Appearance of basal cell carcinoma on untreated capillary malformation
Catalina Buchroithner, Nelson Lobos, Gabriel Neely, Arturo Madrid, Valentina Darlic, Alex Castro

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1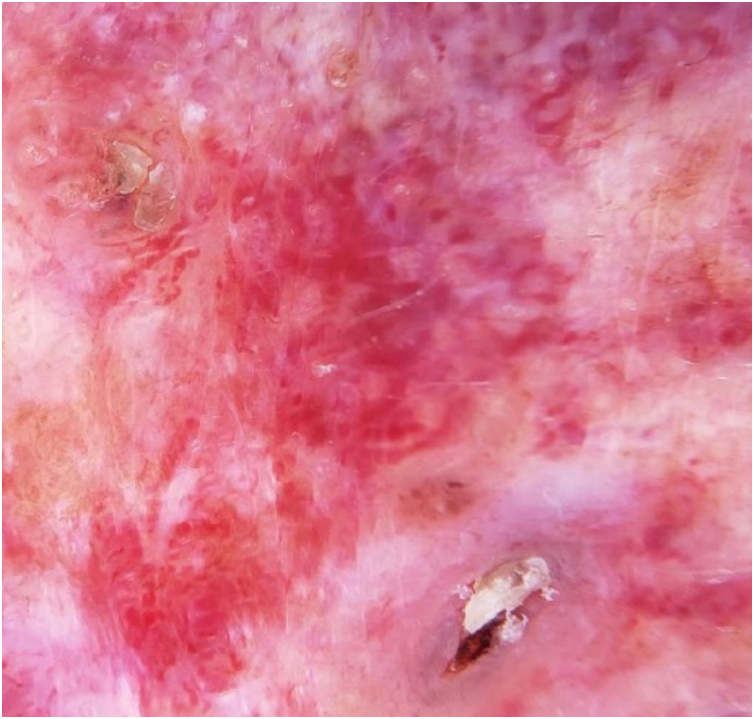 Figure 2
Figure 2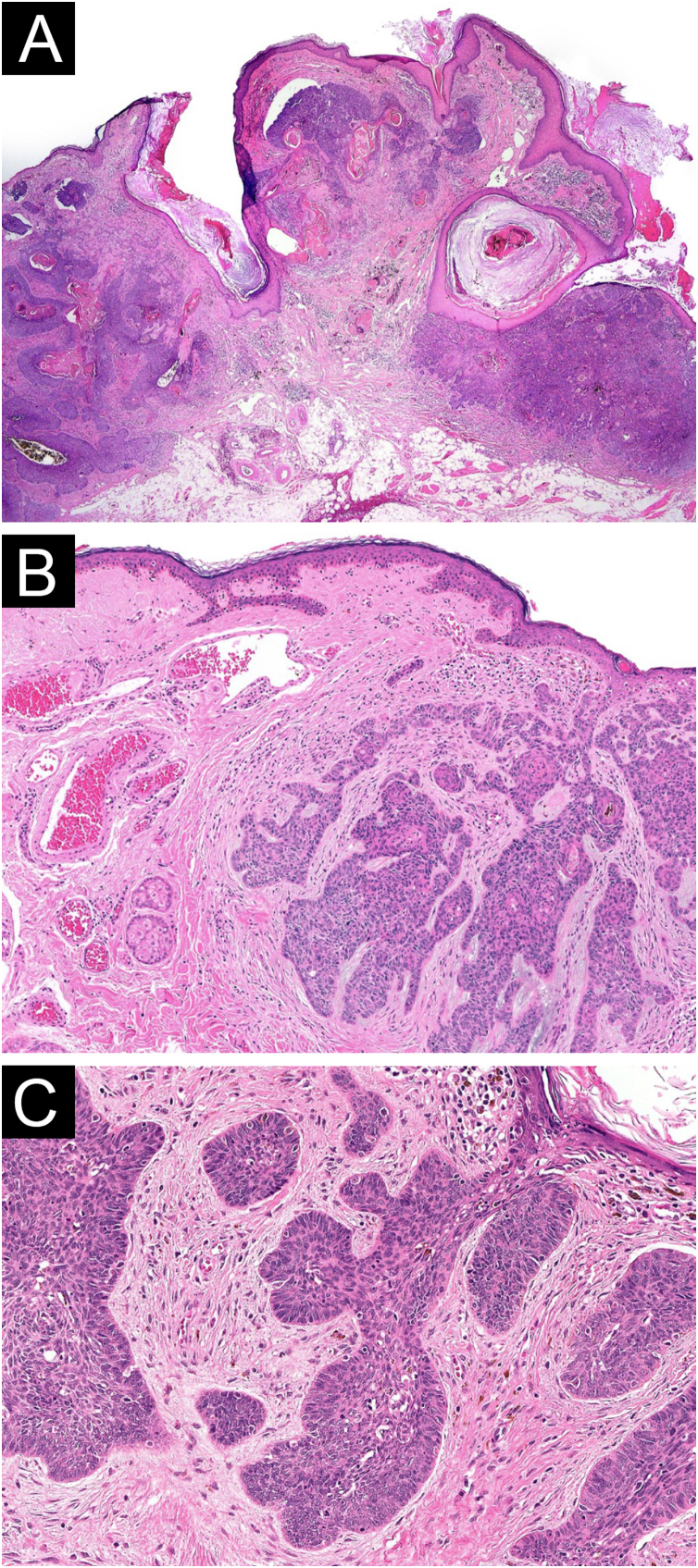 Figure 3
Figure 3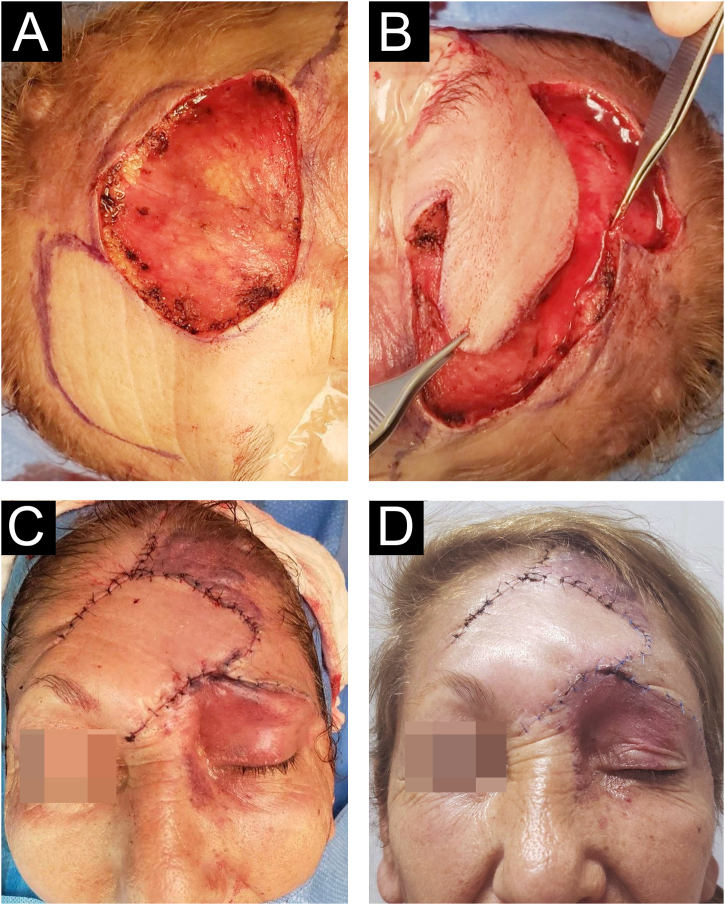 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVascular Malformations and Hemangiomas · Dermatologic Treatments and Research · Nonmelanoma Skin Cancer Studies
Dear Editor,
Capillary malformations are congenital abnormalities in the morphogenesis of capillary vessels in the skin, consisting of a network of dilated blood vessels in the superficial dermis beneath a normal epidermis. They are present in 0.1%–0.3% of infants and represent the most common congenital vascular malformation.1 The development of basal cell carcinoma (BCC) within a capillary malformation is a rare finding, and its etiology remains unclear.2
We present the case of a 62-year-old female patient with a history of a left frontal nevus flammeus following the V1 trigeminal dermatome since birth, with no prior evaluation or treatment. She reported a seven-year history of an asymptomatic, progressively enlarging lesion in the left frontal region, accompanied by the development of nodules and tumors. On physical examination, an erythematous-violaceous plaque with superficial nodules, some hyperkeratotic and tending to coalesce, was observed (Fig. 1). The lesion had a soft consistency and followed the distribution of the V1 trigeminal branch. Dermoscopy revealed an erythematous base with ectatic red vessels, presenting as linear structures with a horizontal orientation and rounded, globular structures with a vertical orientation. Additionally, some nests and blue-gray globules were noted (Fig. 2). Doppler ultrasound identified a low-flow vascular malformation with poorly defined borders in the supraciliary and left frontal region, extending to the junction with the scalp. An incisional biopsy, guided by dermoscopic demarcation, revealed superficial hyperkeratosis, an infundibulum with cystic dilation, and irregular nests of basaloid cells infiltrating into the deep reticular dermis, consistent with pigmented nodular basal cell carcinoma (Fig. 3). A Limberg flap was selected to provide broader coverage without tissue tension and to facilitate closure of the secondary defect (Fig. 4).Figure 1. Erythematous-violaceous plaque with superficial nodules, some hyperkeratotic, with a tendency to coalesce, soft consistency, following the distribution of the V1 trigeminal branch.Figure 1. Figure 2Dermoscopy image displays an erythematous base with ectatic red vessels, linear with a horizontal orientation and rounded, globular with a vertical orientation. Associated with some nests and blue-gray globules, rosettes, fibrosis, and areas resembling seborrheic keratosis.Figure 2. Figure 3Histopathology (A) Hematoxylin & eosin, ×40: Low power shows tumor composed of nests of basaloid cells. Some retraction spaces are visible between tumor islands and stroma. (B) Hematoxylin & eosin, ×100: Tumor is made of basaloid cells arranged in cords and nests. The stroma is fibrous and exhibits mucinous change. At the left, abnormal dilated dermal vessels are seen. (C) Hematoxylin & eosin, ×200: High power shows tumor nests composed of basaloid cells with oval nuclei and scant cytoplasm, forming a peripheral palisading.Figure 3. Figure 4Limberg flap was chosen to achieve greater coverage without tissue tension and to facilitate the closure of the secondary defect. (A) Primary defect. (B) Closure planning. (C) Immediate postoperative period. (D) Postoperative day 21.Figure 4
Previous therapy, particularly radiotherapy, has been proposed as a contributing factor to the development of BCCs within capillary malformations. Although this treatment approach is now obsolete for these lesions, its association with BCC has been reported in up to 75% of cases.2, 3 The first description of BCC arising in a capillary malformation was made by Scott in 1948,4 and to date, approximately 27 cases have been reported,5 of which only six occurred in untreated capillary malformations.2, 6 It has been suggested that the production of an oncogenic factor by the underlying static vessels may render the epidermis more susceptible to ultraviolet or ionizing radiation.2
In conclusion, we report a case of BCC arising within an untreated facial capillary malformation, an association that has been rarely documented and poses a diagnostic challenge. Dermoscopy plays a crucial role in highlighting vascular and pigmented features suggestive of basal cell carcinoma, particularly in this context. However, further studies are needed to determine the presence of local factors that may contribute to the development of these tumors within a capillary malformation.
Financial support
None declared.
Author's contributions
Catalina Buchroithner: Approval of the final version of the manuscript; critical literature review; manuscript critical review; preparation and writing of the manuscript.
Nelson Lobos: Approval of the final version of the manuscript; critical literature review; manuscript critical review; preparation and writing of the manuscript.
Gabriel Neely: Critical literature review; manuscript critical review; preparation and writing of the manuscript.
Arturo Madrid: Critical literature review; manuscript critical review; preparation and writing of the manuscript.
Valentina Darlic: Critical literature review; manuscript critical review; preparation and writing of the manuscript.
Alex Castro: Critical literature review; manuscript critical review; preparation and writing of the manuscript.
Conflicts of interest
None declared.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Faurshou A.Laser or light sources for treating port-wine stains (Review)Cochrane Database Syst Rev.2011 CD 00715210.1002/14651858.CD 007152.pub 222071834 · doi ↗ · pubmed ↗
- 2Fujita M.Tanizaki H.Tanioka M.Kabashima K.Miyachi Y.Basal cell carcinoma arising within port-wine stains with no preceding radiotherapy J Dermatol 421020151007100810.1111/1346-8138.1299526118702 · doi ↗ · pubmed ↗
- 3Lapidoth M.Ad-El D.David M.Alcalay J.Azaria R.Basal cell carcinoma arising over facial port wine stain: a single centre experience J Eur Acad Dermatol Venereol.202006106610691698725910.1111/j.1468-3083.2006.01701.x · doi ↗ · pubmed ↗
- 4Scott I.M.Basal cell epithelioma on the site of an angioma Br J Dermatol Syph.601948697018905001 · pubmed ↗
- 5Kaune K.M.Haas E.Buhl T.Schön M.P.Zutt M.Multiple basal cell carcinomas arising in radiotherapy-treated nevus flammeus: early detection facilitated by 595-nm pulsed dye laser Eur J Dermatol.2020105102040379810.1684/ejd.2010.0956 · doi ↗ · pubmed ↗
- 6Hackett C.B.Langtry J.A.A.Basal cell carcinoma of the ala nasi arising in a port wine stain treated using mohs micrographic surgery and local flap reconstruction Dermatol Surg.4020145905922445632410.1111/dsu.12442 · doi ↗ · pubmed ↗