Cervical Cancer Outcomes in Women With HIV in the Age of Antiretroviral Therapy
Alison K. Yoder, Rehema J. Thomas, Austin Huang, Anushka Mandalapu, Dana M. Roque, Kristina Bowles, Kevin Albuquerque, Christina Son, Michelle S. Ludwig, Kimberly Levinson, Anna E. Coghill, Elizabeth Yu Chiao, Lilie L. Lin

TL;DR
This study examines cervical cancer outcomes in HIV-positive women in the US following the introduction of antiretroviral therapy.
Contribution
The study provides insights into cervical cancer outcomes in the context of HIV and antiretroviral therapy.
Findings
The study analyzes outcomes for women with HIV and cervical cancer in the US.
It focuses on the impact of antiretroviral therapy on these outcomes.
Abstract
This cross-sectional study investigates the outcomes for women living with HIV and cervical cancer in the US after the emergence of antiretroviral therapy.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure
Figure| Characteristic | Entire cohort | Definitive chemoradiation | ||||||
|---|---|---|---|---|---|---|---|---|
| No. (%) | No. (%) | |||||||
| WWH (n = 172) | WLWH-A (n = 24) | WLWH-N (n = 38) | WWH (n = 68) | WLWH-A (n = 9) | WLWH-N (n = 9) | |||
| No. of patients | 172 | 24 | 38 | NA | 68 | 9 | 9 | NA |
| Race and ethnicity | ||||||||
| Black | 62 (36.0) | 19 (79.2) | 32 (84.2) | <.001a | 25 (36.7) | 8 (89.9) | 5 (56.6) | .05a |
| Hispanic | 39 (22.7) | 3 (12.5) | 3 (7.9) | 29 (42.6) | 1 (11.1) | 3 (33.3) | ||
| White and/or Asiana | 71 (41.3) | 2 (8.3) | 3 (7.9) | 14 (20.5) | 0 | 1 (11.1) | ||
| Smoking status | ||||||||
| Active | 58 (33.7) | 8 (33.3) | 20 (52.6) | .04 | 18 (26.5) | 1 (11.1) | 3 (33.3) | .02b |
| Never | 80 (46.5) | 11 (45.8) | 15 (39.5) | 34 (50.0) | 7 (78.8) | 6 (66.7) | ||
| Prior | 34 (19.8) | 4 (16.7) | 2 (5.3) | 16 (23.5) | 0 | 0 | ||
| Unknown | 0 | 1 (4.2) | 1 (2.6) | 0 | 1 (11.1) | 0 | ||
| Disease stage | ||||||||
| I | 58 (33.7) | 9 (37.5) | 9 (23.7) | .23b | 1 (1.5) | 0 | 0 | .99b |
| II | 22 (12.8) | 5 (20.8) | 2 (5.3) | 16 (23.5) | 2 (22.2) | 2 (22.2) | ||
| III | 87 (50.6) | 9 (37.5) | 24 (63.2) | 50 (73.5) | 7 (78.8) | 7 (77.7) | ||
| IV | 5 (2.9) | 1 (4.2) | 3 (7.9) | 1 (1.5) | 0 | 0 | ||
| Positive lymph nodes | ||||||||
| No | 99 (57.6) | 17 (70.8) | 20 (52.6) | .35b | 22 (32.3) | 4 (44.4) | 2 (22.2) | .60b |
| Yes | 73 (42.4) | 7 (29.2) | 18 (46.4) | 46 (68.7) | 5 (56.6) | 7 (77.7) | ||
| Simplified histology | ||||||||
| Adenocarcinoma/other | 30 (17.4) | 2 (8.3) | 6 (15.8) | .52b | 6 (8.8) | 0 | 1 (11.1) | .62b |
| SCC | 142 (82.6) | 22 (91.7) | 32 (84.2) | 62 (91.2) | 9 (100.0) | 8 (88.9) | ||
| Chemotherapy used | ||||||||
| No | 57 (33.1) | 11 (45.8) | 18 (47.4) | .16b | NA | NA | NA | NA |
| Yes | 115 (66.9) | 13 (54.2) | 20 (52.6) | 68 (100.0) | 9 (100.0) | 9 (100.0) | ||
| Chemotherapy cycles, median (IQR) | 5 (4-6) | 4 (1-7) | 3 (1-7) | .006c | 5 (4-6) | 4 (1-7) | 4 (1-7) | .07c |
| Treatment era | ||||||||
| 1997-2001 | 16 (9.3) | 0 (0.0) | 7 (18.4) | .11b | 1 (1.5) | 0 | 0 | .23b |
| 2000-2008 | 48 (27.9) | 6 (25.0) | 12 (31.6) | 7 (10.3) | 0 | 3 (33.3) | ||
| 2009-2017 | 108 (62.8) | 18 (75.0) | 19 (50.0) | 60 (88.2) | 9 (100.0) | 6 (66.7) | ||
| ART treatment compliance | ||||||||
| Yes | NA | 24 (100) | NA | NA | NA | 9 (100.0) | NA | NA |
| No | NA | NA | 20 (52.6) | NA | NA | NA | 6 (66.7) | NA |
| Unknown | NA | NA | 18 (47.4) | NA | NA | NA | 3 (33.3) | NA |
| Institution | ||||||||
| Baylor College of Medicine | 30 (17.4) | 5 (20.8) | 4 (10.5) | .06b | 26 (38.2) | 4 (44.4) | 3 (33.3) | .25b |
| Johns Hopkins | 72 (41.9) | 3 (12.5) | 16 (42.1) | 11 (16.2) | 0 | 1 (11.1) | ||
| University of Maryland | 12 (7.0) | 3 (12.5) | 5 (13.2) | 3 (4.4) | 0 | 0 | ||
| MD Anderson | 20 (11.6) | 3 (12.5) | 6 (15.8) | 9 (13.2) | 1 (11.1) | 1 (11.1) | ||
| Moffitt | 17 (9.9) | 6 (25.0) | 2 (5.3) | 4 (5.9) | 3 (33.3) | 0 | ||
| Southwestern | 12 (7.0) | 1 (4.2) | 5 (13.2) | 12 (17.6) | 1 (11.1) | 4 (44.4) | ||
| University of Illinois-Chicago | 9 (5.2) | 3 (12.5) | 0 | 3 (4.4) | 0 | 0 | ||
| Treatment sequence | ||||||||
| Chemotherapy and RT | 91 (52.9) | 11 (45.8) | 15 (39.5) | .14b | NA | NA | NA | NA |
| RT alone | 13 (7.6) | 2 (8.3) | 10 (26.3) | NA | NA | NA | ||
| Surgery alone | 37 (21.5) | 8 (33.3) | 6 (15.8) | NA | NA | NA | ||
| Surgery followed up RT | 7 (4.1) | 1 (4.2) | 2 (5.3) | NA | NA | NA | ||
| Surgery followed up Chemotherapy | 2 (1.2) | 0 | 0 | NA | NA | NA | ||
| Surgery followed up ChemoRT | 22 (12.8) | 2 (8.3) | 5 (13.2) | NA | NA | NA | ||
| RT dose, median (IQR) | NA | NA | NA | NA | 45 (39.6-50.4) | 45 (40.7-49.3) | 45 (42.3-47.7) | .53c |
| RT fx, median (IQR) | NA | NA | NA | NA | 25 (23-27) | 25 (24-26) | 25 (23-27) | .30c |
| Brachytherapy dose, median (IQR) | NA | NA | NA | NA | 30 (17-43) | 30 (17-43) | 29 (18-40) | .95c |
| Brachytherapy fx, median (IQR) | NA | NA | NA | NA | 2 (1-5) | 2 (1-5) | 3 (1-5) | .68c |
| Extended field RT | NA | NA | NA | NA | 35 (52) | 3 (33) | 5 (63) | .46b |
| Radiation length, median (IQR), d | NA | NA | NA | NA | 56 (40-72) | 53 (34-72) | 59 (49-69) | .12c |
| RT type | ||||||||
| 3D-conformal | NA | NA | NA | NA | 28 (41.2) | 3 (33.3) | 4 (44.4) | .88b |
| IMRT | NA | NA | NA | 33 (48.5) | 4 (44.4) | 4 (44.4) | ||
| Other or not specified | NA | NA | NA | 7 (10.3) | 2 (22.2) | 1 (11.1) | ||
| Brachytherapy type | ||||||||
| Interstitial needles | NA | NA | NA | NA | 5 (7.3) | 1 (11.1) | 0 | .50b |
| Other or not specified | NA | NA | NA | 3 (4.4) | 0 | 0 | ||
| Tandem and ring | NA | NA | NA | 1 (1.5) | 1 (11.1) | 0 | ||
| Tandem and ovoid | NA | NA | NA | 59 (86.8) | 7 (77.8) | 9 (100.0) | ||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCervical Cancer and HPV Research · Viral-associated cancers and disorders · Endometrial and Cervical Cancer Treatments
Introduction
Women living with HIV (WLWH) experience disproportionately high rates of cervical cancer.^1,2^ Whether outcomes and toxic effects are similar between WLWH and women living without HIV (WWH) in the age of highly active antiretroviral therapy (HAART) is unclear.^3,4,5,6^ Research on HIV and cervical cancer outcomes in the US is relatively scarce, with few studies examining disease progression or control. This study aims to fill this research gap.
Methods
WLWH treated for cervical cancer from January 1997 through November 2017 were included in this cross-sectional study and retrospective multi-institutional review; WLWH were matched within each institution with WWH at a 1:3 ratio; a 1:2 ratio was used when a third matched patient was unavailable (eMethods in Supplement 1). The study was approved by the MD Anderson Cancer Center institutional review board. For WLWH, patients were included if they had a positive HIV test or known HIV infection at or before cancer diagnosis. Adherence to HAART for WLWH during treatment was determined via the medical record. If adherence could not be ascertained, those patients were deemed unknown and grouped with the nonadherent patients. Cox regression survival analysis was used to assess for potential associations between HIV status and adherence to ART -exposure categories: WLWH-adherent (WLWH-A), WLWH-nonadherent (WLWH-N), or WWH— clinical variables, and local control (LC), distant metastasis-free survival (DMFS), disease-free survival (DFS) and overall survival (OS). All statistical analyses were conducted using SPSS version 25.0. Statistical significance was assessed at p < .05. This study was approved by each institution’s institutional review board and a waiver of consent was approved by each respective institution given the retrospective design in accordance with 45 CFR §46. The study followed STROBE reporting guidelines.
Results
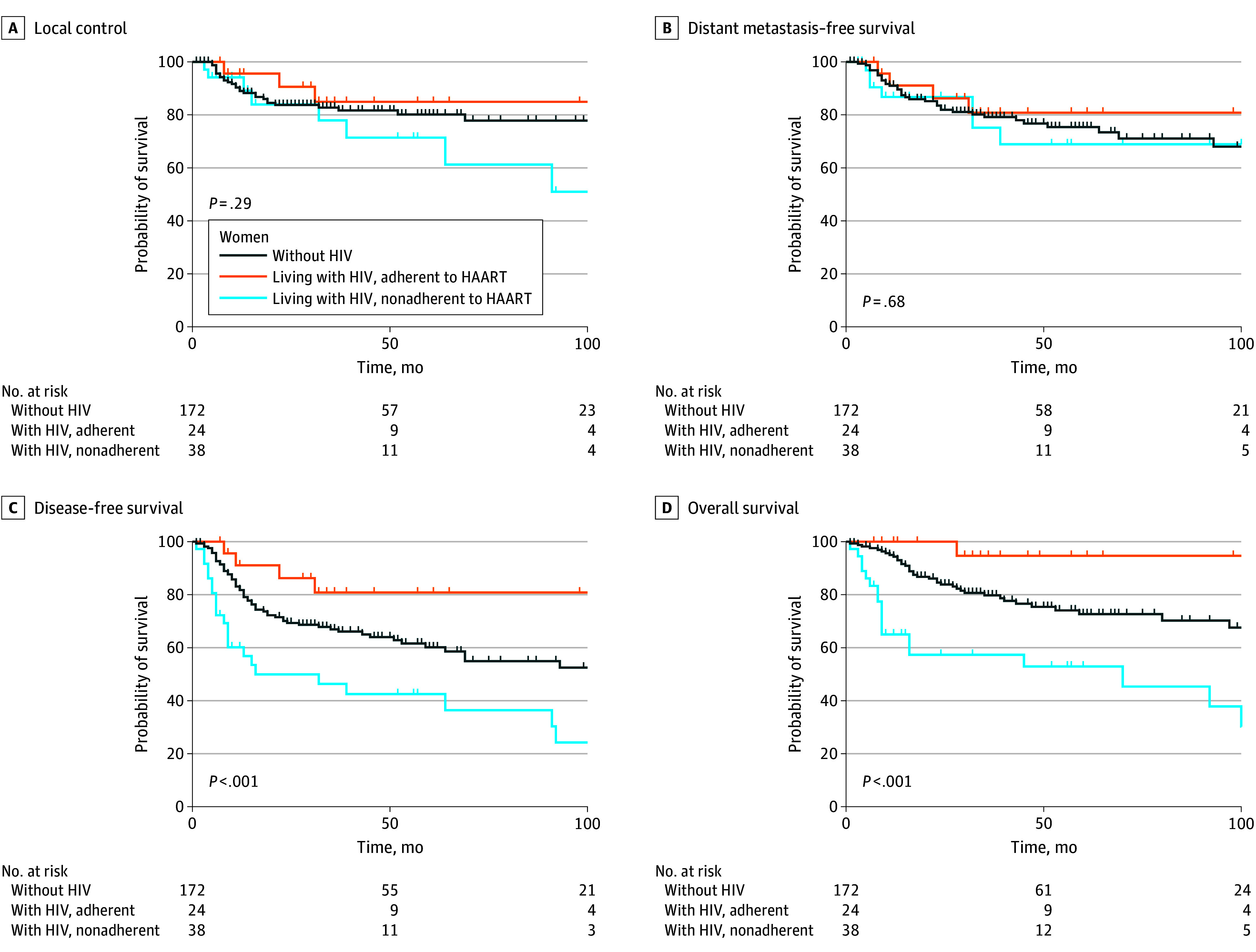
A total of 62 WLWH and 172 matched WWH with known cervical cancer, disease stage at diagnosis, and at least 1 follow-up clinical note were included (Table). Median follow-up time for the cohort was 47 months (IQR, 39-55 months). Most patients presented with stage III disease (120 patients [51%]), and (117 patients [50%]) underwent chemoradiation. Among the entire cohort, DFS and OS differed by HIV status and adherence to HAART (Figure), with worse survival for WLWH-N. More advanced disease stage and nonadherence to HAART were associated with worse OS in multivariable analysis. Similarly, among the subset of 86 patients who received definitive chemoradiotherapy, inferior OS and DFS were noted for WLWH-N. LC and DMFS were similar for both cohorts regardless of HIV status and adherence to HAART.
Kaplan-Meier Curves Comparing Local Control, Distant Metastasis-Free Survival, Disease-Free Survival, and Overall Survival for Women Without HIV (WWH), Women Living With HIV Who Adhered to Antiretroviral Therapy (WLWH-A), and WLWH Who Were Nonadherent to ART (WLWH-N)Local recurrence was defined as disease recurrence within the cervix, vagina, parametria, or regional nodes. Distant recurrence was defined as disease recurrence in another organ or nonregional lymph node. Disease-free survival was defined from the date of initial biopsy confirming cervical cancer to the date of first recurrence or last follow-up. Five-year local control rates did not differ by HIV status and adherence to ART (WWH, 80% [95% CI, 72%-86%], WLWH-A, 84% [95% CI, 60%-94%], and WLWH-N, 72% [95% CI, 45%-87%]; P = .29), and neither did DMFS (WWOH, 76% [95% CI, 67%-82%], WLWH-A, 81% [95% CI, 56%-92%], and WLWH-N, 69% [95% CI, 44%-85%]; P = .68). Five-year DFS was 60% (95% CI, 51%-68%) in WWH, 81% (95% CI, 56%-92%) in WLWH-A patients, and 43% (95% CI, 25%-59%) in WLWH-N patients (P < .001). Five-year OS was 73% (95% CI, 63%-80%) in WWH, 95% (95% CI, 69%-99%) in WLWH-A, and 53% (95% CI, 34%-69%) WLWH-N patients, respectively (P < .001). Nonadherence with ART was associated with worse DFS (WLWH-A HR, 0.41 [95% CI, 0.15-1.12]; P = .08; WLWH-N HR, 1.81 [95% CI, 1.10-2.98]; P = .02), and OS (WLWH-A HR, 0.16 [95% CI, 0.02-1.18]; P = .07; WLWH-N HR, 2.34 [95% CI, 1.32-4.15]; P = .004) on multivariate analysis.
The frequency of acute grade 3 or higher gastrointestinal or genitourinary toxic effects did not differ for WWH (n = 14,14%), WLWH-A (n = 2,13%), and WLWH-N (n = 4,19%) patients (P = .82). Similarly, among the patients who received definitive chemoradiotherapy, no significant difference was found in the frequency of acute grade 3 or higher gastrointestinal or genitourinary toxic effects between WWH (n = 11, 21%), WLWH-A v, and WLWH-N (n = 2, 40%) patients (P = .26).
Discussion
To our knowledge, this cross-sectional study is the largest to date evaluating the association of HIV infection with cervical cancer outcomes in the US. In this study, we found no statistically significant differences in outcomes between WLWH who adhered to HAART and WWH. However, WLWH-N had significantly worse DFS and OS than WLWH-A and WWH in both the entire cohort as well as in the group treated with definitive chemoradiation. No differences in gastrointestinal or genitourinary toxic effects were evident between these 2 cohorts, including in the subset of women who received chemoradiotherapy.
Limitations include the retrospective design, extension over several treatment eras, and limited patient numbers (particularly in the chemoradiation subset). Despite these limitations, this study provides valuable insights into the importance of HAART adherence during treatment for cervical cancer, which should be investigated in future studies. This is the largest cohort of WLWH treated for cervical cancer in the US and the inclusion of 7 institutions with different practice patterns also helps to reduce possible treatment bias.
In the era of HAART, WLWH diagnosed with cervical cancer should receive curative treatment per standard guidelines. The importance of adhering to HAART during treatment for cervical cancer should be stressed by oncologists to ensure that WLWH have optimal outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Kuhn L, Wang C, Tsai WY, Wright TC, Denny L. Efficacy of human papillomavirus-based screen-and-treat for cervical cancer prevention among HIV-infected women. AIDS. 2010;24(16):2553-2561. doi:10.1097/QAD.0b 013e 32833 e 163e 20706107 · doi ↗ · pubmed ↗
- 2Abraham AG, D’Souza G, Jing Y, ; North American AIDS Cohort Collaboration on Research and Design of Ie DEA. Invasive cervical cancer risk among HIV-infected women: a North American multicohort collaboration prospective study. J Acquir Immune Defic Syndr. 2013;62(4):405-413. doi:10.1097/QAI.0b 013e 31828177 d 723254153 PMC 3633634 · doi ↗ · pubmed ↗
- 3Ferreira MP, Coghill AE, Chaves CB, . Outcomes of cervical cancer among HIV-infected and HIV-uninfected women treated at the Brazilian National Institute of Cancer. AIDS. 2017;31(4):523-531. doi:10.1097/QAD.000000000000136728060014 PMC 5263104 · doi ↗ · pubmed ↗
- 4Meghani K, Puri P, Bazzett-Matabele L, . Significance of HIV status in cervical cancer patients receiving curative chemoradiation therapy, definitive radiation alone, or palliative radiation in Botswana. Cancer. 2024;130(14):2462-2471. doi:10.1002/cncr.3528938529676 · doi ↗ · pubmed ↗
- 5Dryden-Peterson S, Bvochora-Nsingo M, Suneja G, . HIV infection and survival among women with cervical cancer. J Clin Oncol. 2016;34(31):3749-3757. doi:10.1200/JCO.2016.67.961327573661 PMC 5477924 · doi ↗ · pubmed ↗
- 6Simonds HM, Wright JD, du Toit N, Neugut AI, Jacobson JS. Completion of and early response to chemoradiation among human immunodeficiency virus (HIV)-positive and HIV-negative patients with locally advanced cervical carcinoma in South Africa. Cancer. 2012;118(11):2971-2979. doi:10.1002/cncr.2663922072021 PMC 3448067 · doi ↗ · pubmed ↗