/124, in Bahasa) and given the presence of active uveitis, treatment was initiated promptly in all three patients using the first line regimen 2RHZE/7RH.cChi-square test P = 0.489.
Because only four patients with active systemic TB had started antitubercular treatment (ATT) before referral to our center, we encourage that active systemic TB evaluations and confirmation be completed before referral to avoid delays in initiating ATT for those who need it. It is well-established that a single active pulmonary TB patient can infect up to 45 other individuals [8]. We speculate that patients with uveitis with active systemic (pulmonary) TB who are blind may pose a higher transmission risk because their dependence on others for daily living could increase close-contact exposure [9]. In addition, we observed that three of 16 (18.8%) cases with active systemic TB had a history of TB with ATT completion (Table 1), raising questions about whether the current active TB represents recurrence or reinfection and whether this might reflect inadequate previous ATT. Moreover, the high proportion of blindness in QFT-positive uveitis cases highlights the need to investigate whether a subset of these cases represents true extrapulmonary TB rather than merely reflecting previous M. tuberculosis exposure. The proportion of patients with QFT-positive uveitis in this cohort (excluding those with active systemic TB, 72 of 148 = 48.6%) exceeds the estimated prevalence of latent TB infection in the general Indonesian population, which is approximately 35% [10]. Although this study is not designed to evaluate the risks and benefits of ATT for patients with QFT-positive uveitis, this question is currently being investigated in a separate prospective study we are conducting (ClinicalTrials.gov, NCT05005637), which we anticipate will offer clearer guidance on the initiation of ATT. Recently, we reported that although several ocular features are highly suggestive of active TB uveitis, some cases may present with atypical manifestations [11]. Judicious use of advanced diagnostics, such as the polymerase chain reaction from ocular fluid we recently described [12], although not discussed here, could also be helpful after careful validation.
We acknowledge that many patients were excluded due to incomplete medical records, particularly, incomplete workups (non-completers), which may have led to over- or under-estimation of the reported proportions. Similar limitations were present in the previous study we compared with (Table 1) [3]. Some of these non-completers may arguably have had undiagnosed active TB and uveitis-related blindness due to inappropriate management. Reducing incomplete workups and maintaining patients in proper management in real-world practice is crucial to mitigating this potential public health burden.
Based on our findings, active systemic TB remains frequently observed among newly referred patients with uveitis, affecting approximately one in 10 patients with uveitis. Over half of TB-related uveitis cases present with blindness. To mitigate potential significant delays in the uveitis referral process, we strongly advocate for thorough TB evaluations in all patients with uveitis, particularly, in high–TB burden settings such as ours. ATT should be initiated promptly in patients with evidence of active systemic TB. Visual outcome after treatment and the socioeconomic impacts of this “triple burden” of blindness, uveitis, and TB require further investigations.
Declarations of competing interest
The authors have no competing interests to declare.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Durrani O.M.Meads C.A.Murray P.I.Uveitis: a potentially blinding disease Ophthalmologica 218200422323610.1159/00007861215258410 · doi ↗ · pubmed ↗
- 2Rif’Ati L.Halim A.Lestari Y.D.Moeloek N.F.Limburg H.Blindness and visual impairment situation in Indonesia based on rapid assessment of avoidable blindness surveys in 15 provinces Ophthal Epidemiol 28202140841910.1080/09286586.2020.185317833380229 · doi ↗ · pubmed ↗
- 3La Distia Nora R.Sitompul R.Bakker M.Susiyanti M.Edwar L.Sjamsoe S.Tuberculosis and other causes of uveitis in Indonesia Eye (Lond)32201854655410.1038/eye.2017.23129099497 PMC 5848274 · doi ↗ · pubmed ↗
- 4Sriranganathan A.Mihalache A.Grad J.Miranda R.N.Felfeli T.Economic burden and cost-effectiveness of management of non-infectious uveitis: a systematic review Ocul Immunol Inflam 202512110.1080/09273948.2025.245047239773098 · doi ↗ · pubmed ↗
- 5Portnoy A.Yamanaka T.Nguhiu P.Nishikiori N.Garcia Baena I.Floyd K.Menzies N.A.Costs incurred by people receiving tuberculosis treatment in low-income and middle-income countries: a meta-regression analysis Lancet Glob Health 112023 e 1640 e 164710.1016/S 2214-109X(23)00369-837734806 PMC 10522775 · doi ↗ · pubmed ↗
- 6Vu H.T.Keeffe J.E.Mc Carty C.A.Taylor H.R.Impact of unilateral and bilateral vision loss on quality of life Br J Ophthalmol 89200536036310.1136/bjo.2004.04749815722319 PMC 1772562 · doi ↗ · pubmed ↗
- 7Ministry of Health Republic of Indonesia National guideline for TB control 2016 Ministry of Health Republic of Indonesia Jakarta
- 8Lin P.L.Flynn J.L.Understanding latent tuberculosis: a moving target J Immunol 1852010152210.4049/jimmunol.090385620562268 PMC 3311959 · doi ↗ · pubmed ↗